
Abstract
Purpose:
Dislocation is a major complication after total hip arthroplasty (THA), and pelvic stiffness is reportedly a significant risk factor for dislocation. This study aimed to investigate spinopelvic alignment, and identify preoperative factors associated with postoperative pelvic mobility.
Methods:
We enrolled 78 THA patients with unilateral osteoarthritis. The sagittal spinopelvic alignment in the standing and sitting position was measured using an EOS imaging system before and 3 months after THA. We evaluated postoperative pelvic mobility, and defined cases with less than 10° of sacral slope change as pelvic stiff type. The preoperative characteristics of those with postoperative stiff type, and preoperative factors associated with risk of postoperative stiff type were evaluated.
Results:
Sagittal spinopelvic alignment except for lumbar alignment were significantly changed after THA.A total of 13 patients (17%) were identified as postoperative pelvic stiff type. Preoperative lower pelvic and lumbar mobility were determined as significant factors for prediction of postoperative pelvic stiff type. Among these patients, nine patients (69%) did not have pelvic stiffness before THA. Preoperative factor associated with the risk of postoperative pelvic stiff type in those without preoperative stiffness was lower lumbar lordosis in standing position by multivariate regression analysis.
Conclusion:
Spinopelvic alignments except lumber alignment was significantly changed after THA. The lower pelvic mobility and lumbar alignment were identified as the preoperative predictive factors for postoperative pelvic mobility. Evaluation of preoperative lumbar alignment may be especially useful for the prediction in patients with hip contractures, for these patients may possibly experience the extensive perioperative change in pelvic mobility.
Introduction
Total hip arthroplasty (THA) is an effective procedure to treat osteoarthritis of the hip. Dislocation is a major complication after THA, and may result in clinical failure requiring revision surgery. Preoperative planning for THA generally uses the pelvic tilt angle in the supine position. 1,2 The sagittal pelvic tilt, however, changes during postural changes, and sagittal pelvic tilt changes in turn affect the functional cup angle, with a 1° posterior pelvic tilt increasing cup anteversion by 0.7°. 3 In fact, dislocation has occurred in patients with a cup implanted in the Lewinnek safe zone, and sagittal pelvic tilt changes during postural changes (pelvic mobility) has been reported as the cause. 4 –7
In most patients, the pelvis tilts posteriorly during postural change from the standing to sitting position. There is increased anteversion of the acetabulum, and this decreases the risk of anterior impingement. 8 In some patients, however, the pelvis does not tilt posteriorly during the aforementioned postural change and the acetabulum cannot antevert, risking impingement and dislocation. Cases with less than 10° change in sacral slope (SS) during postural change from standing to sitting has been reported as a stiff type, and in such cases, there is increased risk of posterior dislocation with anterior impingement in the sitting position. 9 Hence, pelvic mobility affects the risk of impingement and dislocation, however, it remains unclear what preoperative factors influence postoperative pelvic mobility, and whether preoperative pelvic mobility can be used to predict postoperative pelvic mobility. Furthermore, there have been few reports on the characteristics of whole-spinal and pelvic alignment in such patients with stiff type.
This study, therefore, aimed to investigate whole-spinal and pelvic alignment in the standing and sitting position in THA patients, and identify the preoperative factors associated with postoperative pelvic mobility and the risk factors for postoperative stiff type.
Materials and methods
Patients
Of the 446 hips of patients who underwent primary THA from December 2014 to October 2018 at our institution, we enrolled the patients with unilateral osteoarthritis in this study. The patients with bilateral osteoarthritis of the hip, osteonecrosis of the femoral head, rheumatoid arthritis, and who have difficulty in maintaining the standing position for EOS imaging (EOS Imaging company, Paris, France) were excluded from this study. A total of 78 patients were finally evaluated. Patients consisted of 18 males and 60 females with an average age of 63 years (range: 40–86 years) and average Body Mass Index (BMI) of 24 kg/m2 (range 19–35 kg/m2) (Table 1). A total of 71 patients were treated using a modified mini-incision direct lateral approach, and seven using an anterolateral approach 10 (Table 1). There were no dislocations within at least one year of follow up.
