
Abstract
Purpose:
To report of efficacy repair treatment for meniscus posterior root tears repair.
Methods:
We systematically searched databases including PubMed, Embase, and Cochrane Library for relevant articles. Coleman Methodology Score was used for a quality assessment of the included studies. A meta-analysis was performed to analyze for efficacy of MMPRTs repair.
Results:
Twenty-two studies, 14 level III and 8 level IV, were included in this systematic review, with a total of 926 cases. Studies comparing repair with either meniscectomy or conservative treatment found greater improvement and slower progression of Kellgrene–Lawrence grade with meniscal repair. Decreased meniscus extrusion is beneficial to the prognosis of patients undergoing MMPRTs repair. As treatment efficacy, the Lysholm score increased 28.87 (P < 0.001), IKDC score increased 31.73. The overall pooled event rates of progression of K-L grade is 0.200. Difference of Lysholm score and IKDC score between repair and meniscectomy were 8.72 and 9.67.
Conclusions:
The clinical subjective score after MMPRT repair was significantly improved compared with the preoperative status. Considering the progression of joint K-L grade, it can prevent the progression of arthrosis to some extent, but not completely. Decreased meniscus extrusion is beneficial to the prognosis of patients undergoing MMPRTs repair. Based on these results, MMPRTs repair cloud result favorable outcomes.
Introduction
Compared with tears of the medial meniscal body or horns, medial meniscus posterior root tears (MMPRTs) have a low occurrence rate but are often more difficult to diagnose. Moreover, medial meniscal root tears can change normal biomechanics in the knee, finally causing pain and the early stage of knee osteoarthritis. 1,2 Although advances in orthopedics provide more treatment options, which treatment works best is still controversial. Considering the age of most patients with meniscus root tears, surgeons are reluctant to repair these injuries and often choose non-surgical treatment or meniscectomy. But these two approaches cannot change biomechanics caused by medial meniscal root tears which accelerate the degeneration of the cartilage. 3,4 In contrast to these two approaches, repairing for MMPRTs prevents the development of osteoarthritis by restoring the biomechanics of the knee to normal. Generally speaking, repairing for MMPRTs showed promising results, 5,6 some studies using magnetic resonance imaging (MRI) or second-look arthroscopy have shown increased meniscal extrusion and healed wound in patients. 7,8 Moreover, a number of different techniques have been used for MMPRTs and these techniques shown different efficacies. 9,10
Arthroscopic meniscus repair is an effective method to avoid OA progression and achieve meniscus healing. 5,11 –13 Unfortunately, most published studies were short follow-up and retrospective case series. There have been no reports of randomized controlled studies or large cohort studies; several reviews, including systematic reviews and meta-analysis, 14 –16 have been published with conclusion that MMPRTs repair was an effective and safe treatment compared with other treatment for MMPRTs. However, these reviewers also concluded that more cases and long-term follow-up studies were still needed. Considering that prior reviews included a small number of studies on MMPRTs repair (less than nine) for analysis 14 –16 and that quite a few more studies on MMPRTs repair recently have been published, 17 –24 it is necessary to an updated systematic review and meta-analysis, if appropriate, to evaluate whether the evidence-based support for MMPRTs repair treatment will be strengthened or compromised. Furthermore, a large number of studies may allow us to fully investigate the factors that influence the clinical outcome of MMPRTs repair.
The purpose of this study was to examine the clinical outcomes as well as radiological progression following repair treatment in patients with medial meniscus posterior root tears. We hypothesized that repair for MMPRTs would result in better functional and radiological outcomes comparing with non-repair approaches including meniscectomy and conservative treatment.
Methods
Search strategy
Identification and selection of studies in this review was performed under the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement). A systematic search was performed in PubMed, Embase, the Cochrane Library on November 24, 2020 for all English-language publications. The following search terms were used: (“medial meniscus” OR “medial meniscal”) and (“root tear” OR “posterior horn tear” OR “avulsion”).
Studies which met the following inclusion criteria were reviewed: (1) English-language studies or Chinese-language (2) level I–IV clinical studies of repair treatment options for MMPRTs. The exclusion criteria were as follows: (1) technical notes; case reports; not relevant MMPRTs; abstract only articles, biomechanical studies, and review articles and meta-analyses; (2) studies lacking data on clinical outcomes; (3) non-English language, or non-Chinese language.
