
Abstract
Background:
The posterior approach (PA) is the most commonly used surgical approach for total hip arthroplasty (THA), but the proximity of the sciatic nerve may increase the likelihood of sciatic nerve injury (SNI). Gluteus maximus tenotomy can be performed to prevent SNI because tenotomy increases the distance between the femoral neck and sciatic nerve and prevents compression of the sciatic nerve by the gluteus maximus tendon (GMT) during hip movements. We aimed to kinematically compare the postoperative hip extensor forces of patients who have and have not undergone gluteus maximus tenotomy to determine whether there is a difference in hip extensor strength.
Methods:
Seventy-two patients who underwent gluteus maximus tenotomy during THA were included in the group 1, and 86 patients who did not undergo tenotomy were included in group 2. The Harris hip score, body mass index and hip extensor forces were measured both preoperatively, and 6 months after surgery with an isokinetic dynamometer and compared.
Results:
The mean age was 64.6 ± 2.3 years in group 1 and 63.8 ± 2.1 in group 2. Mean body mass index was 25.7 ± 1.1 in group 1, and 25.5 ± 1.3 in group 2. Baseline Harris hip score (HHS) was 42.36 ± 12 in group 1 and 44.07 ± 9.4 in group 2 (p = 0.31), whereas it was 89.1 ± 7.8 and 88.4 ± 8.1 at 6 months after surgery, respectively. Baseline hip extensor force (HEF) was 2 ± 0.4 Nm/kg in group 1, and 2.1 ± 0.7 Nm/kg in group 2 (p = 0.28), while it was 2.4 ± 0.6 Nm/kg, and 2.5 ± 0.5 Nm/kg, respectively at 6 month follow-up (p = 0.87). Both groups had significantly improved HHS and HEF when comparing baseline and postoperative measurements (p < 0.0001). No cases of sciatic nerve palsy were noted in group 1, whereas there were two (2.32%) cases in group 2, postoperatively.
Conclusion:
The release of the GMT during primary hip arthroplasty performed with the PA did not lead to significant decrease in hip extension forces. Hip extensor strength improves after THA regardless of tenotomy. Gluteus maximus tenotomy with repair does not reduce muscle strength and may offer better visualization.
Introduction
Primary total hip arthroplasty (THA) for hip osteoarthritis is a successful and cost-effective surgical option that relieves pain, restores function, and improves patients’ overall quality of life. 1 Although the benefits of hip replacement surgery outweigh the risks, some surgical complications, such as sciatic nerve injury (SNI), can be devastating.
The prevalence of SNI after THA ranges from 0.3 to 3.7%. 2 This major complication may severely have impact on both patients and surgeons. Postoperative hematomas, injuries due to traction for leg positioning and the pressure of the retractors, nerve stretching due to leg lengthening, cement protrusion in cemented prostheses, and compression due to trochanteric wires and grafts used for stabilization may lead to SNIs; however, in more than half of the SNI cases that occur, the cause is unknown. 3,4 Since many factors can cause nerve palsy, more preventative measures need to be taken.
The posterior approach (PA) is the most commonly used surgical approach worldwide for THA. 5 Although the PA has disadvantages, it provides satisfactory visualization of both the acetabulum and the femur and the lowest rate of overall complications among all the approaches. 6 However, the proximity of the sciatic nerve to the posterior structures may increase the likelihood of nerve damage through the PA. Furthermore, the course of the sciatic nerve may change during maneuvers for hip dislocation and relocation. Studies have shown that the sciatic nerve begins to move closer to the femoral neck due to increased hip flexion after dislocation of the hip and femoral neck osteotomy. 3 Careful and soft tissue-friendly surgery may not sufficiently remove the sciatic nerve from the osteotomy site to reduce the risk of strain. The release of the GMT increases the distance between the femoral neck and the sciatic nerve, especially at 90° of flexion of the hip, and facilitates hip dislocations without significant nerve disruption. 7 Tenotomy also prevents the GMT from compressing the sciatic nerve during internal rotation and flexion of the hip. 3 Theoretically, weakness of gluteus maximus in a healthy subject without hip osteoarthritis may lead to deterioration in rapid acceleration of the body upward and forward from a position of hip flexion, such as when pushing off into a sprint, arising from a deep squat, or climbing a steep hill. 8 However, no clinical studies reporting any possible disadvantage of the tenotomy or its association with gluteal muscle insufficiency in hip arthroplasty have been found in the literature. In our study, we aimed to kinematically compare the postoperative hip extensor forces of patients who did and did not undergo gluteus maximus tenotomy in THA with the PA to determine whether hip extensor strength decreases due to gluteus maximus tenotomy.