Patient demographic data in this study.

BMI, body mass index.
Spinopelvic alignment parameters
The sagittal spinopelvic alignment in the standing and sitting position was measured using an EOS imaging system before and 3 months after THA. Patients were positioned in a relaxed position with hands on the clavicles in the standing and sitting position. In the sitting position, the knees were bent at 90°, and both feet rested flat on the floor (Figure 1).
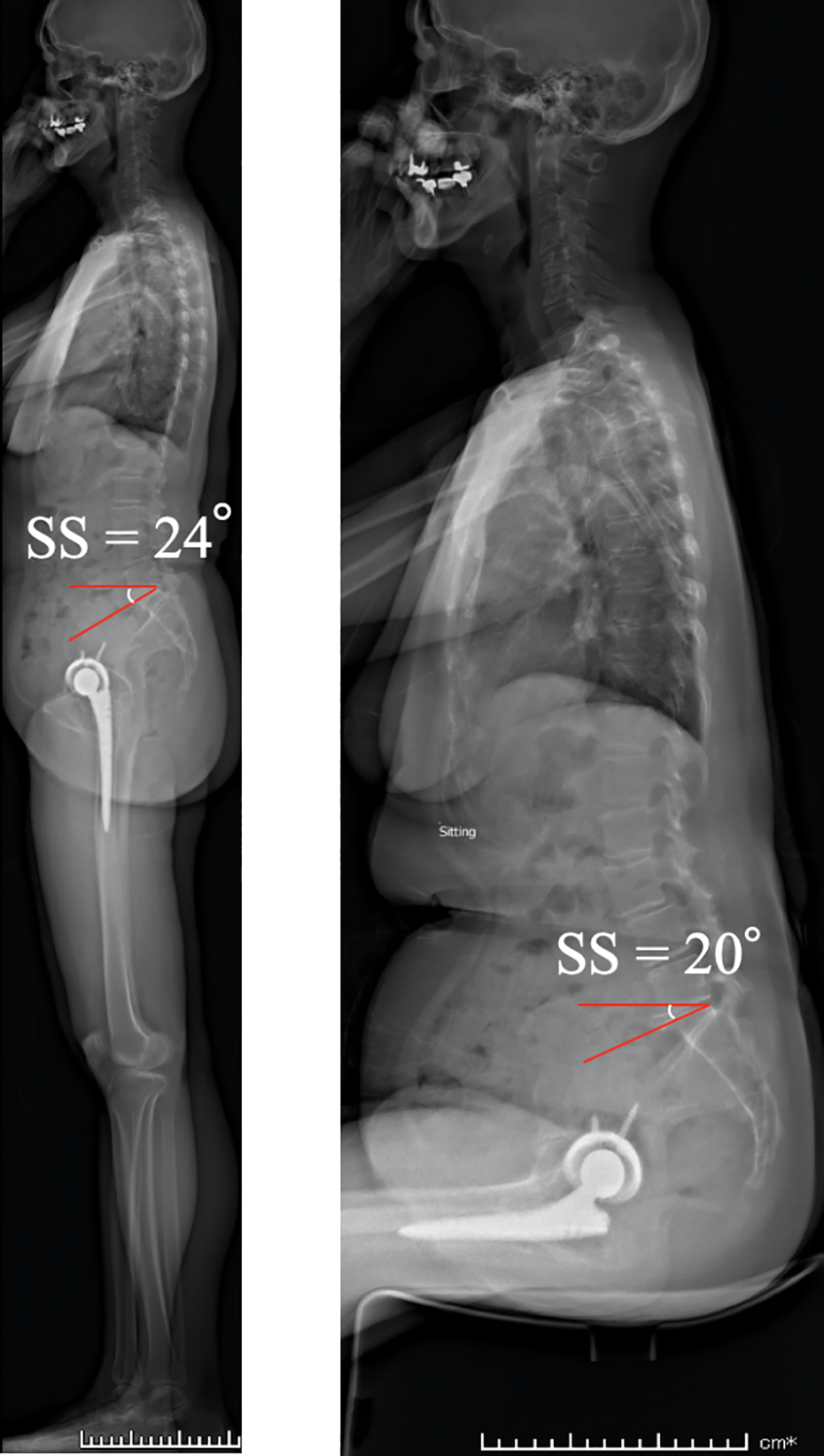
We evaluated sagittal spinopelvic alignment using an EOS imaging system. The ΔSS was four degrees in this case, and identified as a case with stiff type.
