
Abstract
Objective:
Cervical tubercular disease (CTB) is a rare pathology and constitutes 3–5% of all spinal TB. It includes atlantoaxial TB and sub-axial TB. As the literature evidence on this subject is scarce, majority of issues concerning CTB are still controversial. The current narrative review comprehensively discusses the various aspects related to CTB.
Results:
The initial search using keywords cervical tuberculosis, atlantoaxial tuberculosis, sub-axial tuberculosis, and cervico-thoracic tuberculosis yielded 4128, 76, 3 and 9 articles on ‘pubmed’ database, respectively. A similar search using the aforementioned keywords yielded 1,96,000, 2130, 117 and 728 articles on ‘google scholar’ database. The initial screening resulted in the identification of 178 articles. Full manuscripts were obtained for these articles and thoroughly scrutinised at the second stage. Review articles, randomised controlled trials and level 1 studies were given preference. Overall, 41 articles were included.
Conclusion:
AATB and SACTB constitute 0.3 to 1% and 3% of spinal TB, respectively. The incidence of neuro-deficit in CTB is significantly more than other spinal TB. The general principles of management of CTB are similar to spinal TB elsewhere and medical therapy remains the cornerstone. Surgery is advocated in specific scenarios involving gross neuro-deficit, later stages of disease with significant bony/ligamentous disruptions, altered sagittal balance, drug resistance, and poor response to medications. The surgical approaches for AATB include anterior-alone, posterior-alone and combined approaches, although posterior access is the most preferred. Most of the studies on SACTB have supported the role of anterior approach. Additionally, posterior stabilisation may be necessary in specific scenarios. The overall long-term outcome in CTB is favourable.
Keywords
Introduction
Tuberculosis is a serious infectious disease, which has inflicted major social problems in middle- and low-income nations over centuries. 1 –8 However, following the recent global migration phenomenon, increase in elderly population and emergence of immunosuppressive conditions, developed nations have also seen a resurgence. 9 –11 Additionally, a steady rise in the prevalence of drug-resistant organisms has been another major concern in the developing nations. 12,13
While spinal TB accounts for around 1% of total TB burden, cervical TB accounts for 3–5% of all spinal disease. 1,14 –16 The smaller canal dimension, proximity to vertebral artery and other vital structures, unique facetal architecture, higher mobility and lordotic alignment make cervical spine vulnerable to greater neuro-deterioration, instability and progressive mal-alignment. 1,15 –19 In view of the paucity of literature on this pathology, controversies still exist regarding its presentation, ideal modalities for diagnosis and treatment options. The current narrative review comprehensively discusses the verdict of current literature on various aspects of diagnosis and treatment of patients with cervical TB (CTB) disease; and aims to highlight the intricacies and dilemma involved in its management.
Literature search
An elaborate search was made using keywords cervical tuberculosis, atlantoaxial tuberculosis, sub-axial tuberculosis, and cervico-thoracic tuberculosis, on pubmed and google (scholar.google.com) databases on the second of December, 2020. We identified crucial questions regarding cervical tuberculosis and included relevant articles pertaining to these topics.
Results
The initial search using the keywords cervical tuberculosis, atlantoaxial tuberculosis, sub-axial tuberculosis, and cervico-thoracic tuberculosis yielded a total of 4128, 76, 3 and 9 articles on ‘pubmed’ database, respectively. A similar search using the aforementioned keywords yielded a total of 1,96,000, 2130, 117 and 728 articles on ‘google scholar’ database. The initial screening involved exclusion of duplicate articles, articles unrelated to CTB, animal or other non-clinical studies, and articles in non-English literature based on abstracts or titles of articles. This initial screening resulted in the identification of 178 articles. Full manuscripts were obtained for these selected articles and thoroughly scrutinised at the second stage. All articles not concerning CTB, not pertaining to concerned questions, articles concerning other cervical pathologies, case reports or animal studies, articles in non-English language and duplicate articles were excluded. Review articles, randomised controlled trials and level 1 studies were given preference (Figure 1). Finally, 41 articles were included in this review. We did not perform any screening [Methodological Index for non-randomised studies (MINORS) or Preferred Reporting Items for Systematic Reviews and MetaAnalyses (PRISMA) criteria] for including articles.

(a) and (b) Sagittal and axial sections of T2WI-MRI showing features of active TB infection with significant destruction of C7 vertebral body, large epidural and paraspinal abscesses; (c) and (d) Sagittal and axial sections of post-operative T2WI-MRI showing features of complete resolution of infection after C7 corpectomy and C6–T1 fusion with healing of epidural and paraspinal abscesses.
