
Abstract
Background:
Arthroscopic repair of post-traumatic meniscal lesion is one of the most common procedures in the orthopedics. Although algorithm of the treatment of meniscal lesion, this procedure is rarely discussed in combination with smoking as a risk factor for the meniscal healing.
Purpose:
The aim of this study was to assess the knee function, and the amount of time needed to return to daily and sport activities after the non-bucket-handle meniscal outside-in repair depending on Tobacco use.
Methods:
Retrospective chart review identified 99 patients after isolated outside-in meniscal repair within a series of 292 consecutive patients who underwent meniscus repair during a 3 years period. Ninety-two patients were available for follow-up and were divided into smokers and non-smokers group. Demographic data were collected from their medical records which included: age and body mass index, gender, side of index knee, duration of symptoms prior to surgery, meniscal involvement. At the time of the minimum 2 years follow-up examination: KOOS, time of the return to daily activities, time of the return to sport activities, and Tegner scale were collected.
Results:
The smoking and non-smoking groups were similar in age, sex, BMI, side, meniscus involved, Tegner scale, and duration of symptoms. Smokers population was 3.5 years older on average. The knee function was significantly better in non-smokers group with average KOOS score 80.2 vs 67.4 in smokers group. In smokers population delayed time of return to daily activities (5.4 vs 4.2 months) and prolonged time of the return to sport activities (9.4 vs 7.6 months) were observed.
Conclusions:
Smoking is associated with significantly prolonged time of the return to daily and sport activities and decreased knee function after meniscus repair with outside-in technique. Level of evidence: III
Introduction
Smoking is known to be one of the most burning issues of modern medicine that significantly affects public health, as well as increases the expenditure on patient treatment and prolongs individual stay in the hospital. 1 –3 Tobacco exposure is known to affect every organ of the body and cause its immediate damage. 1 Smoking has a multifactorial impact on the soft tissue microenvironment and healing, causing a temporary reduction in tissue perfusion and oxygenation, 4 attenuation of reparative cell functions, 5 decrease of the synthesis and deposition of collagen, 6 and impairment of the inflammation and proliferation phase of the healing process. 7
An increased amount of evidence is emerging from different areas of medicine, including orthopedic surgery field. 3,8,9 General risks of perioperative orthopedic complications like impaired wound healing, delayed fracture union and often worst procedure results are universally known but applying risks connected with smoking to a specific procedure is often represented with a low level of accuracy. 3,10
One of the procedures rarely discussed in combination with smoking is meniscus repair procedure and its implications on patients who are smokers versus non-smoking individuals. 11 –16 Although algorithm of the treatment of meniscal lesion is well established, 17,18 and repair of post-traumatic meniscal lesion is one of the most performed surgeries in the orthopedics, the amount of evidence highlighting post-surgical risks for Tobacco users from the rest of population and differentiating postoperative quality of life between those two groups of patients is strikingly low. 11,15,16,19
The primary aim of this retrospective study was to assess the knee function in the midterm, the amount of time needed to return to daily and sport activities after the non-bucket handle meniscal repair depending on Tobacco use.
Methods
Participants
A retrospective cohort study was approved by our local University’s Ethical Board to assess the knee function of patients who underwent a non-bucket handle meniscus repair. A medical chart review was performed to identify all patients undergoing a non-bucket handle meniscus repair between January 2015 and December 2017. A search across surgical database was conducted utilizing the ICD 9 codes: 80.26, 81.47 and 81.969 to find patients who had undergone an arthroscopic meniscus repair, which resulted in a list of 384 patients from three different orthopedic surgeons. Patients were then identified based on a review of the operative reports, to confirm a diagnosis of meniscus repair at the time of knee arthroscopy. The inclusion criteria consisted of a minimum age of 18 and a maximum age of 45 at the time of surgery, BMI below 35, stable knee, a confirmed traumatic isolated meniscus tear without chondral injury, treated with outside-in technique, and at least 2 years of initial postoperative follow-up. Patients who were previously treated to index knee with meniscectomy or previous meniscal repairs for their tears were excluded from the analysis. Patients who had a return of mechanical symptoms of the unstable meniscus after repair within 12 months and required surgery were classified as primary failures, and the number of failures was reported for each group. This review resulted in a total of 92 patients for our retrospective study. We then separated the smoking patients from the non-smoking patients at the time of surgery. Smoking was defined as a minimum of 10 cigarettes a day for a minimum 6 months period before the procedure.
After patients were identified, demographic data were collected from their medical records which included: age and body mass index (BMI) at the time of surgery, gender, side of index knee, duration of symptoms prior to surgery, medial or lateral meniscal involvement.