To investigate the spinopelvic alignment, lumbar lordosis (LL), T4/T12 angle, sagittal vertical axis (SVA), pelvic incidence (PI) and SS in the standing and sitting position were evaluated.
LL was defined as the angle between the superior L1 endplate and S1 endplate;T4/T12 kyphosis angle was defined as the angle between the superior T4 endplate and the lower T12 endplate in the sagittal plane; SVA was defined as the distance between the posterior edge of the sacral plate and the vertical axis passing through the center of the C7 vertebra in the sagittal plane. PI was defined as the angle between the line connecting the midpoint of the sacral plate to the center of the femoral head. PI value does not change during postural change 11 ; SS was defined as the angle between the sacral plate and the horizontal axis. The SS was regarded as the anatomic plane of the sagittal pelvic tilt in this study. A large value of SS indicates anterior pelvic tilt, and a small value of SS indicates posterior pelvic tilt.
Classification of pelvic mobility
The differences between the SS in the standing and sitting position (ΔSS) was used as a measurement of pelvic mobility (Figure 1). Cases with less than 10° ΔSS were defined as stiff type, and 10–30° were defined as normal type, and over 30° were defined as hypermobile type according to a previous study. 9 The preoperative characteristics of each group were investigated. Furthermore, preoperative factors associated with postoperative ΔSS and the risk for postoperative stiff type was evaluated by univariate and multivariate regression analysis.
Statistical analysis
The Student’s t-tests or Mann-Whitney U test were performed to compare continuous variables between two groups. The three groups (stiff, normal and hypermobile groups) were compared using one-way analysis of variance (ANOVA) with Tukey-Kramer after ANOVA to observe the significance difference between groups(continuous variables), and the Chi-square test with residual analysis after Chi-square test to observe the significance difference between groups (categorical variables). Preoperative factors associated with the postoperative ΔSS and risk for the postoperative stiff type were evaluated by logistic regression analysis. Patients factors included age, gender and BMI. Baseline variables with p-value < 0.05 in univariate regression analysis were included in the multivariate regression analysis. A p-value < 0.05 was considered to indicate statistical significance.
Results
Spinopelvic alignment
The mean SS in standing changed significantly after THA (mean ±standard deviation [SD]; 38° ± 8.7° preoperatively versus 36° ± 10° postoperatively, p = 0.0018, Table 2), but not in sitting (mean ± SD; 15° ± 14° preoperatively versus 15° ± 12°postoperatively, p = 0.40, Table 2). The mean ΔSS significantly decreased after THA (mean ± SD; 23° ± 13° preoperatively versus 20° ± 11°postoperatively, p = 0.042, Table 2).
Pre- and postoperative spinopelvic alignment.

Δ differences between the standing and sitting position measurements.
#Student’s t-tests, significantly changed after THA (p < 0.05).
*Student’s t-tests, significantly changed during postural change (p < 0.05).
SD, standard deviation; SS, sacral slope; LL, lumbar lordosis; SVA, sagittal vertical axis; THA, total hip arthroplasty.
