
Abstract
Purpose:
This study aims to measure the distance between the common site of Achilles tendon rupture and calcaneal insertion through ultrasound and to compare the outcomes between proximal and distal rupture groups.
Methods:
We investigated the electronic medical records of 117 patients and preoperative ultrasound describing the rupture site. Among 88 patients, we compared the patient-reported outcome and re-rupture rate of proximal and distal rupture groups.
Results:
The mean rupture site of the 117 included subjects was 4.5 ± 1.3 cm. The rupture site had a weak negative correlation with body mass index (ρ = −0.230, P = 0.013). Furthermore, 77% of the patients with distal rupture reported good outcome (Achilles Tendon Rupture Score > 80) compared to 56% of the patients with proximal rupture (P = 0.041).
Conclusion:
Patients with proximal rupture had less satisfactory postoperative outcomes than those with distal rupture.
Introduction
Achilles tendon rupture is a common injury with an incidence of 2.1–29.3 per 100,000 person-years. 1 –3 The pathogenesis of Achilles tendon rupture is insufficiently studied. Locating common rupture sites is crucial to the precise understanding of pathogenesis and important for clinical practitioners checking tenderness or dimpling on a patient with a possible Achilles tendon rupture.
Backer et al. reported that the average distance of the Achilles tendon rupture is 5.86 ± 2.66 cm from the calcaneal insertion. 4 Park et al. observed that the average rupture site is 6.4 ± 1.5 cm proximal to the calcaneal insertion. 5 These results contradicted previous reports on common rupture sites at 2–6 cm proximal to the calcaneal insertion; as such, objective imaging modalities, such as MRI or ultrasound, should be used to measure rupture sites. A study concluded that ultrasound and MRI are not interchangeable in the assessment of Achilles tendons. 6 Ultrasound and clinical examination provide approximate results about the distance between rupture ends, but the distance measured through MRI is larger. 7 However, studies have yet to use ultrasound to measure the common rupture site of the Achilles tendon.
The common site of Achilles tendon rupture is associated with avascularity. 8 Pathological differences, such as avascularity, in different sections of the Achilles tendon may affect not only the possibility of rupture but also the healing process after an injury. However, studies have yet to determine whether the rupture site influences surgical repair outcomes.
We hypothesized that the surgical outcomes of proximal and distal rupture groups are different. We aimed to measure the distance between the common rupture site of the Achilles tendon and the calcaneal insertion through ultrasound and to compare the outcomes between the proximal and distal rupture groups.
Methods and materials
Patients
This study was approved by the Institutional Review Board of our institution. The electronic medical records of patients who were hospitalized for Achilles tendon rupture in a regional foot and ankle surgery center from 2013 to 2020 were retrospectively investigated. A total of 123 patients were included. The inclusion criteria were as follows: patients who had Achilles tendon rupture and treated with surgical repair, had preoperative ultrasound describing the site of rupture, and performed daily activities not limited before injury (Ankle Activity Score not lower than 2). Exclusion criteria were: patients with incomplete information, open injury or with combined injury of lower extremities, and histories of lower extremity deformity or lower extremity fracture. Of the 123 patients, 6 were excluded because of incomplete information, or open injury. Finally, 117 patients were included for further analysis, and their medical records and ultrasound reports were carefully reviewed. The information about rupture site, gender, age, injured side, previous rupture history, height, weight, body mass index (BMI), Ankle Activity Score, 9 injury occurring on a weekend, routine warm-up before sports, smoking, alcohol usage, and glucocorticoid usage were extracted from medical records. Eighty-eight patients with a follow-up of more than 1 year after surgical repair were included for further outcome analysis (Figure 1).
