
Abstract
Objectives:
To evaluate whether anthropometric data can predict anterior cruciate ligament (ACL) sizes on magneti resonance imaging (MRI) in Asian population.
Background:
Reconstruction of ACL has been performed over a decade ago. Recently, more individualized ACL reconstruction is performed taking account of each patient’s ACL characteristics. However, there has been limited study regarding ACL sizes in Asian Indonesian population. This study aimed to evaluate the role of anthropometric data in ACL sizes using MRI in Asian Indonesian population.
Study Design:
Retrospective Study.
Method:
A series of 531 knees from 420 patients with knee pain and intact ACL confirmed by MRI study. Length, width and inclination angle of ACL were measured using a T2-weighted sagittal MRI 3.0 Tesla Magnetom Skyra. Height, weight, body mass index (BMI) and age were recorded. Multiple regression analysis was used to determine relationship between the anthropometric data and size of ACL measurements.
Result:
ACL length and width were significantly different between male and female, consecutively. Mean ACL length was 35.36 ± 3.63 mm, male was significantly longer (36.59 ± 3.24 mm) compared to female (32.77 ± 2.99 mm), p < 0.0001. Mean ACL width was 10.23 ± 1.84 mm, male was significantly wider (10.85 ± 1.59 mm) compared to female (8.93 ± 1.64 mm), p < 0.0001. The mean ACL inclination angle was 47.75° ± 3.07° (range 40.17°–57.12°). The strongest correlation for ACL length was height and weight (r = 0.437; r = 0.341 consecutively, p < 0.0001). Females had stronger correlation compared to males for ACL length (R2 = 0.489 vs R2 = 0.418). ACL width showed weak correlation with anthropometric data. The following regression analysis equation was obtained for ACL length: ACL length = 60.697 − 0.11*age + 0.461*weight (kg) − 16.522*height (meter) − 1.093*BMI (R2 = 0.539; p < 0.0001).
Conclusion:
Anthropometric data can be utilized as a predictor of ACL length in Asian Indonesian population. The ACL length in Asian Indonesian population is shorter than that in Western population study.
Introduction
Individualized anterior cruciate ligament (ACL) has become a gold standard in recent ACL reconstruction. 1,2 Previously, single bundle ACL reconstruction has been the golden standard. 3 However, recent studies revealed degenerative changes in 95% of patients after single bundle ACL reconstruction with only 47% were able to return to previous level of activity 4 and persistent functional instability following single bundle ACL reconstruction. 5 A more stable knee during not only anterior-posterior translation but resistance to rotation is desired. A double bundle anatomic ACL reconstruction recently proved to be more suitable compared to a single bundle anatomic ACL reconstruction to serve this purpose. 5,6
Individualized anatomic ACL reconstruction requires an exact positioning of each graft passed in order to obtain an optimal functional outcome. 7 Incorrect placement of graft will result in early failure, limitation of range of motion, and residual instability. 8 Therefore correct positioning of graft in a double bundle ACL reconstruction and proper pre-operative surgical planning is paramount.
Performing double bundle ACL reconstruction in Asian patients has its own unique feature. Compared to western population, there has been higher percentage of patients with ACL tibia footprint <14 mm. 9 There are limited literatures measuring ACL sizes in Asian population especially Asian Indonesian population. Tan et al. revealed that ACL in Singaporean Chinese is smaller, narrower and more vertical than western population rendering the need to adjust graft selection and reconstruction intra-operative technique. 10 The purpose of this study is to measure ACL length and width in Asian population and to find its correlation with patient’s anthropometric data. We hypothesized that ACL correlates well with anthropometric data and hence in our population is shorter compared to Western population.