The mean T4/T12 angle in standing changed significantly after THA (mean ± SD; 29° ± 11° preoperatively versus 30° ± 13° postoperatively, p = 0.0058, Table 2), but not in sitting (mean ± SD; 28° ± 12° preoperatively versus 27° ± 12° postoperatively, p = 0.46, Table 2). The mean LL in standing and sitting had no significant change after THA (standing: mean ± SD; 46° ± 14° preoperatively versus 46° ± 14° postoperatively, p = 0.27, sitting: mean ± SD; 20° ± 14° preoperatively versus 19° ± 14° postoperatively, p = 0.22, Table 2). The mean SVA in standing changed significantly after THA (mean ± SD; 41 mm ± 39 mm preoperatively versus 34 mm ± 40 mm postoperatively, p = 0.016, Table 2), but not in sitting (mean ± SD; 71 mm ± 23 mm preoperatively versus 70 mm ± 27 mm postoperatively, p = 0.43, Table 2).
The pre- and postoperative mean T4/T12 angle, LL and SVA changed significantly during postural change (T4/T12: preoperative; p = 0.041, postoperative; p < 0.001, LL: preoperative; p < 0.001, postoperative; p<0.001, SVA: preoperative; p < 0.001, postoperative; p < 0.001, Table 2).
Preoperative characteristics of the postoperative stiff, normal and hypermobile types
Table 3 shows the preoperative characteristics of patients with postoperative stiff, normal and hypermobile type. A total of 55 (71%) were postoperative normal, 13 (17%) were stiff and 10 (13%) were hypermobile. Those with postoperative stiff type consisted of four (31%) with preoperative stiff type, eight (62%) with preoperative normal type and one (7.7%) with preoperative hypermobile type (Table 3). A total of nine patients (14%) with preoperative normal or hypermobile type had postoperative stiff type (Table 3).
Comparison of preoperative characteristics of patients with postoperative stiff, normal and hypermobile type.

Δ differences between the standing and sitting position measurements.
* Analysis of variance (ANOVA) with Tukey-Kramer, p < 0.05.
#Chi-square test with residual analysis, p < 0.05.
SD, standard deviation;SS, sacral slope; ANOVA, analysis of variance; BMI, body mass index; LL, lumbar lordosis; SVA, sagittal vertical axis; PI, pelvic incidence.
The preoperative SS in sitting in those with postoperative hypermobile type was significantly lower than that of those with postoperative stiff and normal type (normal versus hypermobile: mean ± SD; 16° ± 12° versus 1.8° ± 18°, p = 0.0077, and stiff versus hypermobile: mean ± SD; 21° ± 12° versus 1.8° ± 18°, p = 0.0028, Table 3). The preoperative ΔSS in those with postoperative hypermobile type was larger than that of those with postoperative stiff and normal type (normal versus hypermobile: mean ± SD; 23° ± 12° versus 35° ± 12°, p = 0.0099, and stiff versus hypermobile: mean ± SD; 15° ± 11° versus 35° ± 12°, p < 0.001, Table 3). The preoperative ΔLL in those with postoperative stiff type was lower than that of those with postoperative normal and hypermobile type (stiff versus normal: mean ± SD; 13° ± 10° versus 27° ± 17°, p = 0.029, and stiff versus hypermobile: mean ± SD; 13° ± 10° versus 32° ± 15°, p = 0.026, Table 3).