Discussion
The literature broadly classifies CTB into cranio-vertebral (CVJ) and sub-axial cervical disease (SACTB). 1,2,14,17,20,21 Additionally, lesions involving cervico-thoracic (CT) junctional levels need special consideration, owing to the biomechanical peculiarities of this transitional zone. 16 The pathophysiology, clinical presentation, diagnostic modalities and general principles of treatment of CTB are in similar lines with spinal TB elsewhere and have been discussed vide-infra. Specific characteristic of individual cervical region (CVJ, SAC, CT) and their management guidelines have been separately discussed.
Epidemiology
The term ‘upper cervical TB’ encompasses cases which involve C1 and C2 vertebrae [atlantoaxial disease (AA)] and constitute 0.3 to 1% of all spinal TB. 2,3,15,20,22 Sub-axial cervical TB (SACTB) is also a rare phenomenon and constitutes <3% of spinal TB. 1,14,16,18,19 Although mortality rates following CTB have reduced from 10% to 3% with effective antibiotic regimen, high rates of deformity and paraparesis (around 15–30%) have continued to remain issues of major concern. 1,23,24
Pathophysiology
TB is caused by Mycobacterium tuberculosis complex, which include fastidious, aerobic bacilli. 6,8,25,26 A vast majority of these spinal TB (including most CTB) lesions are secondary infections due to hematogenous (arterial/venous plexuses) or lymphatic spread from primary sites like pulmonary, mesenteric, genito-urinary, gastrointestinal or lymph nodal disease. 8,9,27 –30 A protracted course of retropharyngeal abscess can also tract to cervical spine, leading to localised disease. 1,14,18,19
The disease is characterised by granulomatous inflammation constituted by lymphocytic infiltration and epithelioid cells, which merge to form Langhans giant cells and finally end up in caseous necrosis of involved tissues forming cold abscesses. 28,31 –33 Similarly, progressive osseous destruction by disease leads to instability and deformity. 34,35 While in adults, lesions are localised and less purulent; children tend to manifest with diffuse and extensive disease. 1,6,28,36
Clinical presentation
The four most common clinical presentations of spinal TB include pain (axial/radicular), constitutional symptoms, neuro-deficit and deformity. 6,8 Axial neck pain (87%), radicular pain and limited neck mobility (94%) are the most common presenting symptoms of SACTB. 1,4,14 Alternately, these patients may present with systemic complaints [fever(18%), night sweats(24%), cervical lymphadenopathy(17%), anorexia and emaciation] or pressure-related morbidities due to retropharyngeal abscess [dysphagia(5%), inspiratory stridor(7.5%) and airway compromise]. 4,14,19
In later stages of AATB, severe restriction of neck movements and torticollis are characteristic presentations. 22 Clinically, AATB has rarely been reported to manifest as occipital condyle syndrome (characterised by mastoid pain, apprehension sign, torticollis and ipsilateral 12th cranial nerve palsy) or post-infectious atlantoaxial rotary instability (Grisel’s syndrome). 22,37 –39
70% of patients with spinal TB may present with cold abscesses. 8,29,31 These are chronic abscesses and are devoid of signs of inflammation. These abscesses track sub-ligamentously or along natural planes; and present in a variety of locations. Paravertebral abscesses in cervical region present in the retropharyngeal or sub-mandibular spaces, or track along brachial plexus and present in the axilla or medial side of arm. 40,41
The prevalence of neurological compromise in CTB is reported to be as high as 74% and is higher than TB involving rest of the spine. 4 The possible causes for neuro-deficit during active disease include a. mechanical compression from epidural abscess, granulation tissues, pathological fractures, retropulsed fragments, or spinal instability, b. primary cord involvement/oedema, c. cord arteritis/thrombosis or ischemia. During the healed phases, various static (cord atrophy, myelomalacia, dural fibrosis, traction or compression injury to the cord at the apex of deformity) and dynamic (pseudoarthrosis and inter-vertebral instability) factors contribute to neuro-deterioration. 34,42 –44 The incidence of cord compression and neuro-deficit is significantly high in adults (even reported as high as 81%), owing to associated factors like pre-existing degenerative spinal narrowing, increased spinal rigidity and reduced elasticity of pre-vertebral fascia. 1
In general, these lesions involve anterior vertebral bodies with sparing of posterior elements. 45 –47 Since the line of weight transmission in cervical spine is posterior to vertebral body, kyphosis (19%) in CTB tends to be less of a concern as compared with thoracic or thoraco-lumbar TB.
Diagnostic approach in spinal TB
The approach to diagnosing spinal TB is three-pronged and includes laboratory work-up, imaging and tissue diagnosis. 6 –8,31,34 In endemic regions, a high degree of suspicion based on typical clinico-radiological findings helps in clinching the diagnosis.