Materials and methods
This single-center prospective comparative study was approved by the institutional review board of our hospital, and written informed consent was obtained from all subjects. A total of 158 patients who were diagnosed with primary coxarthrosis and underwent THA between January 2016 and September 2018 were included in the study. Patients with spinal disorders (the most important risk factor for the development of SNI is the preexistence of a lumbar spinal disease), 9 truncal deformities, developmental hip dysplasia, neuromuscular diseases or any other cause of secondary osteoarthritis were excluded. All human and animal studies have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants were informed of the purpose of the study and signed and returned informed consent forms. The study was approved by our Institutional Review Board.
Patients were randomly selected with the sealed envelope method to undergo surgery with one of two methods considering the time of admission to the hospital. Seventy-two patients (42 female and 30 male) who underwent gluteus maximus tenotomy were included in group 1, and 86 patients (46 female, 40 male) who did not undergo tenotomy were included in group 2. Forty-two patients in group 1 and 36 patients in group 2 had well-controlled type 2 diabetes mellitus.
Outcome measurement
Body mass adjusted hip extensor forces were measured both preoperatively, and at 6 months after surgery with a CSMI Human Norm II isokinetic dynamometer (Figure 1). Five repetitive measurements were taken in supine and lateral (lying on the sides) positions. The patients were verbally encouraged to do “their best,” and the highest values of the Harris hip score were also recorded and analyzed for both baseline and at the 6th month, postoperatively.

Hip extensor forces were measured with a CSMI Human Norm II isokinetic dynamometer.
The patients were examined for any evidence of motor weakness in the extensor hallucis longus, ankle dorsiflexors or plantar flexors immediately after the effect of spinal anesthesia dissipated. Any findings of sensory and motor weakness were noted to record signs of sciatic nerve palsy.
Surgical procedure
All surgeries were performed by the same surgical team. The section of the sciatic nerve from under the piriformis muscle to the distal region of the gluteus maximus was completely exposed (Figure 2). Dissection and clear visualization of the GMT was achieved in the patients in both groups, and afterwards, tenotomy was performed only for group 1 by leaving 1 cm of the tendon where the gluteus maximus inserts into the vastus lateralis muscle and gluteal tuberosity base before femoral neck osteotomy was performed (Figure 3). The tendon was gently reattached by absorbable sutures at the end of the implantation procedure.
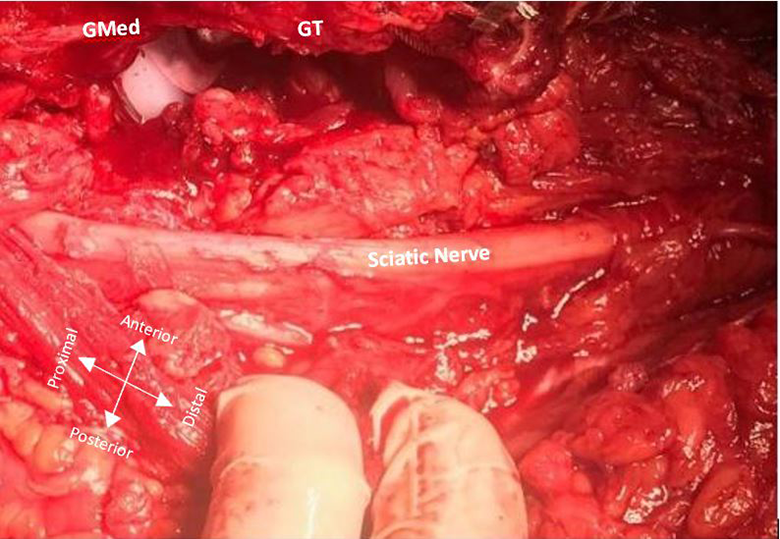
The path followed by the sciatic nerve was completely exposed. Gmed: Gluteus medius muscle, GT: Greater trochanter.

