
Abstract
Purpose:
This study aimed to present the change in humeral retroversion (HR) angle (HRA) that occurs in childhood and young adulthood and the potential developmental difference that is observed in wrestlers.
Methods:
HRA of dominant and non-dominant shoulders (DSHRA and NDSHRA, respectively) were measured using ultrasonography in a group of 30 wrestlers who started wrestling before the age of 13 years (Group 1), a group of 30 young adults, aged between 16–20 years, who were not actively engaged in any branch of overhead sports (Group 2) and a group of children aged between 11–13 years and not actively engaged in any branch of overhead sports (Group 3). Range of motion (ROM) degrees of dominant and non-dominant shoulders in all groups were compared within each group and between the groups.
Results:
DSHRA (mean: 88.73°, 88.93° and 89.40°) values were significantly higher than NDSHRA (mean: 81.13°, 81.83° and 84.37°) values (p < 0.001, p < 0.001 and p < 0,05) in Groups I, II and III, respectively. Internal rotation and total ROM degrees of the dominant shoulder in Group 1 and 3 were higher than those in Group 2.
Conclusion:
There is no significant change in terms of HRA in people aged between 11–13 and 16–20 years because of natural development or wrestling. DSHRA values are higher than NDSHRA ones. In contrast to the shoulders of throwers, the shoulders of wrestlers are characterized by an increase in internal rotation, described as “Wrestler’s shoulder.”
Level of Evidence:
Level III.
Introduction
Humeral retroversion (HR) development has been reported in cadaver studies, to date. A cadaver study by Edelson in 2000 reported that HR angle (HRA) is approximately 65° between the ages 4 months–4 years, a large change between the ages 4–11 years, later the value continues to decrease and the last state of change is observed around the ages 16–19 years. 1 And mostly accepted degree interval is between 25º to 35º in adults. 2
The decreasing speed of change in HRA is caused by the bone and soft tissue adaptation in people engaged in overhead sports and the shoulder injuries observed in athletes involved in overhead sports are a popular subject in recent studies. 3 –5 The frequency of use of computed tomography, recognized as the gold standard for evaluating HRA, is gradually decreasing following the study that reported ultrasound (US) to be sufficient for the evaluation. 6 –11
Wrestling is one of the ancient and original Olympic sports and shoulder is the most commonly injured joint of the wrestlers. 12,13 The wrestlers trains to develop their shoulder structures because they are required to have an increased range of motion (ROM) in their shoulders. They need to have a dynamic and strong internal rotation (IR) motion to defend the wrestling movements (Figures 1 and 2).