Data extraction
Two reviewers independently screened all titles and abstracts to select suitable articles for full-text reviewing. End Note was used to review study and extract data. Data extracted included the publication year, study design, patients’ demographics, interventions, and all clinical and radiographic outcomes.
Quality assessment
The quality of each included study was assessed by independent two reviewers according to the modified Coleman Methodology Score. 25 Ten specific quantitative and qualitative criteria were used in this assessment system: study size; mean follow-up; number of surgical procedures; type of study; diagnostic certainty; description of surgical procedure; postoperative rehabilitation; outcome measures; outcome assessment; and selection process. The final score ranges from 0 to 100, the higher the score, the higher the quality of the evidence.
Outcome measures
The primary outcomes of our study were clinical and radiologic improvement or progression of MMPRTs between the repair treatments and non-repair treatment and outcomes between pre- and post-operation. Indicators used to assess clinical outcomes include International Knee Documentation Committee (IKDC) and Lysholm Activity Scale. Radiologic outcomes were assessed by medial meniscus extrusion changes using magnetic resonance imaging (MRI) and Kellgrene–Lawrence (K-L) grade.
Statistical analysis
All point estimates of analyses and their 95% confidence interval (95% CI) were calculated using random effects models. Heterogeneity was assessed using the Q-test and by calculating I 2 . If the p-value was below 0.05 in the Q-test and/or the I 2 index was higher than 50%, the pooled analysis was considered to be significantly heterogeneous, the random effects model was used.
For subgroup meta-analyses, continuous variables such as the Lysholm knee score, IKDC score, were extracted as means and standard deviations. Binary outcomes were pooled as prevalence (progression rates of K-L grade), SE or the 95% CI can be calculated as following formula: When the prevalence data does not satisfy a normal distribution, use formulas as follows:
All analyses were carried out with the RevMan 5.4 statistical software (The Nordic Cochrane Centre, Copenhagen, Denmark, http://ims.cochrane.org/revman/download) in Windows 10.
Results
A total of 402 unique studies were identified for review. A flow chart regarding the screening of the articles is shown in Figure 1; 22 studies were selected for full-text review, all of which satisfied our inclusion and exclusion criteria; 4 studies included partial meniscectomy groups, 2 studies included conservative groups, all studies included repair groups. In the 22 studies, 14 were Level III evidence, 5,9 –13,17 –20,22,27 –29 8 were Level IV evidence. 6 –8,21,24,30 –32 Among the Level III evidence comparative studies, three compared partial meniscectomy with pull-out suture repair 9,13,27 and one compared conservative treatment with pull-out suture repair, 28 one compared meniscectomy, repair and conservative treatment. 11 The rest of the studies reported subgroup analysis of repair treatment of MMPRTs, 5,10,12,17 –20,22,29 including different surgical technique 5,10,18,20,22,29 and meniscus extrusion changes after repair of MMPRTs. 12,17,19 Of the Level IV case series studies, eight studies reported the outcomes of repair in MMPRTs.