Intra-operative view of the left hip wih posterior approach. The gluteus maximus tendon was identified, and tenotomy was performed with consideration of the sciatic nerve passing under it (
Post-operative rehabilitation
The Vancouver Coastal Health (VCH) rehabilitation program was implemented for both groups after surgery. 10 The VCH rehabilitation program consists of exercises and positions used to reduce the forces on the hip in the early postoperative period (first 6 weeks) to prevent dislocation of the hip joint. The program includes breathing exercises to improve pulmonary functions, the use of compression socks to prevent thromboembolic events, active massage, and hip range of motion (ROM), strengthening, balance, and proprioception exercises.
Statistical analysis
The mean, standard deviation, minimum, maximum, frequency and ratio values were used as the descriptive statistics of the data. The Kolmogorov-Smirnov test was used to assess the distributions of the variables. The quantitative data were analyzed with independent t tests to determine whether there was a statistically significant difference between groups. To compare groups in terms of neuropathy, the chi-square test was performed. IBM SPSS Statistics 22 (SPSS IBM, Chicago, Ill., USA) was used for statistical analysis. P < 0.05 was considered significant.
Results
Seventy of the 158 (44.3%) patients were male, and 88 (55.6%) were female. The mean age was 64.6 ± 2.3 years in group 1 and 63.8 ± 2.1 in group 2. Mean body mass index was 25.7 ± 1.1 in group 1, and 25.5 ± 1.3 in group 2. Baseline Harris hip score (HHS) was 42.36 ± 12 in group 1 and 44.07 ± 9.4 in group 2 (p = 0.31), whereas it was 89.1 ± 7.8 and 88.4 ± 8.1 at 6 months after surgery, respectively. Baseline hip extensor force (HEF) was 2 ± 0.4 Nm/kg in group 1, and 2.1 ± 0.7 Nm/kg in group 2 (p = 0.28), while it was 2.4 ± 0.6 Nm/kg, and 2.5 ± 0.5 Nm/kg, respectively at 6 month follow-up (Table 1) (p = 0.87). It was concluded that final extensor hip strength was not lower in the tenotomy group than in the control group.
Summary of patient demographic characteristics, baseline and final outcome measures.

Both groups had significantly improved HHS and HEF when comparing baseline and postoperative measurements (p < 0.0001). No cases of sciatic nerve palsy were noted in group 1, whereas there were two (2.32%) cases in group 2, postoperatively. Neuropraxia with silent spontaneous activity on electromyography that lasted approximately for 6 months was observed in these cases. Those patients were fitted with an ankle-foot orthosis before being discharged from the hospital. Fortunately, these patients had already fully recovered from nerve palsy at the time of the 1-year follow-up.