Blood investigations
While elevated total leukocyte counts (TLC) are reported in 30–50% of patients, elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are seen in two-thirds of patients with spinal TB. 8,31,34 The latter two parameters have significant prognostic utility, as persistently elevated ESR and CRP beyond 3 months of chemotherapy should trigger suspicion of alternate diagnosis, poor drug compliance, insufficient dosage or drug resistance. Liver function (LFT) should also be assessed in all patients, as most anti-tubercular drugs (ATT) are hepato-toxic. 48 –50
Immunological tests
Immunological tests like Mantoux, interferon release assay and immunoglobulin-based tests evaluate host immune response to tubercular antigens. 51 –53 Interferon gamma (IFN-γ) release assays are enzyme-linked immunosorbent assay (ELISA) tests, which identify the amount of IFN-γ released against TB antigens (QuantiFERON TB and QuantiFERON TB Gold; sensitivity-85%, specificity-95%). The utility of these immunological tests is limited in endemic regions with high prevalence of TB, as they may be positive even in the absence of active disease.
Imaging
Spinal TB is predominantly an ‘anterior vertebral disease’ and has been described to present in four different patterns, namely para-discal [most common – involvement of vertebral endplate and marrow adjacent to inter-vertebral disc (IVD)], central, posterior, and non-osseous disease. 6,8,28,31 In cervical disease, the most common patterns of presentation include para-discal and central.
Plain radiographs do not demonstrate any significant findings in the initial 3–4 weeks. Disc space narrowing, lytic lesions, enhanced vertebral radiolucency and kyphotic collapse are characteristic features. Additionally, retropharyngeal abscess (observed as widened pre-vertebral space), anterior vertebral scalloping (aneurysmal phenomenon) and calcifications within soft tissue shadows can also be evident. 8,29,31,36,54 –56
Computed Tomography (CT) can demonstrate bony lesions more lucidly than plain radiographs. Lesions smaller than 1.5 cm, soft tissue calcifications and CVJ lesions are best depicted on CT. 41,55,57 –59
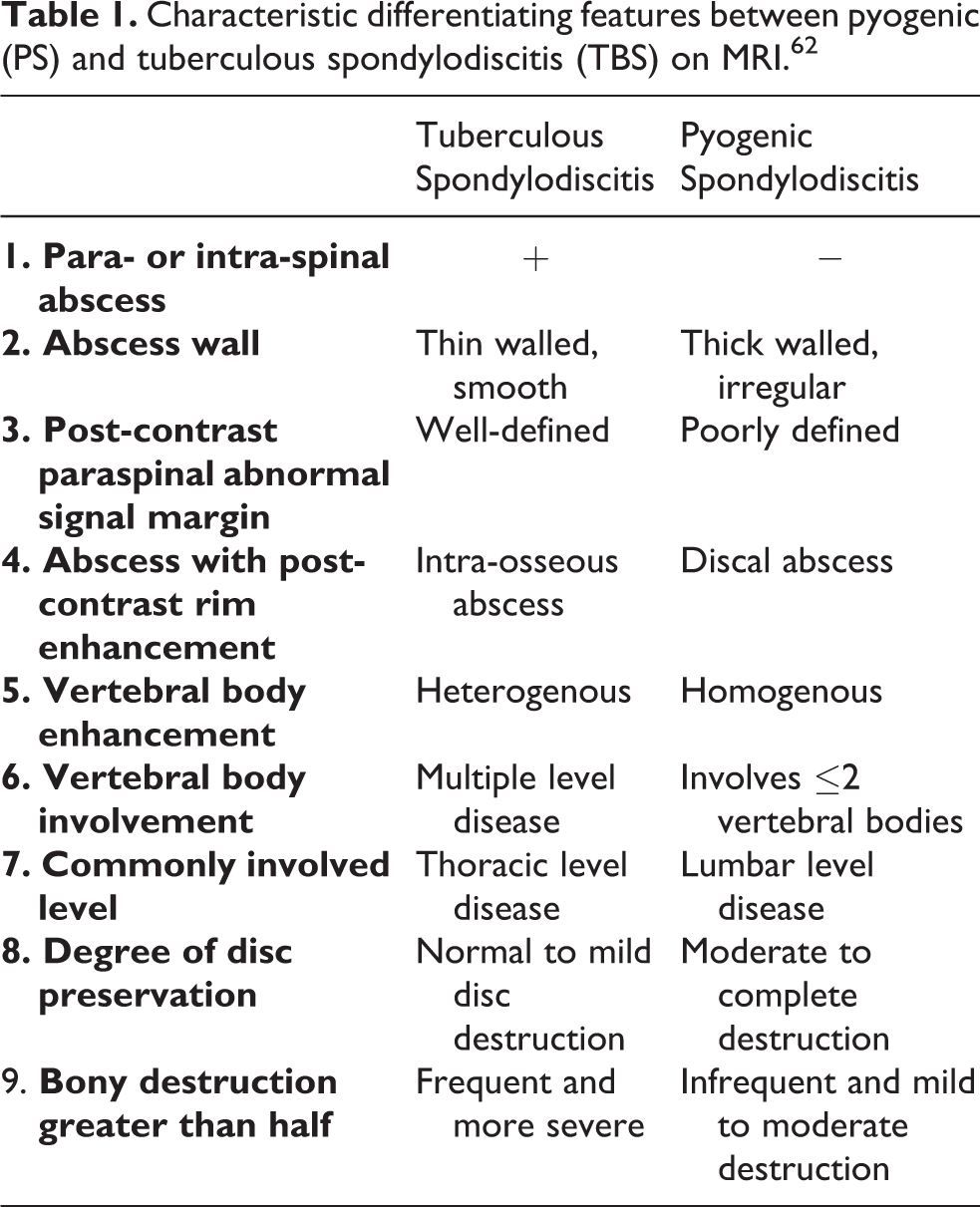
The gold standard for diagnosing spinal TB is magnetic resonance imaging (MRI), with a reported sensitivity and specificity of 93% and 96%, respectively. MRI [T1WI, T2WI, short tau inversion and recovery (STIR) and contrast-enhanced sequences] has a major role in differentiating tubercular lesions from pyogenic infections or neoplasia. 