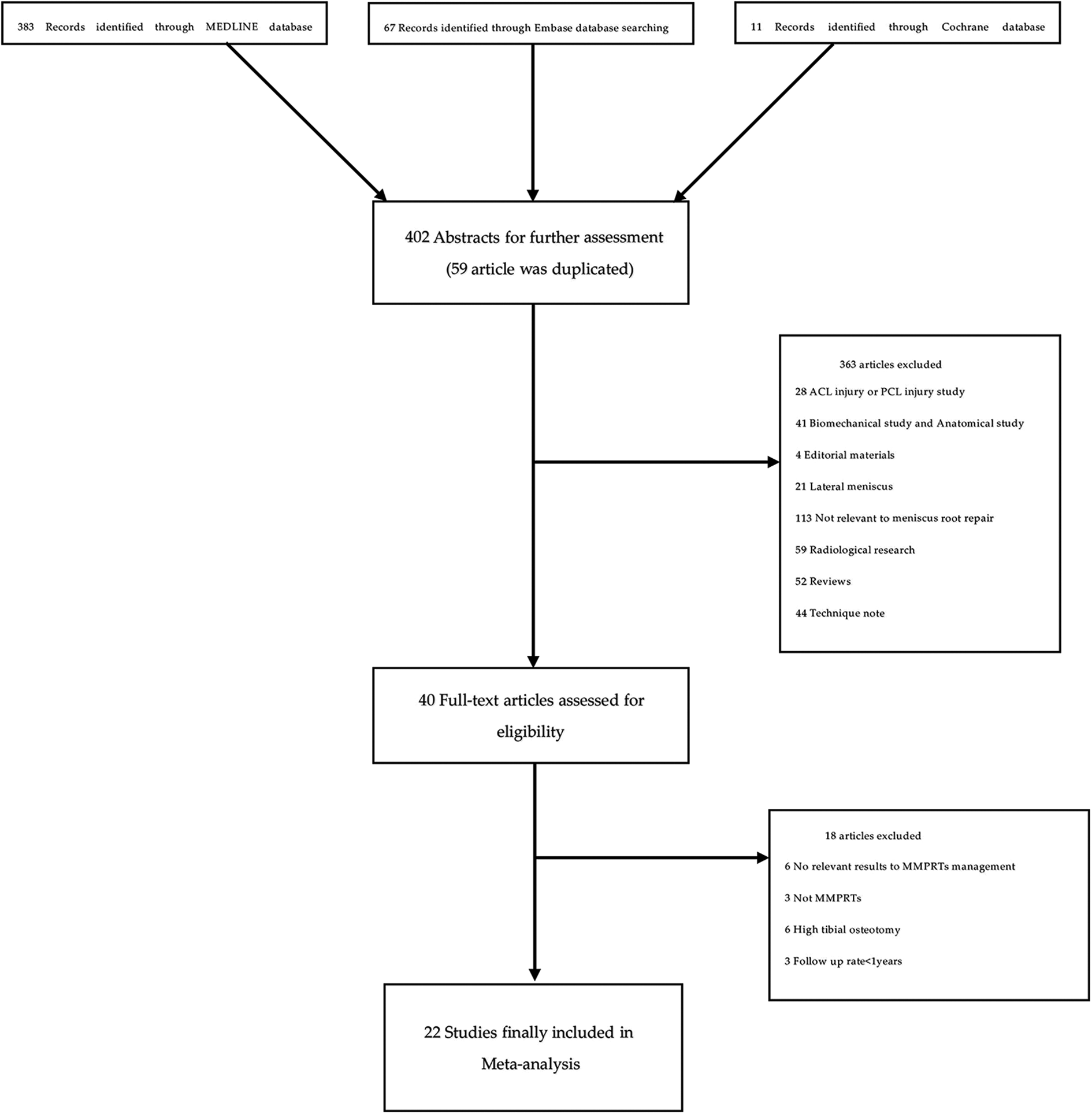
Systematic review algorithm using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
The mean modified Coleman Methodology Score was 67.7 ± 4.1. The corresponding values for each study are shown in Table 1. In the section A, the average score for the study size was 5.5; the average score for the mean follow-up, number of procedure, type of the study, diagnostic certainty, surgery description and rehabilitation description were 4.3, 10, 0.5, 5, 5, 5.2, respectively. In the section B, the average score for the outcome criteria, the procedure for outcome and the selection process were 10, 7, 15, respectively.
Level III studies.

mCMS: modified Coleman Methodology Score; HSS: Hospital for Special Surgery; IKDC: International Knee Documentation Committee; K-L: Kellgrene–Lawrence; KOOS: Knee Injury and Osteoarthritis Outcome Score; VAS: visual analog scale; TLS: two loop stitches; TSS: two simple stitches; MAS: Mason-Allen stitch; F-MMA: FasT-Fix Modified Mason-Allen.