At the time of the follow-up examination, patients were contacted by mail and data like KOOS, time of the return to daily activities, time of the return to sport activities, current smoking habits and levels of sport activities (Tegner scale) were collected.
Surgical procedure
The patient was brought to the operating room and was then administered spinal anesthesia with antibiotic prophylaxis and placed in a supine position. Each surgeon used the same surgical repair technique of the meniscal pathology. The torn meniscus was first debrided and scarified with 3.5 mm full-radius motorized shaver (Dyonics; Smith & Nephew, Andover, MA, USA) to produce bleeding at the site of injury. Then meniscus was repaired with multiple outside-in sutures Monoplus No. 1 (B. Braun Melsungen AG, Germany) approximating the tear surfaces. Suture materials were advanced through the spinal needles 1.2 × 90 mm (Becton, Dickinson U.K. Limited, Berkshire, UK). With this method, a suture can be oriented in a vertical or horizontal fashion, thus providing adequate contact between torn surfaces. The same procedure was repeated as often as necessary to perform the stable meniscal repair. An approximately 1-cm skin incision was made in the region corresponding to a meniscal tear. Both sutures ends tightened to adequately tension the reduced meniscus without any soft tissue interposition via direct arthroscopic visualization, and the first knot is made tightly.
Additional Fast-fix (Smith&Nephew, Andover, MA, USA) fixation of the posterior horn was applied in four cases (one smoker/three non-smokers) when outside-in repair was not technically possible. Tension and quality of repair were checked with a probe via arthroscopic visualization. The wounds were closed and a compressive bandage was applied, and patients left the hospital the next day. The compressive bandage was removed 2 days postoperatively.
Postoperative treatment
The patients were provided with the same standard rehabilitation program. The patient’s knee was initially placed in a knee brace with restricted a range of motion to 0–30° for 2 weeks, 0–60° for the next 2 weeks, and after 4 weeks the brace was taken off. The patient was instructed to weight-bear as tolerated immediately postoperatively with the knee secured with the brace. During this time isometric muscles exercises were allowed. A closed chain strengthening exercise program was initiated 4 weeks after the surgery. After 2 weeks closed chain strengthening exercises were replaced by open chain strengthening exercises. Straight-line jogging was started 8 weeks after surgery with an increase in the pace of running. A progressive core-strengthening program with ball work, side to side movement was introduced 8 weeks postoperatively with a gradual return to activity.
Clinical scales
Knee Injury and Osteoarthritis Outcome Score (KOOS). The KOOS is a self-administered knee-specific questionnaire containing five-item Likert scales. The KOOS covers five patient-relevant dimensions: pain, other symptoms, activities of daily living (ADL), function in sports and recreation (Sports/Rec), and knee-related quality of life (QOL). 20 The validated Polish version of the KOOS was used. 21
The Tegner Activity Scale is a rating score from 0 to 10 with each particular numerical value representing a different level of physical activity, with higher scores relating to more intense physical activity and lower scores representing more sedentary activities, and was constructed as complement to the functional score of the knee joint. 22
Approval from the Ethical Board at our local University was obtained for the study design and to acquire data from medical records for this study and informed consent was obtained from all participants.
Statistical methods
For statistical analyses, to describe our study population, means and dispersion values were calculated for both groups characteristics. Shapiro–Wilk goodness-of-fit tests for Caucassian data distribution were performed and confirmed normality of the data. Single-variable analyses for all continuous variables (clinical scales) between the smoker and non-smoker groups were performed using T-test. The significance of the correlation between variables was assessed using Pearson correlation. Chi-square test. The sample size calculation showed that with a power of 80% (two-sided testing at a significance level of 0.05) a sample size of 50 participants was needed to show a difference in KOOS between smokers and non-smokers groups. All statistical analyses were performed using Statistica 10 PL (Statsoft, Poland). The level of significance was set at p = 0.05 throughout.
Results
In total, 92 patients who met the inclusion criteria for this study completed follow-up questionnaires (Figure 1). There were 56 females (61%) and 36 males (39%) in the study group. The mean age for the entire cohort was 31.5 ± 8.81 years (range: 19–45 years old). There were a total of 77 medial meniscus repairs (84%) and 15 lateral meniscus repairs (16%). The mean duration of symptoms prior to surgery was 4.8 ± 3.6 months (range: 1–14.5 months), and mean postoperative follow-up time was 37.4 ± 10 months (range: 24–56 months). Additional demographic data stratified into non-smokers and smokers are summarized in Table 1.

Flow chart of the study.
Table documenting preoperative demographic criteria for the both study groups.