Method
We retrospectively evaluated a total of 531 knees from 420 patients complaining knee pain from January 2017 to July 2020. Intact ACL in physical examination and normal visualized MRI were included. The exclusion criteria of this study were abnormal ACL (partial or complete tear), history of knee infection, rheumatoid arthritis or fracture on the knee joint area. Height and weight were measured in the hospital on the day MRI was performed. Informed consent was obtained from all patients and this study was approved by the ethical committee KE/FK/1203/EC/2020.
Measurement of ACL length and width
All MRI were obtained with the knee in full extension. The ACL length, width and inclination angle were measured using high definition Siemens Magnetom Skyra MRI machine 3.0 Tesla. The images were then imported to Carestream Vue Motion (Carestream Health Inc, Rochester, NY) for analysis. The following protocols were used: proton density-weighted sagittal image (thickness, 1.5 mm; 256 × 256 matrix, field of view, 16 × 16 cm; time of repetition, 1300 milliseconds; time to echo, 15–17 milliseconds), T2-weighted sagittal images (thickness, 1.5 mm; 256 × 256 matrix, field of view, 16 × 16 cm; time of repetition, 4000 milliseconds; time to echo, 100–110 milliseconds), and oblique coronal proton density-weighted images (thickness, 1.5 mm; 256 × 256 matrix, field of view, 16 × 16 cm; time of repetition, 1300 milliseconds; time to echo, 15–17 milliseconds).
Measurements were performed twice by two different orthopedic surgeons and the mean value were recorded. ACL width was measured using an oblique coronal slice best showing the ACL fiber tibial attachment. A line was drawn above subchondral bone as close to the bone as possible between the most medial and most lateral portions of ACL fiber tibial attachment. The length of the line was measured as the width of the ACL at the tibial insertion. (Figure 1(a)). 11 In order to measure ACL length, proton density sagittal view was used and the clearest cut showing both tibial and femoral insertion sites was chosen. ACL length was measured as the distance between mid-portion of the insertion sites (Figure 1(b)). 12
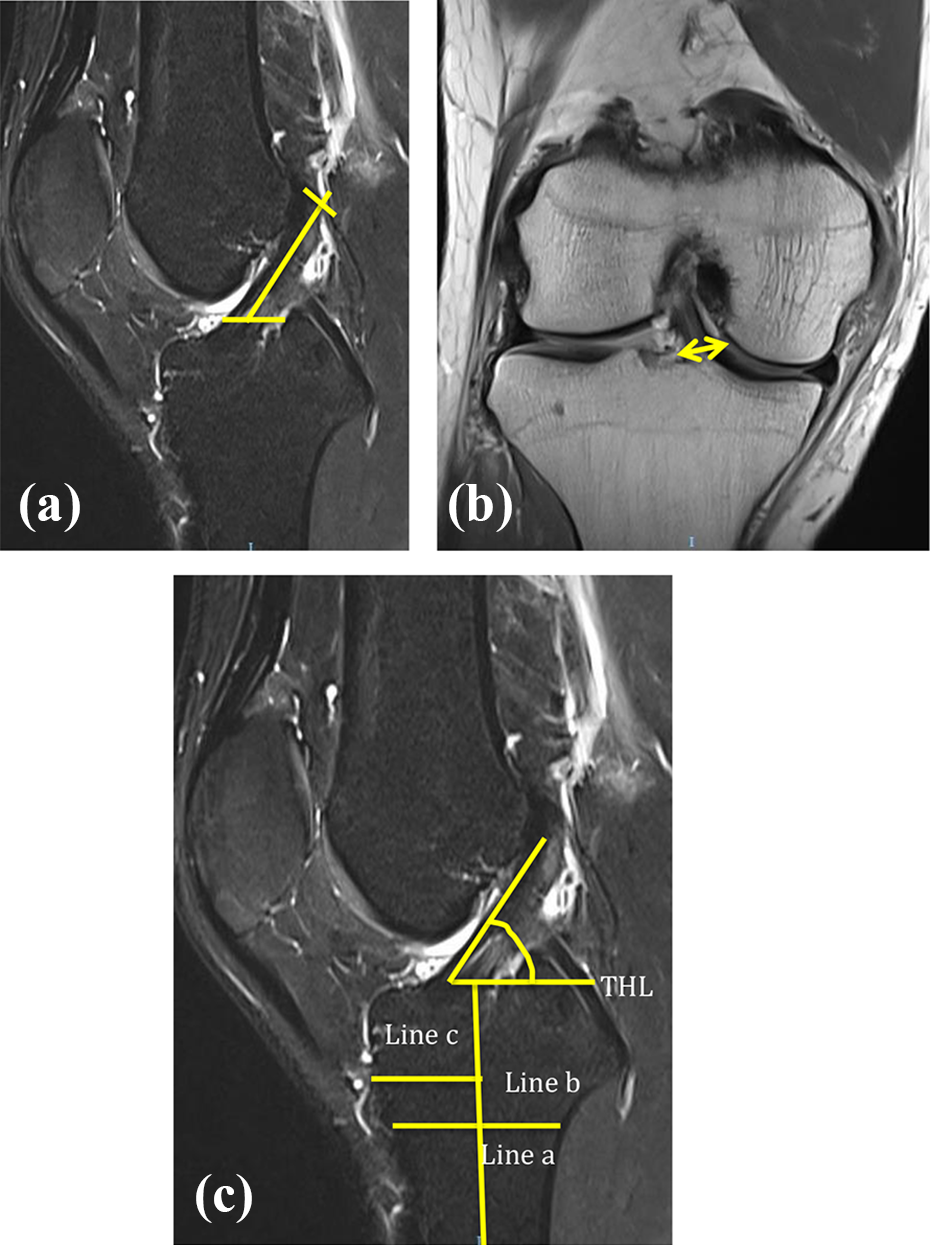
(a) Femoral and tibia insertion site is highlighted, the distance between mid-portion of tibia and femoral insertion sites are measured as ACL length. (b) ACL width on tibia insertion. (c) Line a drawn over the physeal scar, half of the line a, and line b is taken half of distance from the most distal width. The midpoints of these lines are connected coursing the long axis of tibia (line c). A line perpendicular to line c is the tibial horizontal line (THL). Inclination angle is formed by THL and the most anterior fiber of ACL.