A total of 919 patients (926 cases) were included in this system review. Of these, 786 patients (793 cases) undergone MMPRTs repair surgery in all of the studies. 5 –13,17 –22,24,27 –32 The remaining 133 patients (133 cases) were treated with non-operative methods 11,28 or partial meniscectomy. 5,11,13,27
Among the 14 level III studies(Table 1) included in this review, 3 compared meniscal repair with meniscectomy, 9,13,27 1 compared repair with conservative treatment, 28 9 compared distinct repair groups, such as increased extrusion vs decreased extrusion or repair techniques, 9 –12,17,19,20,22,29 1 cohort study compared the efficacy of non-operative management, meniscectomy, and repair. 11 Meniscal repair resulted in significant improvement in functional outcomes scores in all studies. Clinic result with repair was significantly greater in the one study comparing it with conservative treatment of MMPRTs 28 and three studies comparing meniscectomy. 5,13,27 Meniscal repair resulted in significant improvement in functional outcomes scores in all studies. Functional improvement with repair was significantly greater in the most studies comparing it with other treatment of MMPRTs, but there were differences between the different repair techniques. 10,22,29 Moreover, changes in meniscus extrusion affect the clinic outcomes after MMPRTs repair, three studies reported their findings 12,17,19 and the results were similar. Chung et al. 12 reported that patients with decreased meniscus extrusion had better surgical outcomes in terms of clinical scores and radiographic findings, indicating the importance of reducing meniscus extrusion. In another study, Moon et al. 19 found no significant difference in postoperative clinical scores between patients with reduced or maintained meniscus extrusion and those with increased meniscus extrusion; however, the progression of osteoarthritis was delayed in the patients with reduced or maintained meniscus extrusion. Although, Yanagisawa et al. 17 reported that the radiographic findings did not significantly differ between increased meniscus extrusion group and reduced or maintained meniscus extrusion group, the postoperative K-L grade was significantly worse than the preoperative K-L grade in the group with increased meniscal extrusion at 1 year postoperatively. These results indicated that the progression of arthritic changes can be prevented by preventing meniscal extrusion after MMPRTs repair.
Of the eight level IV studies (Table 2) included in this systematic review, all studies focused on repair of MMPRTs. 6 –8,21,24,30 –32 All studies showed improvement in clinical outcomes for repair of MMPRTs. Lee et al., Liu et al. and Nha et al. 6,24,32 reported that a significant improvement in both radiographic and clinical outcomes with patients undergone repair treatment. Three studies used second-look arthroscopy to evaluate surgical outcomes. 8,21,24 Seo et al. 8 found that all patients showed clinical improvement despite findings of incomplete or failed healing on second-look arthroscopy after repairing. However, Lee et al. 30 reported that the healing status of the repaired meniscus may relate to clinical outcomes, the stable healed meniscus showed better clinical outcomes and have less complaint compared with unhealed meniscus. Moon et al. 7 identified varus alignment, and degree of cartilage damage as worse prognostic factors for MMPRTs repair, increased meniscus extrusions provided patients with a clinical benefit. By cartilage damage of the medial compartment in patients postoperatively, Kodama et al. 21 suggested that early repair surgery for MMPRTs should be undertaken for patients with mild osteoarthritic knee.
Level IV studies.

mCMS: modified Coleman Methodology Score; HSS: Hospital for Special Surgery; IKDC: International Knee Documentation Committee; K-L: Kellgrene–Lawrence; KOOS: Knee Injury and Osteoarthritis Outcome Score; VAS: visual analog scale; ICRS: International Cartilage Repair Society.
Twelve studies reported incidence of K-L grade progression 5,6,9,12,13,17,19,20,27,29,30,32 ; for the K-L grade progression in the repair group, a total of 169 cases was reported while 55 cases were reported in meniscectomy group. Three studies reported rates of conversion to TKA (total knee arthroplasty). Kim et al. 5 reported that three patients treated by partial meniscectomy finally underwent TKA at a mean of 17.8 months after meniscectomy because of advanced osteoarthritis. Bernard et al. 11 reported nine patients treated with meniscectomy and four patients treated with no operation underwent TKA. Seven patients treated with meniscectomy underwent conversion to TKA in Chung’s study 13 ; in contrast, none of the patients who underwent repair surgery required TKA.
Meta-analysis of the efficacy of MMPRTs repair
Lysholm scores
After excluding 5 studies and 7 subgroups that did not include the SD, a total of 16 studies 5 –7,9,10,12,13,17 –22,24,27 –30 and 25 subgroups including 669 patients were used to evaluate the treatment effect. Mean differences were investigated to determine the overall best estimate of 28.87 with [27.91, 29.84] as the 95% confidence interval (CI), measured in SD units of the difference scores (P < 0.001). A forest plot of paired standardized mean differences is presented in Figure 2.

Lysholm forest plot of meniscal repair studies. CI: confidence interval; IV: inverse variance; SD: standard deviation.