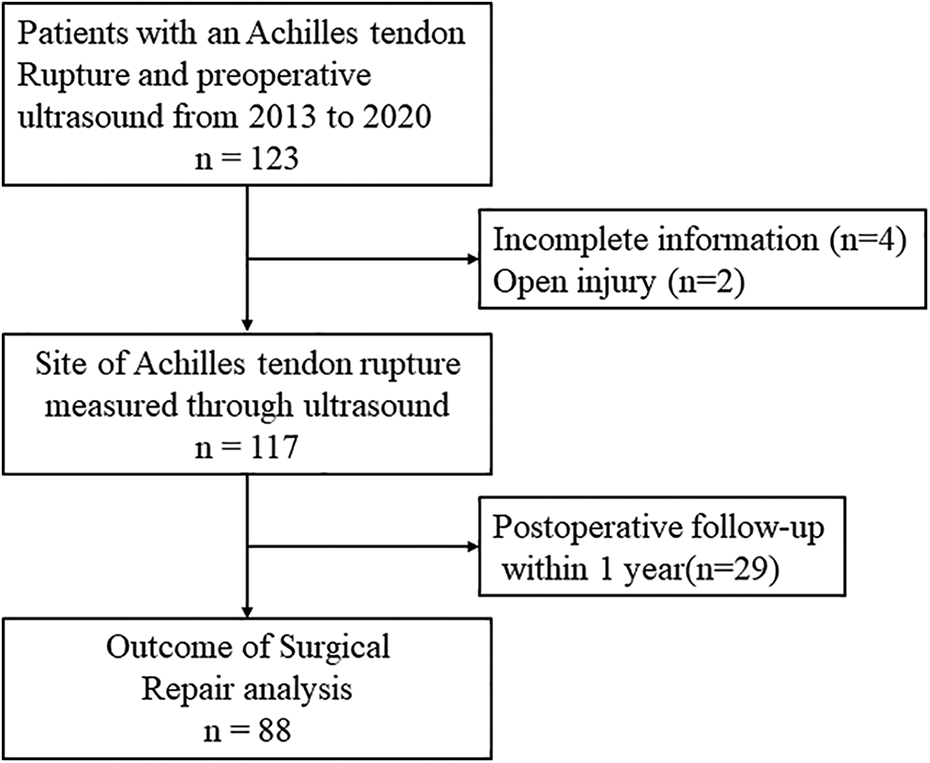
Flowchart of subject selection.
Ultrasound analysis
Ultrasound was performed in the same medical center within 2 days after a patient was hospitalized. All ultrasound examinations were performed by a senior radiologist. An ALT HDI 5000 US unit (Philips Medical Systems, Bothell, WA, USA) with high frequency (10–17 MHz) linear array transducers was used. The patients were instructed to lay prone on the examination table with their ankles at an approximate neutral position. The transducers were moved from the calcaneal insertion to the proximal part of the Achilles tendon over the skin with coupling gel. The straight distance from the most proximal point of the calcaneal insertion to the proximal end of the distal stump was measured (Figure 2). The rupture site that was longer than the length of a transducer was measured in separate frames and subsequently summed up.

Straight distance from the most proximal point of calcaneal insertion to the proximal end of the distal stump (dashed line). C, calcaneus.
Surgical repair and postoperative rehabilitation
All the 117 patients were surgically repaired. Under general anesthesia or spinal anesthesia, they were positioned to lay prone on a surgical table with a tourniquet around the root of the thigh. An incision was made over the posteromedial skin of the Achilles tendon. Repair was performed using the Krackow suture method. The paratenon was closed with 2-0 absorbable threads, and the skin was closed with interrupted sutures. The lower extremity was immobilized for 3 weeks. Then patients were allowed to begin partial weight-bearing in a walking cast 3–6 weeks postoperatively. They were subsequently instructed to have full weightbearing 6 weeks postoperatively in orthosis. They were allowed to walk without a supportive device 12 weeks postoperatively. Gentle jogging and single limb heel rises were also commenced. The postoperative rehabilitative regimen was supervised by the same senior physiotherapist.
Outcome measures
Eighty-eight patients with a follow-up of more than 1 year (average follow-up, 4.4 ± 2.4 years) after surgical repair were retrospectively surveyed using an Achilles Tendon Rupture Score questionnaire. This questionnaire included 10 questions, and a maximum of 100 points indicated the best possible outcome. A score of over 80 points was considered a good overall patient-reported outcome. Re-rupture events were also recorded at the time of the survey. The patients were categorized into a proximal rupture group if the distance between the rupture site and the calcaneal insertion was ≥4.5 cm and a distal rupture group if the distance was <4.5 cm.
Statistical analysis
The mean value, standard deviation, 10th percentile, and 90th percentile calculated in SPSS (version 19.0, SPSS Inc., USA) were used to describe the common rupture site of 117 subjects. Graphics were created using GraphPad Prism 6 software (GraphPad Software, USA). Correlations between the rupture site and continuous demographic data of the subjects were assessed with Pearson ρ. The rupture sites of the dichotomic groups of the subjects were compared via an independent t test. The outcomes of the proximal and distal rupture groups were compared using Chi-square test or Fisher’s exact test if one or more of the cell counts in a 2 × 2 table was <5. Odds ratios and 95% confidential intervals were applied to calculate the risk of less satisfied postoperative outcomes. P < 0.05 was regarded statistically significant.
Results
The 117 subjects had a mean age of 37.8 years (range, 16–66), a mean height of 173.7 cm (range, 156–191 cm), a mean weight of 75.7 kg (range, 49–105 kg), and a mean Ankle Activity Score of 6.0 (range, 2–9). Of these subjects, 91.4% (107 of 117) were injured during sports, and the most common sports were basketball (40 subjects), badminton (30 subjects), and soccer (27 subjects).