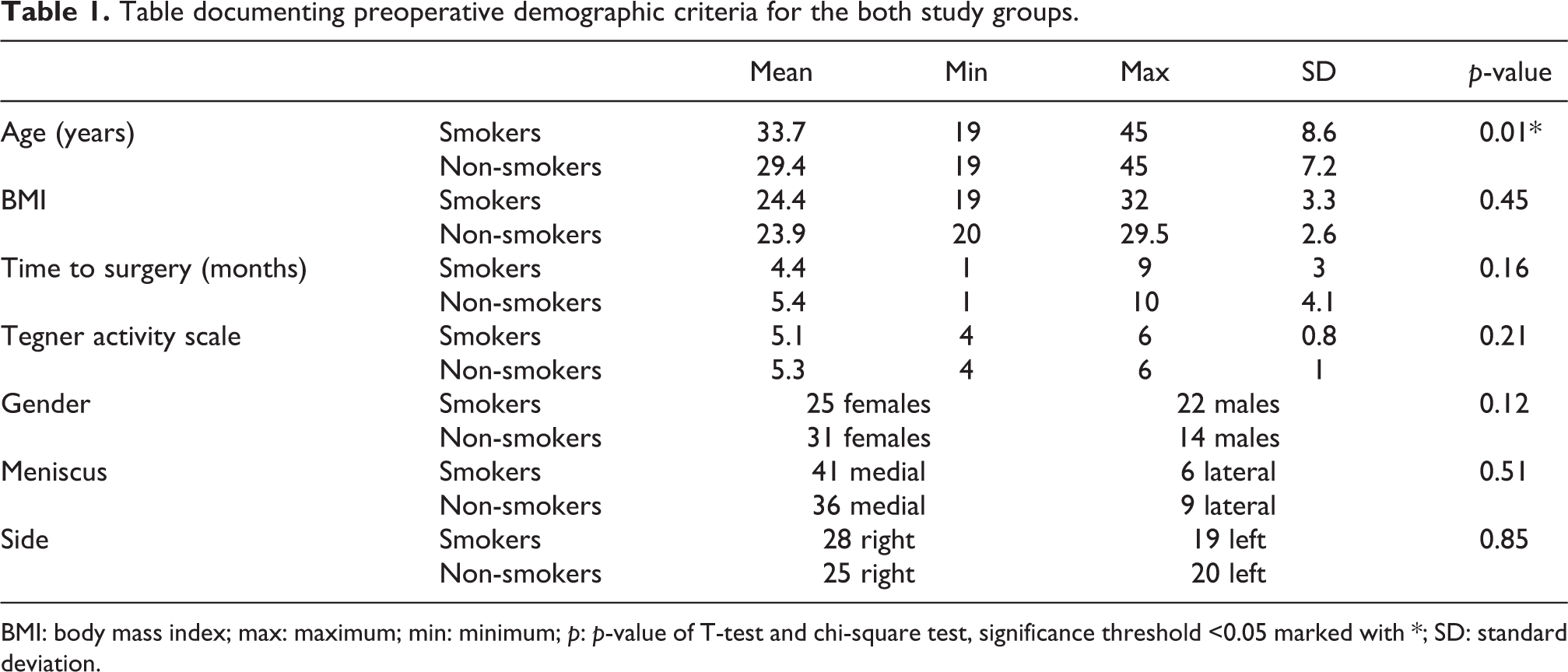
BMI: body mass index; max: maximum; min: minimum; p: p-value of T-test and chi-square test, significance threshold <0.05 marked with *; SD: standard deviation.
Postoperative clinical outcome scores were assessed for the 92 patients at a minimum of 2 years after their index procedure. None of the smoking patients changed their smoking habits during the period studied. The mean total KOOS was 73 ± 15 for the entire population, with significantly higher mean scores for the non-smokers’ group (80.2 ± 13.6) as compared to the smokers’ group (67.4 ± 14.7) (p = 0.001) (Table 2). Similarly, the statistical significance between study groups was observed in all KOOS subscales (Figure 2).
Outcome score tabulation for the patients in the smokers and non-smokers groups. Significance threshold was set at 5% (p < 0.05).

ADL: activities of daily living; KOOS: Knee Injury and Osteoarthritis Outcome Score; max: maximum; min: minimum; p: p-value of T-test and chi-square test, significance threshold <0.05 marked with *; SD: standard deviation; Sport activity: difference in preoperative and postoperative Tegner activity scale.

Comparison of KOOS subscales results between groups. ADL: activities of daily living; KOOS: Knee Injury and Osteoarthritis Outcome Score; QOL: quality of living; Sport/Rec: sport and recreational activities.
The non-smokers group returned significantly more than 1 month earlier to activities of daily living (ADL) and almost 2 months earlier to sport activities (RTS) (Table 2). There were no significant differences between the mean preoperative (5.4 ± 1.5) and postoperative (4.86 ± 0.97) Tegner activity scale for the entire population, as well as between the two subpopulations (Table 2).