IKDC scores
A total of 13 studies or subgroups 5,9,10,12,13,19 –22,24,27,29,30 including 541 patients were used to evaluate the IKDC improvement. The pooled improvement in IKDC scores was 31.73 with [29.79, 33.66] as the 95% confidence interval (CI), measured in SD units of the difference scores (P < 0.001). A forest plot of paired standardized mean differences is presented in Figure 3.
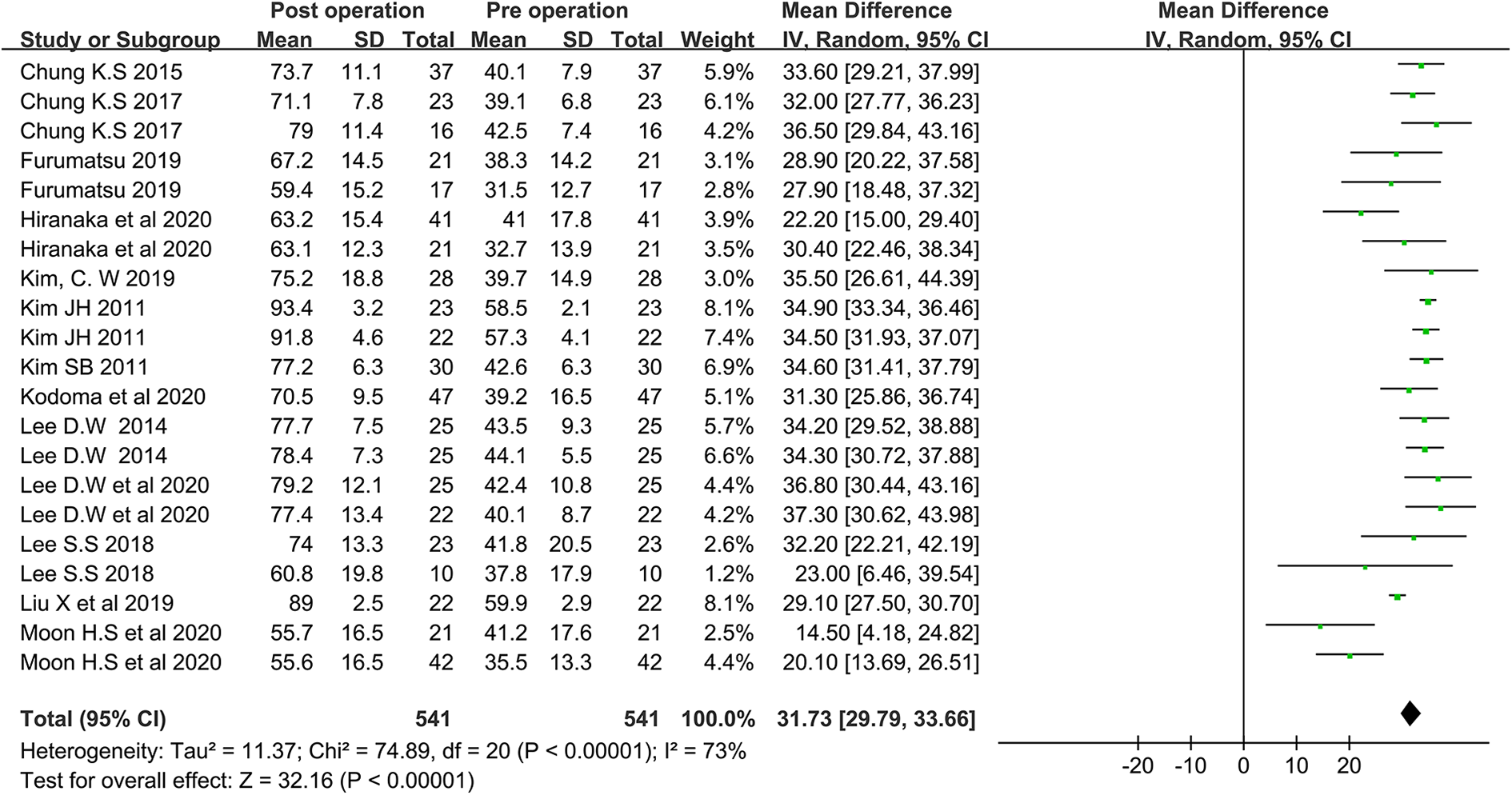
IKDC forest plot of meniscal repair studies. CI: confidence interval; IKDC: International Knee Documentation Committee; IV: inverse variance; SD: standard deviation.