31,60,61 The characteristic MRI findings of TBS include thin and smooth-walled abscess with uniform contrast uptake, large paraspinal/intra-osseous abscess, relative preservation or late involvement of disc, multi-vertebral disease and sub-ligamentous extension of abscess 62,63 (Table 1). Metastatic lesions are characterised by vertebral destruction (with bulging posterior vertebral wall), soft tissue masses and disc sparing; typical TBS lesions present with vertebral body destruction, narrowed disc space and paraspinal abscess. 6,28,31 Dynamic contrast-enhanced MRI (DCE-MRI) demonstrates good accuracy in differentiating TB and metastasis, taking advantage of the differences in cellularity and vascular pattern. 64,65 Additionally, MRI can be helpful in determining cord status (oedema/myelomalacia/atrophy) and nature of cord compression in patients with neuro-deficits. 8,28,29,31 Non-contiguous or skip lesions are also best identified by whole spine screening sequences on MRI. 6,28,29,31
Nuclear scans FDG-PET aid in identifying hypermetabolic regions within the lesions which enables a targeted tissue sampling, as well as evaluate the metabolic activity of lesions and monitor response to treatment. 10,66,67
Characteristic differentiating features between pyogenic (PS) and tuberculous spondylodiscitis (TBS) on MRI. 62
Tissue sampling
The most important step in confirming the diagnosis is the analysis of tissue samples obtained from infected foci. Tissues may be procured either surgically or percutaneously under image (fluoroscopic/CT) guidance. All procured tissues must be sent for molecular [polymerase chain reaction (PCR)], pyogenic bacterial culture, tubercular culture and histopathological examinations.
28,31,34
Polymerase chain reaction (Xpert MTB/RIF) analysis is a molecular test which allows rapid (90 minutes) and accurate (88% sensitive, 98% specific) detection of TB DNA sequences. It also detects the genetic mutations associated with rifampicin resistance.
29,31,68,69
Bacterial culture All procured tissue samples are subjected to standard aerobic culture for pyogenic bacteria as well as sensitivity to routine antibiotics.
Tubercular culture The gold standard confirmatory test in diagnosing spinal TB is mycobacterial culture (Becton-Dickinson and Co., BACTEC and BACTEC MGIT). All culture-positive samples should also undergo testing for sensitivity to first- and second-line ATT.
29,31,70,71
Histopathological examination (HPE) has been demonstrated to show substantially higher yields as compared with culture techniques in different studies (sensitivity-8.2%, specificity-93.4%, accuracy-92%). The typical HPE findings in TB include granulomatous lesion (tubercles) with caseating necrosis, multinucleated giant cells, epithelioid cells and lymphocytes.