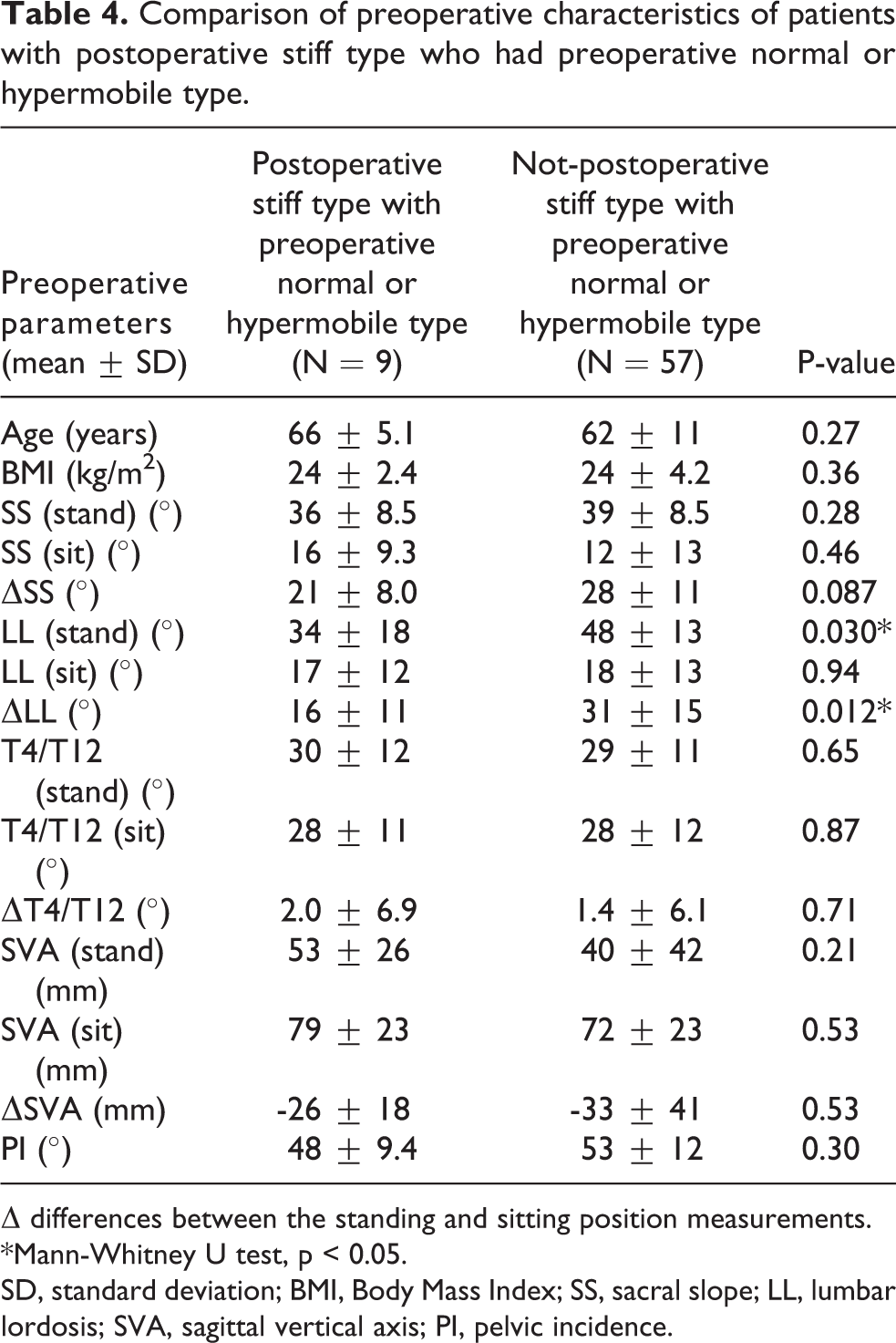
Among the patients with preoperative normal or hypermobile type, the preoperative LL in standing and ΔLL in those with postoperative stiff type were significantly lower compared to those with postoperative normal or hypermobile type (LL in standing: post-stiff versus not post-stiff; 34° ± 18° versus 48° ± 13°, p = 0.030 and ΔLL: post-stiff versus not post-stiff; 16° ± 11° versus 31° ± 15°, p = 0.012, Table 4).
Comparison of preoperative characteristics of patients with postoperative stiff type who had preoperative normal or hypermobile type.
Δ differences between the standing and sitting position measurements.
*Mann-Whitney U test, p < 0.05.
SD, standard deviation; BMI, Body Mass Index; SS, sacral slope; LL, lumbar lordosis; SVA, sagittal vertical axis; PI, pelvic incidence.