Progression of K-L grade
After excluding three studies 12,13,27 which brought great heterogeneity. The pooled K-L progression rate of meniscal repair is 0.200 (95% CI, 0.145–0.270). The detailed calculation procedure is as follows: When the prevalence data does not satisfy a normal distribution, use formulas as follows 26 :

X is the number of occurrences of an event
n is the total number of observed objects+
The summary OR/RR calculated via Revman was 0.25, (95% CI, 0.17–0.37), Figure 4. Then use formulas as follows:

Finally, K-L progression rate of meniscal repair = 0.25/(1 + 0.25) = 0.200, 95% CI lower-limit = 0.17/(1 + 0.17) = 0.145, 95% CI upper-limit = 0.37/(1 + 0.37) = 0.270.

Forest plot of pooled event rate of the progression of arthrosis graded by Kellgren–Lawrence grade. CI: confidence interval; IV: inverse variance; SE: standard error.
Differences between repair and meniscectomy
Differences of Lysholm scores between meniscal repair were not as consistent however, with an MD of 8.72 (95% CI, −0.67 to 18.11, Figure 5), similar findings were found for IKDC scores with an MD of 9.67 (95% CI, −2.31 to 21.65, Figure 6).

Forest plot of Lysholm Score differences. CI: confidence interval; IV: inverse variance; SD: standard deviation.

Forest plot of IKDC Score differences. CI: confidence interval; IV: inverse variance; SD: standard deviation.
Discussion
The primary outcomes of this study were to review changes in functional outcomes and the rate of conversion to TKA and progression in K-L grade for the repair treatments of MMPRTs. Based on a systematic review of the literature on MMPRTs therapy, it is clear that, although many prognostic factors may play a role, repairing for MMPRTs has the best clinical and radiographic results compared with meniscectomy and conservative treatment.
Comparative analysis of clinical and radiologic outcomes for the treatment of MMPRTs demonstrated the best results with surgical repair over meniscectomy and conservative groups. For the repairing treatment, the available data showed better functional outcome scores for patients comparing with meniscectomy. Three surface-level comparison of the repair treatment of MMPRTs versus meniscectomy of MMPRTs revealed a better result in repaired meniscus with an MD of 9.67 (95% CI, −2.31 to 21.65) in IKDC scores and an MD of 8.72 (95% CI, −0.67 to 18.11) in Lysholm scores. Moreover, given that meniscectomy does not restore hoop tension, it results in biomechanical changes to a worsen situation. Because of decreasing tibio-femoral contact area and increasing pressure on the residual intact meniscus, biomechanical situation of a keen after meniscectomy is similar to a totally meniscectomized knee. 4 Repair of MMPRTs restores the biomechanics to the normal knee joint 33 and can prevent or delay osteoarthritis progression. In this study, K-L grade is used to evaluate osteoarthritis progression, the pooled event rate was calculated as 0.200 (95% CI, 0.145–0.270). Considering the rough estimate of 95% confidence interval, 20.0% of patients had progression of joint K-L grade; therefore, a minimum of 73.0% and a maximum of 85.5% of patients with meniscus dysfunction due to MMPRTs could avoid degenerative changes via MMPRTs repair. Meanwhile these patients can also recover the function of meniscus through MMPRTs repair, the pooled improvement in IDKC scores was 32.41, (95% CI, 31.60, 33.23) and Lysholm scores was 28.87, (95% CI, 27.91–29.84). This suggests that repair treatment for MMPRTs can not only reduce symptoms in a short time, improve functional scores but also prevent long-term joint degeneration in the future.