Measurement of ACL inclination angle
The ACL inclination angle was measured by method described by Illingworth et al. 13 Sagittal proton density-weighted image cut was selected to measure ACL inclination angle. The long axis of tibia is estimated by selecting its most distal portion available in the image. The width of the diaphysis (line a) parallel to the physeal scar is then measured. Proximally in the diaphysis, another width measurement (line b) is taken half of the distance from the most distal width. The midpoints of these lines are connected coursing the long axis of the tibia (line c) and a line perpendicular to the line c, named the tibial horizontal line (THL), is drawn. A parallel line to the THL is created and its end placed at the most anterior portion of the ACL. The angle between this line and the most anterior fibers of ACL is the ACL inclination angle (Figure 1(c)). 12
Statistical analysis
All data were collected and analyzed using SPSS software version 23. Descriptive statistics were calculated for all variables. Independent T-Test was used to compare the differences between gender and ACL length, width and inclination angle. All significance level was set at P < 0.05. Pearson rank correlation coefficient was calculated to evaluate the association between the size of ACL length, width and patient’s weight, height and BMI. The strength of the correlation was indicated by the coefficient −1 to +1. When the relationship of one variable decreases while the other increases the coefficient is negative but greater than −1; when both variable increases the coefficient is positive but less than +1; and when a relationship is random or non-existent, the coefficients are nearly zero. Simple linear regression was used to estimate the association between patients’ height and weight with ACL width and length. Multiple linear regression equations were used to predict the size of ACL length and width based on patients’ height. Descriptive statistics was used to describe ACL inclination angle. Intra- and inter-observer reliability of the ACL length and width size on MRI was analyzed with an intra-class correlation coefficient (ICC). The strength of agreement can range from 0 to 1 (≥0.80, good; 0.60–0.79, moderate; ≤0.59, poor).