The distribution of the rupture site is illustrated in Figure 3. The rupture site had a mean value ± standard deviation of 4.5 ± 1.3 cm (range, 1.4–9.0 cm), with 10th to 90th percentile of 3.0–6.3 cm. The correlations between the rupture site and demographic data of the subjects are listed in Table 1. The rupture site was not significantly correlated with age, height, weight, and Ankle Activity Score, but it had a weak negative correlation with BMI (ρ = −0.230, P = 0.013, Figure 4). With the numbers available, no significant difference could be detected in the rupture site between different genders, sides, previous rupture histories, injury occurring on a weekend, routine warm-up before sports, smoking, alcohol drinking, or glucocorticoid usage.
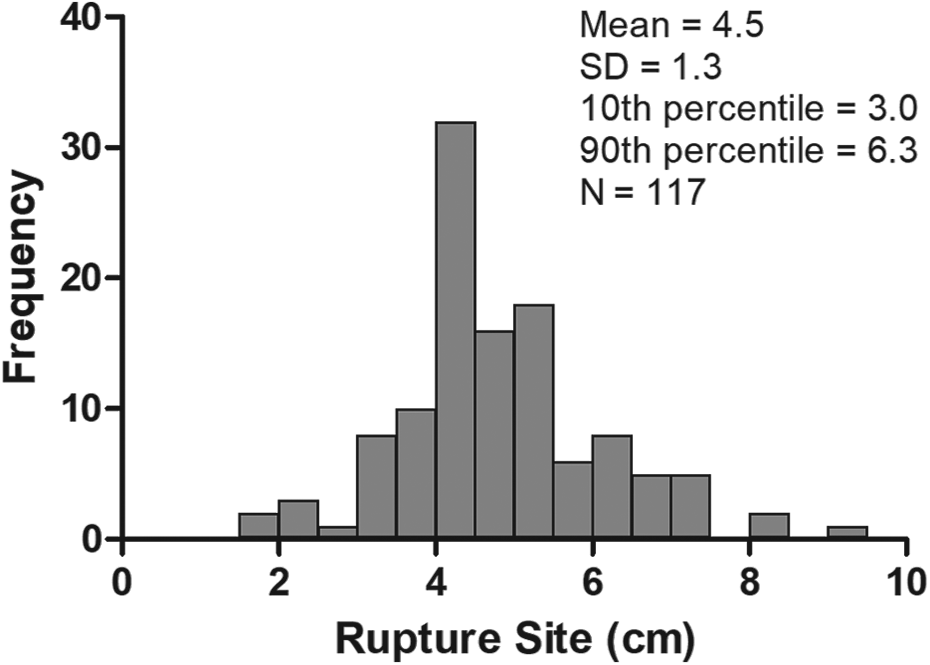
Distribution of rupture sites.

Negative correlation of the rupture site with BMI (ρ = −0.230, P = 0.013).
Patient demographics and their correlations with rupture site.

Data were listed as mean value (range) or number of patients. N/A, not applicable; *P < 0.05
The outcomes of the proximal and distal rupture groups are listed in Table 2. A good outcome was reported by 77% of patients with distal rupture (Achilles Tendon Rupture Score > 80). By comparison, a good outcome was observed in 56% of the patients with proximal rupture (P = 0.041). The patients with proximal rupture were more likely to have less satisfactory postoperative outcomes than those with distal rupture (odds ratio, 2.56; 95% confidential interval, 1.03–6.39). The re-rupture rate was not significantly different between these two groups. One postoperative wound infection was observed in the distal rupture group, but none was observed in the proximal rupture group.
Outcomes of proximal and distal rupture groups.

Data were listed as number of patients (percentage). *P < 0.05.
Discussion
In this study, the common site of Achilles tendon rupture measured through ultrasound was 3.0–6.3 cm from the most proximal point of the calcaneal insertion to the proximal end of the distal stump; this finding was comparable with commonly reported rupture sites at 2–6 cm proximal to the calcaneal insertion. 10 Conversely, the measured site was shorter than that obtained by Park et al. 5 In our study, the patients with proximal Achilles tendon rupture had less satisfactory outcomes after surgical repair than those with distal Achilles tendon rupture.
Previous reports on avascular area were similar to the average rupture site of 3.0–6.3 cm in the current study. The blood supply of the Achilles tendon is mainly from the posterior tibial, anterior tibial and peroneal arteries. 8,11 The blood supply of the mid-section (4–7 cm above the calcaneal insertion) of the Achilles tendon is mainly from the peroneal artery, which is relatively avascular and thin. 8 Carr and Norris reported that the part of the Achilles tendon 4 cm above the calcaneal insertion has the least blood supply and cross-sectional area. 10 Recent studies have found reduced capillary oxygen saturation and microperfusion at 5 cm above the calcaneal tubercles compared with those at 1 cm above the calcaneal tubercles. 12 These reports on the avascular region have indicated that the proximal Achilles tendon rupture has insufficient blood supply and serves as a risk factor affecting the surgical repair outcomes. However, the relation between proximal Achilles tendon rupture and unsatisfactory postoperative outcome has not been reported. 13 –15 Patients with proximal Achilles tendon rupture might benefit from an extended period of postoperative rehabilitation because of an insufficient blood supply.