29,31,72
–74
Differential diagnosis
In non-endemic regions, diagnosis can be challenging and requires a high degree of suspicion. Pyogenic or fungal osteomyelitis, inflammatory conditions, and neoplastic conditions (myeloma and lymphoma) need to be considered. 34,75,76
Principles of medical management
In accordance with the age-old adage, ‘Uncomplicated tuberculosis is primarily a medical disease’, chemotherapy remains the cornerstone in the management of spinal TB. 28,77,78 The first-line ATT include isoniazid(INH), rifampicin(RMP), ethambutol(EMB), pyrazinamide(PYZ) and streptomycin(S). The general recommendations for medical therapy in TBS are administration of multiple-drug regimen over long duration. Based on recent WHO guidelines, typical regimen includes two phases: intensive phase of 2 months involving 4 drugs, and continuation phase of 7–9 months involving two or three drugs. In drug-resistant infections, appropriate changes are made to incorporate effective first- and second-line drugs. The main factor determining the success of conservative management is the sensitivity of organism to ATT. 53,79
All conservatively managed CTB patients must also be considered for appropriate external spinal immobilisation, so as to prevent long-term deformity. The options for external immobilisation include hard, Philadelphia, Minerva, Aspen, Miami and four-post collars; and halo-vest orthosis. 38,80 –82 Grady et al. 82 supported the use of Philadelphia collar for immobilisation and concluded that outcome following collar depended on three factors, namely compliance, age and neck mobility while wearing collar. The general recommendation is to ensure strict adherence to a rigid orthosis (Halo-vest, Minerva/four-post collar etc.) and avoidance of all activities involving neck movements and weight-bearing for ≥3 months or until there is definitive radiological evidence of healing. 22,80
Monitoring response to ATT
Patients on ATT are monitored regularly for their response to medications. The evaluation includes clinical assessment (subjective sense of well-being, improvement in symptomatology, increased appetite, weight gain and neurological recovery), laboratory evaluation (ESR, CRP, LFT), and radiological evidence of healing (bony sclerosis, resolution of lytic lesions and re-ossification on plain X-rays/CT). MRI is a very useful modality 29,31,83,84 to assess treatment response (Figure 1). The follow-up T1WI may be used to prognosticate the response to ATT. In a patient responsive to ATT, T1WI shows a progressive increase in signal intensity within vertebral marrow indicating gradual fatty marrow replacement. The corresponding T2WI shows complete resolution of granulation tissue and pus collection. Alternately, nuclear imaging (PET/CT) may also be utilised to assess response to therapy. 10,66,67
Indications for surgical intervention in CTB
The four main objectives of surgical indications in spinal TB include obtaining tissue samples, spinal decompression, debridement and stabilisation. 29,31,85 The usual indications for surgical intervention have been shown in Table 2.
As previously mentioned, CTB is considered as three separate entities based on region of involvement, namely AATB (CVJ TB), SACTB and CTTB. Specific considerations with regard to each region have been discussed below.
Indications for surgery in spinal TB. 28

AATB
Imaging principles
Plain radiographs of cervical spine [open-mouth antero-posterior (AP) and lateral views] are the initial investigations. Increased atlanto-dens interval (>3 mm in adults and >5 mm in children) can help in identifying AA instability 2,5,86,87 As in other cases of spinal TB, computed tomography (CT) and magnetic resonance imaging (MRI) can help precisely delineate bony, soft tissue, articular and spinal canal morphology. CT provides the best information regarding AA articular status and BI. 88
Classification systems
The classification systems described in AATB may be grouped into clinical- and radiological-based systems. The classic classification by Lifeso 3 includes three stages, namely stage 1 where ligamentous/bony architecture are well-preserved, stage 2 where ligamentous architecture is compromised; and stage 3 where significant osseous destruction is observed. Goel 22 classified AATB into three stages based on extent of disease. Stage 1 includes lesions with unilateral involvement of cancellous portions of atlas, axis and odontoid. Stage 2 is characterised by extension of disease onto unilateral AA joint. In stage 3, disease involves bilateral AA joints. Stage 3 lesions have high prevalence of associated neuro-deficit. Behari and Arora 2,5,89 classified AATB into four grades (Di-Lorenzo grading), based on clinical presentation: grade 1 includes patients with neck pain alone, grade 2 includes independent patients with minor disabilities, grade 3 and 4 include patients who are partially and totally dependent on others for activities of daily living. A similar classification system incorporating both clinical and radiological parameters has been put forth by Teegala. 90,91
Surgical indications
A majority of studies have shown that as with tubercular disease of the rest of skeletal system, management of AATB is essentially medical. 2,3,23 In general, literature is divided between two antithetical algorithms: a. algorithm relying on conservative measures 23,89,92 and b. algorithm including surgical options depending on clinical condition and radiological findings. 2,5,93 While the former approach advocates long-term rigid orthosis application, the latter approach advocates surgical fixation (±decompression).
However, the current recommendation is that patients with more extensive radiological destruction and those with significant neuro-deficit would benefit from surgery. 2,5,88 Goel 22 recommended conservative treatment for stage 1 and 2 disease; and surgery for stage 3. Similar algorithms have been put forth by Teegala et al., 90 Molliqaj et al. 88 and Behari et al. 2,5 for surgically managing patients with AATB.