Discussion
The baseline and final hip extensor forces of patients who did and did not undergo gluteus maximus tenotomy in THA with the PA were compared to determine whether hip extensor strength decreases due to gluteus maximus tenotomy with repair. We demonstrated that gluteus maximus tenotomy with repair in THA did not reduce hip extensor strength at 6 months postoperatively when compared to those who did not receive tenotomy during surgery. Besides, both groups had significant improvement in final HEF compared to baseline levels. Relieving the pain after THA allows for increased daily activity, which can also lead to improved muscle function. 11 This may be under favor of improvement in hip range of motion via artificial replacement of the arthritic joint, together with recovery form impaired gait and balance by postoperative rehabilitation program. 12,13
Several studies have clearly demonstrated that gluteus maximus tenotomy did not lead to loss in hip extensor strength, even left unrepaired. Chughtai et al. performed nerve decompression surgery by partial GMT release for patients with sciatic nerve palsy after total hip arthroplasty and indicated that all patients had full recovery to 5/5 muscle strength including hip extensors by 12 weeks, postoperatively. 14 Polesello et al. described endoscopic GMT release for external snapping hip syndrome and completely transected the femoral insertion of the GMT using a radiofrequency device close to the linea aspera until the tenotomy was complete in 8 patients. They stated that all patients returned to their previous activity level without any complaint of weakness at 22-month follow up. 15 Similarly, Liu et al. retrospectively reviewed 108 patients with bilateral gluteal muscle contractures who had arthroscopic gluteal muscle release and reported no residual hip pain or gluteal muscle wasting at a minimum of 7 months follow up. 16
The probability of nerve damage due to possible ischemic and mechanical causes after THA surgery is 0.3%–3.7%. 2 Although the incidence of SNI with clinical findings is low, it is known that subclinical nerve injuries, which can be diagnosed by electrodiagnostic imaging during surgery, are more common. 17 Schmalzried et al. 4 reported that sciatic nerve damage occurs in 79% of all postsurgical nerve damage cases. The female sex and presence of developmental hip dysplasia increase the risk of nerve damage.
After the sciatic nerve exits the pelvis from the sciatic notch, it travels distally through the deep gluteal space. The deep gluteal space, where sciatic nerve compression mostly occurs, consists of the gluteus maximus posteriorly, posterior acetabular column anteriorly, gluteal tuberosity laterally, sacrotuberous ligament medially, inferior margin of the sciatic notch superiorly, and ischial tuberosity inferiorly. 18 The sciatic nerve may be injured in this area due to direct surgical trauma, excessive traction, intraoperative compression due to leg positioning in flexion, adduction during femoral preparation, the effect of heat from the cement, improperly placed retractors, and grafts or cables applied for stabilization and subgluteal hematomas. Despite all these known causes, the cause is unfortunately unknown in 50% of cases of SNI. 4
The superior fibers of the gluteus maximus, the largest fibers, insert broadly on the iliotibial tract, but the deep fibers of the inferior part attach to the gluteal tuberosity immediately distal to the quadratus femoris, and this attachment is called the “gluteal sling.” 19 The sciatic nerve lies medial and deep to the gluteal sling at this level. Hip flexion and internal rotation during THA tighten the gluteal sling and compress the nerve against the ischial tuberosity. 20
There are two clinical explanation for the compression phenomenon. Nerve damage in these patients is not permanent, and the majority of patients recover completely within 1 year. Peroneal involvement is more prominent in patients with nerve lesions because peroneal fascicles are located superiorly and more tightly packed in the sciatic nerve. 21
The three frequently preferred surgical approaches during hip arthroplasty, the direct anterior, direct lateral, and posterior approaches, have their own disadvantages and advantages, although the surgeon’s experience and the patient’s medical records are important in choosing the type of incision. The anterior approach uses the interval between the rectus femoris and gluteus medius muscles; therefore, it is a muscle-sparing incision with low dislocation rates and leads to the early restoration of gait kinematics. The lateral approach, in which the joint capsule is reached by splitting the gluteus medius and vastus lateralis, has advantages such as extensile exposure to the femur, if needed, and a low dislocation rate. 22
The PA to the hip for THA is the most common surgical approach used worldwide. 5 This approach involves splitting the gluteus maximus, performing tenotomy of the piriformis and other short rotator tendons and finally, reaching the posterior capsule. With this surgical approach, if the whole course of the sciatic nerve is exposed proximally and distally and the short rotator tendons are directed backward to cover the sciatic nerve, the nerve can be protected. Although compared with other approaches, the PA has the advantages of providing extended exposure for the femur and acetabulum in primary and revision surgeries, and the sciatic nerve can be monitored and protected comfortably throughout the entire procedure, the more frequent occurrence of dislocation is an important disadvantage. Pellicci et al. 23 reported that performing good soft tissue repair, including the repair of short external rotators, the posterior capsule, and the quadratus femoris, significantly reduced the dislocation rate from 4% to 0%.