Correlation between preoperative spinopelvic alignment and postoperative pelvic mobility
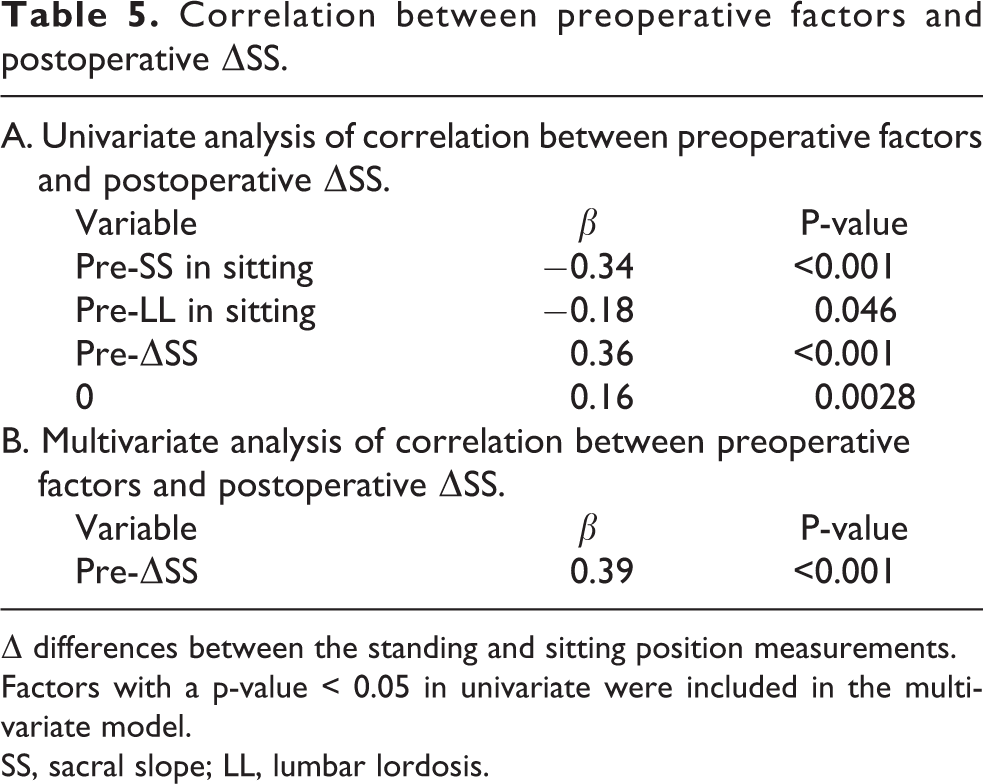
To predict the postoperative ΔSS, univariate and multivariate regression analyses were performed with variables including patient background (gender, age, BMI) and preoperative spinopelvic alignment in the standing and sitting position. Univariate analysis identified preoperative SS in sitting (β = -0.34, p < 0.001, Table 5), LL in sitting (β = -0.18, p = 0.046, Table 5), ΔSS (β = 0.36, p < 0.001, Table 5) and ΔLL (β = 0.16, p = 0.0028, Table 5) as the preoperative factors to predict the postoperative ΔSS. Multivariate analysis identified the preoperative ΔSS as the preoperative factor to predict the postoperative ΔSS (β = 0.39, p < 0.001, Table 5).
Correlation between preoperative factors and postoperative ΔSS.
Δ differences between the standing and sitting position measurements.
Factors with a p-value < 0.05 in univariate were included in the multivariate model.
SS, sacral slope; LL, lumbar lordosis.
Preoperative risk factors for the postoperative stiff type
We identified a total of 13 cases (17%) with postoperative stiff type. The preoperative factors associated with the risk for postoperative stiff type were preoperative lower ΔSS(Odds ratio = 0.94, 95% confidence interval [CI] = 0.89–0.99, p = 0.022, Table 6) and ΔLL (Odds ratio = 0.95, CI = 0.91–0.99, p = 0.025, Table 6) by univariate regression analysis. Multivariate analysis identified preoperative lower ΔSS as the risk factor for postoperative stiff type (odds ratio = 0.94, CI = 0.89–0.99, p = 0.023, Table 6).