Surgical approaches
The surgical approaches in AATB include anterior-alone, posterior-alone and combined approaches. 2,3,5,21,23,37,39,88,90 –93 In general, while anterior approach gives direct access to lesion and enables better decompression and tissue sampling; posterior approach provides biomechanically robust options for stabilisation.
Currently, posterior approach is the most preferred globally. 5,88 The options for stabilisation through posterior approach include AA fusion and occipito-cervical fusion (OCF) 22 (Figures 2 and 3). In patients with atlantoaxial disease alone, AA fusion may suffice. The importance of pre-operatively assessing reducibility of AA dislocation (AAD) in these patients cannot be understated. While patients with reducible AAD benefit from posterior fusion alone, those with irreducible or rotatory AAD require posterior distraction (and reduction) with stabilisation or combined antero-posterior approaches. Additionally, in patients with irreducible AAD, pre- or intra-operative halo traction may be considered for achieving reduction. 2,5,22,88 However, if the disease has already progressed to the occipito-atlantal joints leading to BI or those with significant bilateral AA joint destruction, OCF offers the best stability.

(a) and (b) Antero-posterior and lateral plain radiographs showing significant destruction and dislocation of C1–C2 vertebrae secondary to AATB; (c) and (d) Coronal and sagittal images showing significant C2 vertebral destruction; (e) Axial section of T2WI-MRI showing a large abscess and C2 vertebral destruction; (f) and (g) Right para-sagittal and mid-sagittal sections of T2WI-MRI showing large pre-vertebral and right paravertebral abscesses and C2 vertebral destruction; (h) and (i) Antero-posterior and lateral plain radiographs showing C1 to C4 instrumented stabilisation and complete healing.

(a) and (b) Antero-posterior and lateral plain radiographs showing significant destruction, dislocation of C1–C2 vertebrae and secondary to AATB with torticollis; (c) to (e) Parasagittal and mid-sagittal sections of T2WI-MRI showing AATB with significant pre-vertebral abscess; (f) Coronal MRI showing right parasagittal and perifacetal abscess; (g) and (h) Antero-posterior and lateral plain radiographs showing occipito-cervical fusion and good healing of AATB.
SACTB
Imaging principles
Among radiological investigations, plain standing radiographs yield the most useful information regarding cervical alignment [C2–C7 lordosis and C2–C7 sagittal vertical axis (SVA)]. 46,47 Additional whole spine radiographs can be helpful in determining compensatory changes in the rest of spine and pelvis in patients with major cervical deformities. In the series by Hsu and Leong, 14 two-segment involvement was the commonest pattern, followed by single- or multi-segment involvement. C5 was the most common level, followed by C6.
Classification systems
Wang et al. 15 described a clinico-radiological grading which includes three separate components, namely restriction of neck movements, motor power and radiological features (including paravertebral abscess, bone destruction and cord compression). A score of 3–4 was classified as grade 1, 5–6 as grade 2 and 7–8 as grade 3.
Surgical indications
The indications for surgical intervention in patients with SACTB are similar to the general recommendations for TB involving other regions of the spine. 4 Recently, the significance of cervical sagittal balance in deciding upon need for surgical stabilisation has been highlighted. It has been recommended that patients with C2–C7 lordosis >0° or C2–C7 SVA >4 cm have poorer neck disability index (NDI) as well higher chance of kyphosis progression; and would benefit from anterior cervical debridement and reconstruction. 46,47
Surgical approaches
Anterior approach to cervical spine gives the most direct access to diseased vertebrae, enables better disease clearance, spinal decompression, and offers robust stabilisation, ameliorated reconstruction, fusion, as well as better lordosis restoration. Most of the current studies on SACTB have supported the role of anterior approach. 1,17,18,49
In the classic series by Hsu and Leong, 14 all patients recovered after radical debridement followed by reconstruction (Hong Kong procedure) through Southwick-Robinson approach. Wu et al. 18 reported excellent outcome (significantly improved kyphosis angle) following anterior debridement, decompression and instrumented fusion with titanium mesh cage. Similar reports by He et al. 94 also demonstrated 100% fusion and neurological stabilisation in 25 patients who underwent anterior debridement and reconstruction with bone graft. Koptan et al. 95 performed a non-randomised trial comparing roles of titanium mesh cage and iliac crest bone graft; and concluded that cage-reconstruction enabled better restoration of kyphosis. Recent systematic reviews 96 have also demonstrated the superiority of anterior approaches for debridement in CTB.