Although it is thought that the risk of SNI may be higher with the PA due to the anatomical proximity of the sciatic nerve to posterior structures, Navarro et al. did not find any differences between the lateral and posterior approaches. 24 Robinson et al. 25 even found that this risk may be slightly higher with the lateral approach. For our study, we preferred the PA, as we are more experienced with this approach and it can fully reveal the course of the sciatic nerve and its relationship with the GMT.
With internal rotation and flexion of the hip, the sciatic nerve becomes closer to the femoral neck, while the gluteal sling begins to compress the nerve distally. 3,7 Nerve damage may vary depending on the amount and duration of the pressure applied. A pressure increase of as little as 20 mmHg may result in venous stasis, which may lead to extraneural edema, whereas a 80 mmHg pressure increase stops all intraneural blood flow. 26 It is known that accompanying diabetes as a concomitant disease in these patients will cause the nerve to be more sensitive due to compression-related edema. 27 In our study, nearly half of the patients in each group were diagnosed with regulated diabetes mellitus.
Gay et al. 20 showed that the release of the GMT significantly reduces the pressure on the sciatic nerve. Hurd et al. 21 reported that sciatic nerve palsy occurred in 2 patients after hip arthroplasty and showed with MRI that the sciatic nerve was trapped under the GMT. The authors did not observe any sciatic nerve lesions among 752 hips undergoing full release of the GMT but reported 3 patients with nerve damage among 804 hips that did not undergo tenotomy and were included in the control group. 19 Paiva et al. 28 performed gluteus maximus tenotomy in a patient with 5.5 cm limb dysmetria who underwent hip replacement surgery, and they assessed the fibular and tibial branches of the sciatic nerve before and after tenotomy with electro neurophysiological monitoring. The authors found that tenotomy especially improved the motor response of the fibular component of the sciatic nerve. 28
There are numerous studies in the literature on the somatosensory evoked potential (SEP) changes in the sciatic nerve that occur due to compression during joint positioning. 17,29,30 For example, Stone, Black and Pereles reported that extremity positioning, especially during the preparation of the femoral canal, causes SEP changes, regardless of the type of incision selected. We did not find any studies published in English on the clinical effects of gluteus maximus tenotomy on hip extension. Our study was the first to show that there is no significant loss in hip extension forces after gluteus maximus tenotomy and that tenotomy reduces the risk of sciatic nerve palsy.
The most important limitation of our study is that comparing the hip extension forces that were measured in osteoarthritic hip to those measured in artificial hip could cause misleading results in evaluating the extension forces due to mechanical blocks in the joint itself, pain and functional limitations. For this reason, we interpreted the results with respect to the control group, which included patients with similar characteristics who did not undergo tenotomy during surgery. Another limitation was that the patient was placed in the supine and lateral positions rather than the standing position and leaning forward during the kinematic hip measurements. Last, studies with larger sample sizes would yield more accurate and reproducible outcomes.
Conclusion
The release of the GMT during primary hip arthroplasty performed with the PA did not lead to significant decreases in hip extension forces. Hip extensor strength improves after THA regardless of tenotomy. Gluteus maximus tenotomy with repair does not reduce muscle strength and may offer better visualization.
Footnotes
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Yunus Imren, Semih Dedeoglu, Sevgi Atar, Haluk Cabuk and Hakan Gurbuz. The first draft of the manuscript was written by Bulent Karslioglu and Serhat Gurbuz. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Each author certifies that his or her institution has approved the reporting of this report, that all investigations were conducted in conformity with ethical principles of research. Our study was approved by HSU Prof. Cemil Tascioglu City Hospital Ethical Committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.