Risk factors for postoperative stiff type.

Δ differences between the standing and sitting position measurements.
Factors with a p-value < 0.05 in univariate were included in the multivariate model.
SS, sacral slope; LL, lumbar lordosis.
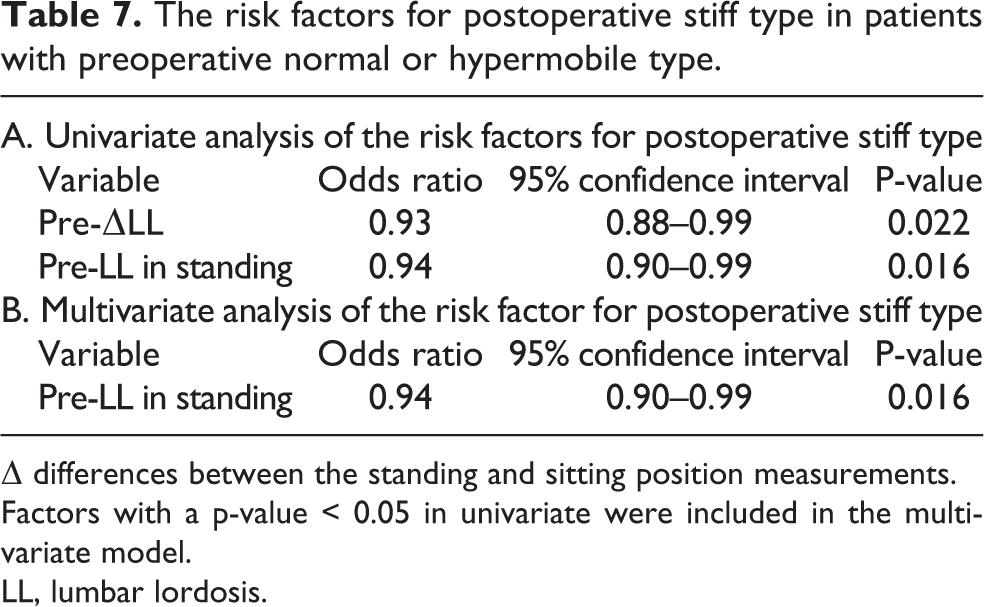
In addition, we evaluated a total of nine patients with postoperative stiff type who had preoperative normal or hypermobile type. The preoperative factors associated with the risk for postoperative stiff type in those with preoperative normal or hypermobile type were lower ΔLL(Odds ratio = 0.93, CI = 0.88–0.99, p = 0.022, Table 7) and LL in standing (Odds ratio = 0.94, CI = 0.90–0.99, p = 0.016, Table 6) by univariate regression analysis. Multivariate analysis identified preoperative lower LL in standing as the risk factor for postoperative stiff type in those with preoperative normal or hypermobile type(Odds ratio = 0.94, CI = 0.90–0.99, p = 0.016, Table 7).
The risk factors for postoperative stiff type in patients with preoperative normal or hypermobile type.
Δ differences between the standing and sitting position measurements.
Factors with a p-value < 0.05 in univariate were included in the multivariate model.
LL, lumbar lordosis.
Discussion
Improvement of hip mobility is important for improved daily activity in THA patients, although this increases the implant impingement risk that may cause dislocation. Accurate cup and stem positioning can achieve a maximized and stable range of motion without increasing implant impingement risk. 12 Dislocation, however, has occurred in patients with theoretically accurate implant position, and pelvic mobility has been reported as an important factor for hip dislocation. 4,7 Therefore, adjustment to the angle of the acetabular and femoral implant may be needed depending on the patient’s pelvic mobility. 13 As patients with stiff pelvic mobility may require higher coronal inclination and anteversion for minimizing posterior dislocation, 13 preoperative prediction of postoperative pelvic stiffness is important in THA.