Partial meniscectomy was described as a traditional treatment for MMPRT. However, reports of partial meniscectomy in MMPRT or comparative studies between repair and meniscectomy are few. Ozkoc et al. 34 reported that the mean Lysholm score improved from 53 to 67 (mean age 55.8 years; follow-up duration 56.7 months). The average K-L grade improved from 2 preoperatively to 3 at the last follow-up which indicates a worsen change. Han et al. 35 reported unsatisfactory results of partial meniscectomy for MMPRTs with mean Lysholm score improved significantly from 72 preoperatively to 77 at the final follow-up, and 35% patients showed progression in the K-L grade. Four comparative studies in this study 5,11,13,27 compared repair and partial meniscectomy, the pooled differences of IKDC scores 9.67 (95% CI, −2.31 to 21.65) demonstrated advantages of repair surgery. Results in progression of the K-L grade suggested that the repair group demonstrated significantly reduced progression of arthrosis than the partial meniscectomy group; especially in Chung’s study, 13 100% of patients. Therefore, compared with partial meniscectomy, meniscus repair seems to improve clinical score and prevent or delay joint progression.
Meniscus extrusion is an important radiological parameter to evaluate the degenerative changes of knee joint. The changes of meniscus extrusion are considered to be related to meniscus degeneration, extensive meniscus tears, medial joint space stenosis and medial femoral condylar cartilage lesions, resulting in the progression of knee osteoarthritis. 36 –38 As meniscus extrusion can closely reflect the tension of meniscus hoop, 39 the postoperative evaluation of meniscus extrusion is very important to predict the prognosis of patients who undergo MMPRTs repair surgery. However, the results of the study on the changes of postoperative meniscus extrusion are contradictory, 12,1616,40 suggesting that there may be related factors affecting the progress of postoperative meniscus extrusion and prognosis of patients. In this study, changes in meniscus extrusion affect the clinic outcomes after MMPRTs repair, three studies reported similar results. 12,17,19 These results indicated that a decreased or maintained meniscal extrusion after MMPRTs repair means favorable clinical outcomes or at least better radiological results.
This system review has several limitations. First, there are only five studies directly compared different treatment measures in this review. Three studies compared clinic and radiographic outcomes between the meniscectomy group and the repair group. One study compared the results of meniscus repair with conservative treatment, and one compared the results of three different treatments including repair, meniscectomy and conservative treatment, but data in this study is not clear. Other studies include heterogeneous case series or comparative studies that describe subgroup analysis. Therefore, it is hard to combine the results of different studies that compare different treatment measures. In addition, none of the studies included in this review are randomized. Because of the small sample size and the heterogeneity of the result parameters, the significance of overall statistical analysis is limited. Second, the quality of all studies is only III- and IV-level evidence, which means that many of the included studies have potential selection biases, which may affect clinical and radiological outcomes. Third, due to the lack of long-term follow-up studies, it is impossible to evaluate the long-term prognosis of patients with or without MMPRT repair. The longest follow-up period for all studies was more than 5 years, and there was only one article. Long-term biomechanical changes of the knee joint may have a negative impact on the progress of the joint, the change of symptoms and the score of knee joint function. Fourth, the inclusion criteria of none of the patients are uniform, which is biased against the results of the study. In order to clarify the effectiveness of MMPRTs repair, it is necessary to conduct a meta-analysis of all existing MMPRTs case series and comparative studies. This study attempts to reduce bias by including more updated studies. In the future, more well-organized, long-term follow-up, large sample size comparative studies, especially the direct comparison of different treatment methods, are needed to evaluate the effects of MMPRT repair.
Conclusions
The clinical subjective score after MMPRT repair was significantly improved compared with the preoperative status. Considering the progression of joint K-L grade, it can prevent the progression of arthrosis to some extent, but not completely. Decreased meniscus extrusion is beneficial to the prognosis of patients undergoing MMPRTs repair. Based on these results, MMPRTs repair cloud result favorable outcomes.
Supplemental material
Supplemental Material, sj-doc-1-osj-10.1177_23094990211003350 - The efficacy of meniscus posterior root tears repair: A systematic review and meta-analysis
Supplemental Material, sj-doc-1-osj-10.1177_23094990211003350 for The efficacy of meniscus posterior root tears repair: A systematic review and meta-analysis by Lifu Wang, Kun Zhang, Xuening Liu, Zhongcheng Liu, Qiong Yi, Jin Jiang and Yayi Xia in Journal of Orthopaedic Surgery
Footnotes
Author Contribution
LIfu Wang and Kun Zhang contribute to this work equally.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81874017, 81960403 and 82060405); Lanzhou Science and Technology Plan Program (2018-3-52); Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (CY2017-QN12, CY2017-QN11); and the Fundamental Research Funds for the Central Universities (lzujbky-2020-kb17).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.