Results
From 531 knees, 360 were males and 171 were females with an average age of 31.64 (range 18–40 years old). Mean height was 168 ± 8.3 cm (range 150–181 cm), weight was 75.37 ± 17.25 (range 49.45–132.20 kg), and BMI was 26.54 (range 18.57–41.72). The mean ACL length was 35.36 ± 3.63 mm, with ACL length in male was significantly longer (36.59 ± 3.24 mm) compared to female (32.77 ± 2.99 mm), p < 0.0001. (Table 1) Mean ACL width was 10.23 ± 1.84 mm, and ACL width in male was significantly wider (10.85 ± 1.59 mm) compared to female (8.93 ± 1.64 mm), p < 0.0001 (Table 2). Females had stronger correlation compared to males for ACL length (R2 = 0.489 vs R2 = 0.418) and width (R2 = 0.058 vs R2 = 0.041). The mean ACL inclination angle was 47.75° ± 3.07° (range 40.17°–57.12°). There was no significant difference between ACL inclination angle in male and female (P = 0.584).
Physical characteristics of the participants.

BMI: body mass index (kg/m2).
Data were given in mean ± standard deviation.
a P value: comparison of values between males and females.
ACL length, width, and inclination angle measurements in men and women.
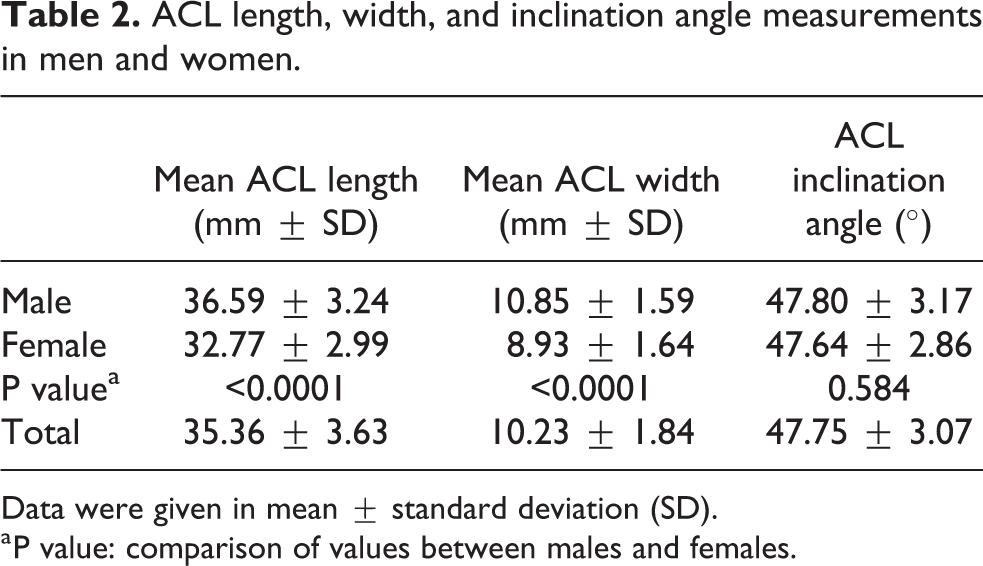
Data were given in mean ± standard deviation (SD).
a P value: comparison of values between males and females.
The strongest correlation for ACL length was patient’s height and weight (R = 0.662; R = 0.585 consecutively, p < 0.0001) (Table 3) while the strongest correlation for ACL width was patient’s height (R = 0.434, p < 0.0001) (Table 4). Females had stronger correlation compared to males.
Univariable analyses for ACL length. 1

a ACL: anterior cruciate ligament; BMI: body mass index; MRI: magnetic resonance image.
b Adjusted R2.
Univariable analyses for ACL width.