Stiffness in pelvic mobility, reportedly a significant risk factor for dislocation in THA patients, can be predicted by preoperative patient characteristics. Although several previous reports demonstrated a correlation between sagittal lumbar alignment and sagittal pelvic alignment, no study has investigated the association of whole-spinal alignment on pelvic mobility. Whole-spinal alignment represents the patient’s posture and may be useful for predicting pelvic stiffness. Therefore, the present study investigated the change of whole-spinal alignment before and after THA and evaluated whole-spinal alignment association with pelvic mobility.
Investigation of whole-spinal alignment demonstrated a significant postoperative change in sagittal balance (SVA) and thoracic alignment (T4/12) as well as pelvic alignment (SS), however, the lumber alignment (LL) was unchanged in both standing and sitting position before and after THA, indicating that lumbar alignment is less affected by THA compared with other sagittal alignment. Similar to previous reports, our patients experienced a significant reduction of pelvic mobility from standing to sitting after THA as represented by decrease of ΔSS. 9,14 This may be because improvement of hip contracture from THA improved hip mobility while reducing pelvic mobility.
A previous study reported that preoperative pelvic mobility was a useful parameter to predict postoperative pelvic mobility and the risk of dislocation. 15 Our study also demonstrated that preoperative ΔSS is associated with postoperative ΔSS and preoperative lower ΔSS is a risk for postoperative stiff type. However, in severe hip osteoarthritis patients, the strong hip contracture may affect the prediction of the extensive change of perioperative pelvic alignment. In the current study, we encountered significant changes in perioperative ΔSS in nine patients who had preoperatively normal or hypermobile pelvic mobility but showed stiff pelvic mobility after THA. In our population, the preoperative LL in standing position and lumbar mobility were determined as useful factors for the prediction of postoperative pelvic mobility, especially in patients who had preoperatively normal or hypermobile pelvic mobility.
Previous studies reported that the risk of dislocation was high in patients with lower lumbar mobility. 16 –18 Berliner et al. also reported that THA patients with lumbar degenerative disc disease showed little change in spinopelvic alignment from a standing to a sitting position. 14 Thus, preoperative lumbar mobility influences postoperative pelvic mobility. This is because in patients with lower lumbar mobility, the pelvis, which is connected to the lumbar by the lumbosacral joint, also became less mobile. Furthermore, lumbar alignment was not affected by THA in this study, and the assessment of low lumbar mobility may be useful to predict the risk for postoperative stiff type and subsequent hip dislocation, especially in hip osteoarthritis patients with severe hip contracture.
Therefore, preoperative standing and sitting X-rays or EOS imaging system should be taken to evaluate the pelvic and lumbar alignment, and to predict the postoperative pelvic mobility and risk of dislocation. For patients with stiff pelvic mobility, the acetabular cup requires more coronal tilt and anteversion, and that the use of a dual mobility cup should be considered. 13
This study has several limitations. First, only one radiation technologist measured the alignment in the present study and the accuracy of measurements was not evaluated. However, another study has reported excellent reliability of the EOS imaging system for measuring spinopelvic alignment. 14 Second, this study evaluated the parameters three months after THA, which was fairly short-term. Several studies have reported that sagittal pelvic tilt changes over time, 19,20 therefore, a further long-term study should be performed. In contrast, dislocation often occurs early in the first few postoperative months, 21,22 thus early postoperative evaluation is also important. Third, we excluded patients with bilateral osteoarthritis because spinopelvic alignment may be affected by contralateral osteoarthritis 23 : this may contribute to result bias. Fourth, the surgical approach, type of implant and other surgical factors were not evaluated in our study that might influence our result.
Conclusion
Our study demonstrated the perioperative change in spinopelvic alignment except lumber alignment in THA patients. In these spinopelvic parameters, the pelvic mobility and lumbar alignment were identified as the preoperative predictive factors for postoperative pelvic mobility. Evaluation of preoperative lumber alignment may be especially useful for the prediction in patients with hip contractures, because these patients possibly experience the extensive perioperative change in pelvic mobility.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article.