Additionally, posterior approach (Figure 4) may be necessary in patients with pan-vertebral or posterior-only involvement, significant kyphosis/ sagittal imbalance, long-segment disease necessitating corpectomies >2 levels, junctional level (cervico-thoracic junction) and those with additional canal compromise due to compression from vertebral elements lying posterior to the cord (thickened ligamentum flavum, congenitally narrow canal etc.). 17,97 Based on their clinico-radiological grading, Wang et al. 15 proposed a treatment protocol for SACTB: conservative treatment for grade 1, anterior debridement and fusion for grade 2; and combined anterior-posterior approach for grade 3 lesions.

(a) and (b) Antero-posterior and lateral plain radiographs showing significant destruction and involvement of C3 to C6 vertebrae; (c) to (e) Mid-sagittal T2WI-MRI, Mid-sagittal CT and axial T2WI-MRI showing C3–6 tubercular infection with significant vertebral destruction and a large epidural abscess extending across these levels; (f) and (g) Antero-posterior and lateral plain radiographs showing C3–C6 antero-posterior instrumented fusion and good healing of SACTB.
Yin et al. 17 concluded that anterior and combined antero-posterior approaches were viable options in SACTB; and all patients, irrespective of the approach demonstrated good neurological recovery, pain improvement and restoration of alignment. The therapeutic strategies need to be individualised, depending upon patient’s general condition, disease characteristics and surgeon’s expertise.
CTTB
CT lesions (C7 to T2) 16 carry certain peculiarities, as compared with rest of SAC lesions. Being a junctional level, it represents a transitional zone between kyphotic and lordotic, as well as rigid and mobile spinal segments. 98 These factors predispose it to enhanced biomechanical stresses, which augment its propensity to develop progressive kyphosis and instability. Therefore, it is recommended that the surgeon understands inherent characteristics of this region and has a lower threshold to stabilise these lesions, as compared to elsewhere in SAC spine. 16
CT spine can be accessed through traditional anterior cervical or posterior approaches. 16,99 –101 The literature has been in favour of anterior approach (alone or in combination with posterior approach) as a safe and direct approach to the diseased vertebra. 98,100,102 –106 Anatomically, deep location of CT vertebrae with the presence of sternum, clavicles and mediastinum anteriorly as well as scapulae posteriorly, kyphotic collapse of the diseased vertebrae; and anatomical proximity to complex vital structures make the surgical access to this region challenging. 105
Extended versions of anterior approach have been described to access this segment. Sundaresan et al. 16,99,100 described an extended approach involving medial claviculectomy and manubriectomy. Ramani et al. 16 published good outcome in a series of patients who underwent anterior, extended (involving medial claviculectomy) approach for debridement of CT lesions. Other similar studies have reported good outcome with extensile anterior approach involving manubriotomy or sternotomy. 16,98 –100,106 Sharan et al. 107 reported that while T1–2 disc could be fully visualised above sternal notch in 45.3% of patients, T2–3 disc could only be exposed in 14.15%. In order to expose T3, conventional anterior approach with manubriotomy may be necessary in 80–85% of patients. 104,107,108