Biomechanical features are not consistent among different sections of the Achilles tendon and may contribute to results of the common rupture site. 16 Different biomechanical strengths may be related to various arrangement patterns of type I and type III collagens. Ruptured Achilles tendons have more type III collagens than healthy Achilles tendons, and this pathological feature is evident in regions adjacent to the rupture site. 17,18
In the current study, the Achilles tendon rupture site had a weak negative correlation with BMI in the current study. In general, subjects with a high BMI may have a high cholesterol level, 19 which is an important metabolic factor that likely affects the collagen arrangement pattern 20 and the biomechanical feature of the Achilles tendon. 21 However, studies have yet to determine whether the biomechanical change due to the metabolic factor in the Achilles tendon is region specific.
The findings of the present study differed from those of a previous report possibly because different points in the insertion footprint are defined as the distal end of the Achilles tendon. 5 The most proximal point of the calcaneal insertion was used as the distal end of the measured Achilles tendon instead of the most distal fibers of the Achilles tendon at the calcaneal insertion. This difference may result in approximately 17.8 mm discrepancy in length. 22 The most proximal point of the calcaneal insertion was chose for the following reasons. First, the results acquired through this method were more similar to clinical situations where the rupture site is measured from the palpable posterosuperior margin of the calcaneal tuberosity. 5 Second, the most distal fibers of the Achilles tendon at the calcaneal insertion may be continuous with the plantar fascia via the periosteum; consequently, locating the accurate point of the most distal fibers becomes difficult. 22 Third, insertional ruptures rarely occur between the most proximal point of the calcaneal insertion and the most distal fibers. 23 The rupture sites of the mid-substance ruptures are better reported as the distance from the most proximal point of the calcaneal insertion. Fourth, the most proximal points of the calcaneal insertion are widely used as an anatomic landmark in studies on Achilles tendons. 11
Ultrasound may systemically differ from MRI in terms of assessing the Achilles tendons. Ernat et al. reported that the distance between two rupture ends of the Achilles tendons measured through clinical examination and ultrasound has an average difference of 1.1 ± 1.4 cm from those measured through MRI. 7 Kruse et al. reported that the cross-sectional areas of the Achilles tendons measured through ultrasound are 5.5% smaller than those measured through MRI. 6 They suggested that this discrepancy is related to the pressure applied to the transducers during ultrasound measurement. Although ultrasound has the advantage of low cost, comparability with physical palpation, and dynamic assessment, this imaging modality has the deficiency of relatively low reliability and high dependence on the experience of operators.
This study should be cautiously interpreted because of several limitations. First, surgical treatment outcomes depended on several other factors because of the retrospective nature of this study. However, we tried to eliminate the confounding factors. The surgical technique and postoperative rehabilitation protocol were identical for all the included subjects. All ultrasound examinations were performed by the same senior radiologist. Second, the Achilles Tendon Rupture Score and postoperative re-rupture rate were evaluated in a small group of subjects only. As such, further studies with larger numbers of included subjects and objective outcome measurements, such as plantarflexion strength and heel rise height, should be performed.
Conclusions
The common site of the Achilles tendon rupture measured through ultrasound was 3.0–6.3 cm. The Achilles tendon rupture site had a weak negative correlation with BMI. Patients with distal Achilles tendon rupture reported better surgical outcomes than those with proximal rupture. Clinical practitioners should be aware that patients with proximal Achilles tendon rupture had less satisfactory outcomes after surgical repair. These findings are important for clinical practice and beneficial to the precise understanding of pathogenesis in the treatment of patients with Achilles tendon rupture.
Supplemental material
Supplemental Material, sj-xlsx-1-osj-10.1177_23094990211007616 - Influence of Achilles tendon rupture site on surgical repair outcomes
Supplemental Material, sj-xlsx-1-osj-10.1177_23094990211007616 for Influence of Achilles tendon rupture site on surgical repair outcomes by Shengxuan Cao, Zhaolin Teng, Chen Wang, Qian Zhou, Xu Wang and Xin Ma in Journal of Orthopaedic Surgery
Footnotes
Authors’ note
Shengxuan Cao, Zhaolin Teng, and Chen Wang contributed equally to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Xin Ma is currently receiving grants from National Natural Science Foundation of China (Grant No. 81772295).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.