There were five primary failures (return of mechanical symptoms less than 12 months after surgery) of meniscal repair in smokers group and three primary failures in non-smokers group. No other complications were reported during the study.
Discussion
Results of our study strongly indicate an association of smoking with worse post-surgical knee function and prolonged time of the return to daily and sport activities. KOOS results showed the significant differences in symptoms, quality of life and sport and recreation subscales in comparison with non-smoking participants.
Candidates who meet inclusion criteria were relatively young between 18 and 45 years of age at the time of surgery so we were able achieve high level of certainty their tissues will regenerate quickly as well that there were no underlying degenerative issues connected with age. Their BMI had to be below 35 to exclude the probability of risk factors connected with obesity. 18 All unstable knees were excluded since instability is widely acknowledged risk factor affecting the knee function and leading to degenerative diseases of the knee join. The rigorous inclusion criteria (87 patients out of 384 screened) allowed highlighting smoking as an most important risk factor in deterioration of the knee function, postoperative activities and overall life quality.
Previous studies describing smoking as a risk factor during meniscal repair surgery focused mainly on failure rates of this repairs. 11 –16
Blackwell et al. 11 assessed 104 patients (52 smokers and 52 non-smokers) and indicated that the risk of meniscus repair failure, as defined by the patient undergoing repeat surgery on the same meniscus, was 3.8 times higher for smokers compared to non-smokers. The risk of failure was significantly higher in smokers and reached 27% of failures in surgery on index knee in comparison with only 7% failure in none smokers when the candidates similarly like in our study were matched by sex age ACL status, BMI, meniscus repair technique and meniscus involved.
Haklar et al. 13 assessed the results of 140 patients with medial meniscal tears repaired with single or double vertical sutures and indicated smoking as a factor which had a significant, negative effect on meniscal healing (positive McMurray test) after repair using the inside-out technique. Uzun et al. also proved the deteriorating effect of smoking on meniscal healing after arthroscopic repair on both medial 15 and lateral 16 menisci regardless the type of the lesion and technique used for repairs. In both studies failure rates and the need for the revision surgeries were statistically higher for smokers than non-smokers: 37.5% vs 5.3% (p = 0.008) for medial meniscus 15 and 25% vs 6.5% (p < 0.05) for lateral meniscus. 16
The formation of the scar during meniscal healing depends on the vascularity 2 as well as quality of the meniscal tissue. 23 It is well documented that tissue vascularity and blood flow are impaired in smoking population. 1,4,7,8,24
In the study conducted by Lincoln et al. 25 on 1346 healthy Army recruits meniscus injury rate was significantly higher in smoking recruits during preliminary army training. Researchers concentrated on the incidence of meniscus injury in smokers versus no smoking soldiers, clearly showing the difference between groups as the prevalence of meniscal injury was much higher in the smoking group. 25 These findings showed that smoking had a high impact on meniscus as an anatomical structure, and explained our findings of lower KOOS scores and prolonged time of return to sport activities among smokers.
On the other hand in the retrospective study of 87 all-inside meniscal repairs Laurendon et al. did not show in univariate analysis the effect of Tobacco use on repair failure defined by secondary meniscectomy. 12 Also Moses et al. 14 in the retrospective cohort of 51 patients who underwent bucket-handle meniscus repair using all-inside and inside-out methods reported no association between smoking and repair failure rate, defined as a return of mechanical symptoms and pain alongside a re-tear of the repaired meniscus within 2 years of surgery in the same zone, as confirmed by MRI and arthroscopy.
This study has some limitations. It’s retrospective design did not allow to assess the type of zone of meniscal tear according to meniscal vascularity: red-red zone, white-white zone and red-white zone. 26 It is well known that meniscal healing and success of repair depend on the region of tear, 23 but the decision-making algorithm and surgical procedure were the same in both groups studied. From this study design it was impossible to find out which factor was more important: preoperative smoking alone or smoking during pre and postoperative period?
Conclusion
There is a significant difference in the speed of healing process, post-surgical quality of life as well as postoperative time frame of come back to sport between smoking patients and its nonsmoking peers. Furthermore, meniscus and its postoperational healing manifests very strong connection with smoking in comparison with other anatomical structures but it seems that the causation of it needs to be investigated further. Our findings indicate that in all of the assessed areas Tobacco users scored lower than non-smokers, particularly when it comes to come back to sport and Quality of life parameters.
Footnotes
Author contributions
M.D.: idea and design of the study, data analysis, manuscript preparation. M.M.: data collection, data analysis, manuscript preparation. J.W.: data collection, manuscript preparation. K.M.: data collection. A.G.: data analysis, manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical Board Medical University of Lodz.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All involved subjects gave informed consent to the work.