Although, being a transitional zone, reinforcement with posterior stabilisation may be a biomechanically sounder option; a majority of reports in the existing literature seem to suggest a good outcome with anterior debridement and stabilisation alone 99,100,108 (Figure 5). Zhu et al. 105 purported the role of pre-operative CT to assess the relationship of sternal notch with the diseased vertebra. They recommended additional posterior stabilisation whenever the diseased level or the level of distal stabilisation was distal to the notch. Wang et al. 24 reported excellent outcome following combined antero-posterior approach in paediatric CTTB patients. Rajasekaran et al. 35,36,109,110 described the ‘spine-at-risk’ signs for paediatric spinal TB, which include facet subluxation, retropulsion, lateral subluxation and toppling. It has been shown that the presence of these radiological findings can place the spine at a high risk for deformity progression. In cervical or CTTB with positive ‘spine-at-risk’ signs, combined antero-posterior approach may offer better biomechanical advantage. 35,36,109,110
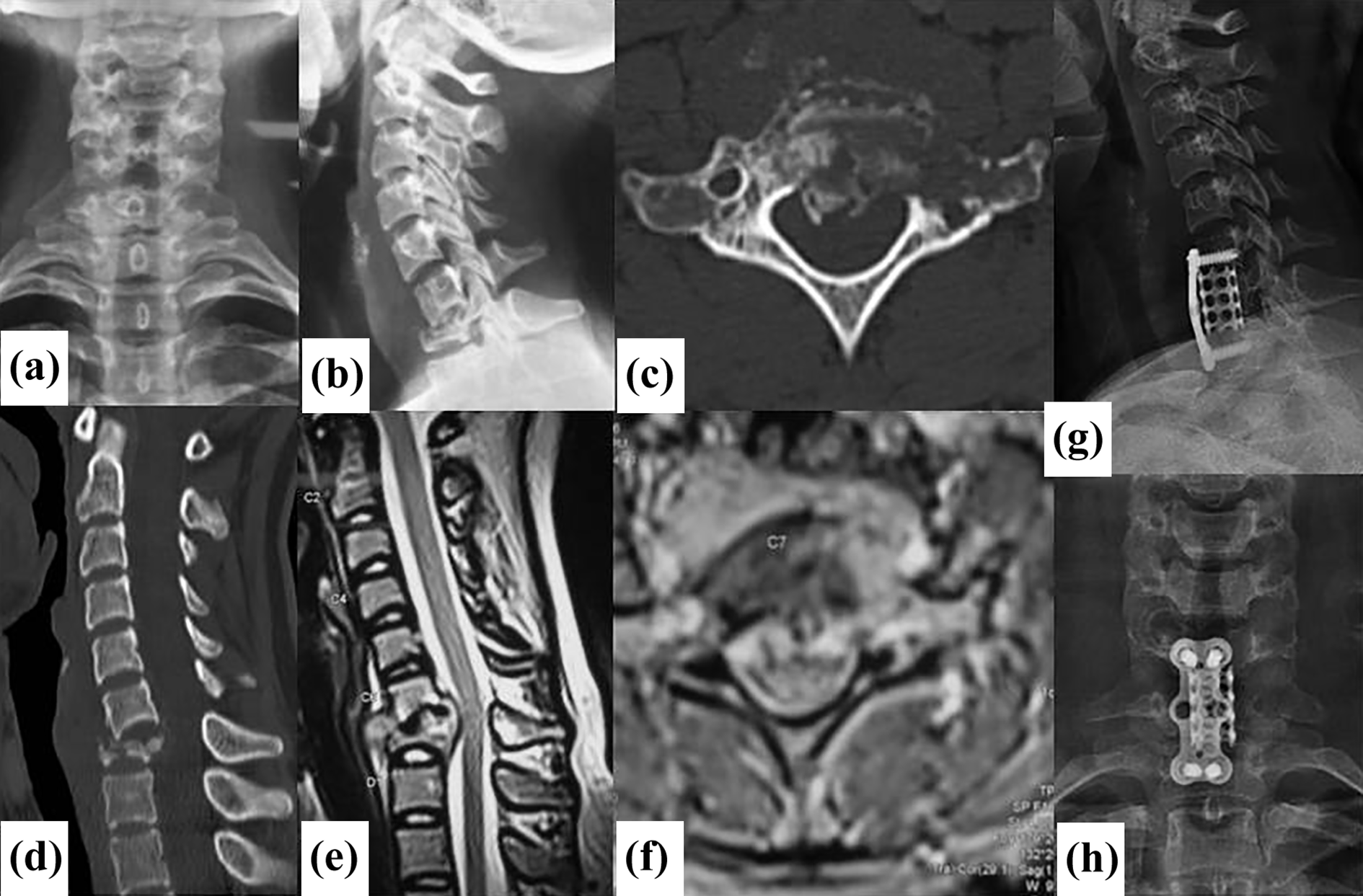
(a) and (b) Antero-posterior and lateral plain radiographs showing significant destruction and involvement of C7 vertebra with collapse; (c) and (d) Mid-sagittal and axial CT images showing significant destruction and collapse of C7 vertebra; (e) and (f) Mid-sagittal T2WI-MRI, and axial T2WI-MRI showing significant collapse and large epidural and paraspinal abscess at C7 level; (g) and (h) Antero-posterior and lateral plain radiographs showing C7 corpectomy and C5–T1 fusion and good healing of CTTB.
Clinical outcome of CTB
Typically, the effectiveness of ATT is evident by 3 weeks and further symptoms continue to improve over time. Eventually, all lesions heal by fibrous union, which further leads onto ossification and stabilisation. 22 Overall, based on the available evidence, the outcome in both conservatively and surgically managed CTB (AATB, SACTB, CCTB) patients has been reported to be largely favourable. 1 –5,111
Conclusion
AATB and SACTB constitute 0.3 to 1% and 3% of spinal TB, respectively. 1 –5 The incidence of neuro-deficit in CTB is significantly more than other spinal TB. 1,5 The general principles of management of CTB are similar to spinal TB elsewhere and medical therapy remains the cornerstone. Surgery is advocated in specific scenarios involving gross neuro-deficit, later stages of disease with significant bony/ligamentous disruptions, altered sagittal balance, drug resistance, and poor response to medications. The surgical approaches for AATB include anterior-alone, posterior-alone and combined approaches, although posterior access is the most preferred. Most of the studies on SACTB have supported the role of anterior approach. Additionally, posterior stabilisation may be necessary in pan-vertebral disease, significant kyphosis, long-segment disease and junctional levels. The overall long-term outcome in CTB is favourable.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.