a ACL: anterior cruciate ligament; BMI: body mass index; MRI: magnetic resonance image.
b Adjusted R2.
The following regression analysis equation was obtained for ACL length:

The following regression analysis equation was obtained for ACL width:

Discussion
The most important finding of this study is that anthropometric data could reliably predict ACL length in Asian population. Graft-size mismatch is one of the most common complications in an ACL reconstruction. 14 Understanding the intra-articular length of ACL during pre-operative planning is pivotal especially when performing an individualized anatomical ACL reconstruction to prevent graft-tunnel mismatch. 15 Knowing and undersatanding patient’s anatomical ACL size before surgery would obviously aid in the pre-operative planning and graft selection.
Previous literatures have shown conflicting relationsfhip between anthropometric data and intra-articular ACL length. 16,17 Brown et al. showed a strong positive correlation between intra-articular length of ACL and patient’s height and the patient’s height could be used as a predictor for appropriate graft length in a BTB allograft ACL reconstruction. 16 However, Denti et al. did not find significant relationship between length of intra-articular ACL graft and patient height and weight in a 50 reconstructed and 9 cadaveric knees. 17 Different results might be due to the highly variable ACL in certain populations. To date, there have been no study evaluating relationships of ACL length and anthropometric data in Asian population.
Our study revealed a mean ACL length of 35.36 mm which was longer than a previous study in Chinese Singapore population 10 but shorter than ACL in Western population studies. 15,18,19 The mean ACL width in our population at the tibia insertion site was 10 mm which was approximately the same compared to Western population 15 but slightly wider than other studies 10,20 which might be due to the different measurement technique. We measured the ACL width at the tibia insertion site but Tan et al., 10 measured at the mid-substance, while Kupczik et al. at middle third of the intercondylar region. 20 Hence due to the fan-shaped ACL fiber our result at the tibia insertion site was wider. Like all other literatures, we found that gender also affect the size of ACL, male significantly had longer and wider ACL compared to female which was in concordance with other studies (Table 5). 10,15,18,19 This result if important during performing graft selection in ACL reconstruction taking account the shorter and more narrow characteristic of ACL in Asian population compared to western population and moreover in females.
Comparison between ACL measurements from literatures.

ACL: anterior cruciate ligament; NA: data not available.
Data were given in mean ± standard deviation (range).
Previous study also found strong correlation between patient’s height and graft length, 16 therefore during graft selection, autograft is more favorable while allograft from Western population or larger diameter synthetic graft is not recommended. During ACLR, an “all-inside” technique which requires the graft to be quadrupled, and screw fixation in the femoral tunnel is not recommended with a more narrow native ACL
Anatomical graft placement may lead to a better functional outcome after an ACL reconstruction. Illingworth et al. 13 quoted a value of more than 55° was considered as a non-anatomic placement of femoral tunnel. Similar with studies from Illingworth et al. 13 (43°–57°) and Kupczik et al. 20 (43°–57°), we found an inclination angle ranged between 40° and 57° with no significant differences between gender. Our result was different from a study in ACL anthropometry by Tan et al. 10 in Singaporean Chinese population showing a more vertical ACL orientation. This might be due to the different technique used to measure the inclination angle. We used the same technique by Illingworth et al. 13 This result is an important information so that we should prevent placing ACL graft in a more vertical fashion in Asian population.
Limitation of study
This study has its certain limitation. Although rigorous inclusion and exclusion criteria have been applied to minimize errors, compromised ACL cannot be entirely excluded. Second, although this is the first study measuring ACL sizes in Indonesian population, an in-vivo (cadaveric) study might be needed to compare the ACL size from MRI and the true size. Finally, a future study with larger size and multi-centered sample will enhance the significance of this study.
Conclusion
Anthropometric data can be utilized as a predictor of ACL length in Asian population. The ACL length in Asian population is shorter than that in Western population study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.