A wrestler’s shoulder rotation training with a weight of 5 kg.
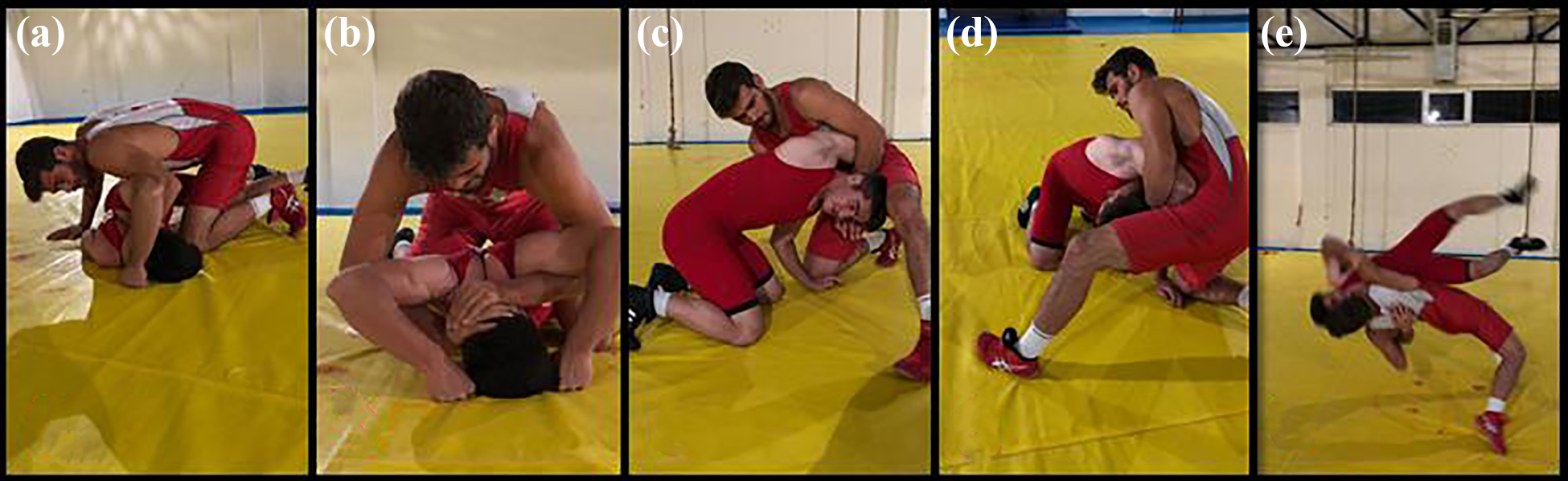
Photos from a wrestling competition: (a) Half Nelson movement, (b) Full Nelson movement, (c) shoulder being forced for an external rotation, (d) another view of the (c) figure, and (e) suplex movement.
Increased HRA is thought to be both the reason and protective mechanism for shoulder injuries in baseball players. 3,4,10 In the light of this information we hypothesized that athletes engaged in wrestling who most commonly injuries their shoulder have increased shoulder ROM and increased HRA would be one of the reason for this.
The present study aimed to compare the HRA values and ROM of wrestlers with a group of people not engaged in overhead sports aged between 16–20 years and another group of individuals not engaged in overhead sports aged between 11–13 years and thus known to have completed their HR development to a greater extent. 10
Materials and methods
The study was accepted by the local ethics committee (decision numbered 371 on 24th of April, 2019). Informed consent was provided from all participants or both from participants and their families if they are under the age of 18.
Measurements
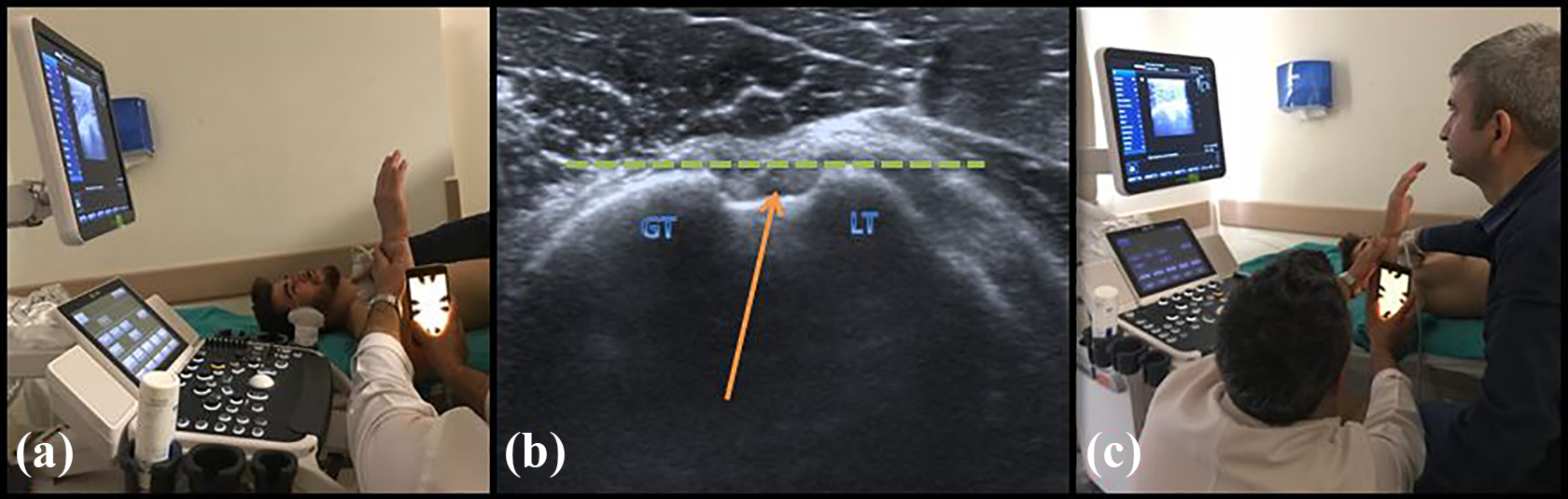
Assessment of the humeral retroversion angle. (a) Trying to parallel the US probe to the ground. (b) GT: Greater tubercle, LT: Lesser tubercle. Arrow shows the bicipital groove and the bicipital tendon. GT-LT parallel to the horizontal line. (c) Another view of the procedure.

Assessment of the glenohumeral internal rotation degree.
For the inter-group evaluation, ANOVA was used to analyze the results suitable for the normal distribution. In cases where there was no normal distribution Kruskal–Wallis test was used for analysis, and pairwise comparison was conducted for significant results. T-test was used to compare the differences between the intra-group measurements of dominant and non-dominant shoulders. All statistical analyses were conducted using SPSS Statistics 19.0 (SPSS Inc, an IBM Company, Chicago, Illinois).
In addition to the participants in whom the measurements were conducted, 60 shoulders of 30 individuals with different ages were measured twice at 1-week intervals, and their HRA, External rotation (ER) and IR angles were recorded on the dominant and non-dominant sides to evaluate intraobserver reliability.
Results
All of the participants were male. The mean age of the participants was 15.52 years (range; 11 to 24 years, Standard Deviation [SD] = 3,1).
Group 1 comprised wrestlers that were engaged in wrestling for at least 2 years, and 5,73 years on an average and the mean age was 16.53 years (range; 13 to 24 years, SD = 3.1374) (Table 1). The minimum and maximum ages for starting wrestling were 7 and 13 years, respectively. The mean age for starting wrestling was 10.8 years. Among these, 6 and 24 had their left and right hands as dominant, respectively, 8 were qualified as national team wrestlers and the rest 22 were only athletes of sports clubs.
Age, DSHRA, NDSHRA values of each groups.

In Group 2, mean age of the participants was 17.93 years (range; 16 to 20 years, SD = 1.2015) and 4 and 24 had their left and right hands as dominant hands, respectively. In Group 3, mean age of the participants was 12.1 years (range; 11 to 13 years, SD = 0,8030) 4 and 26 had their left and right hands as dominant, respectively.
Mean Non-Dominant Shoulder HRA (NDSHRA) values for Groups 1, 2 and 3 were 81.13°, 81.83° ve 84.37°, respectively (Table 1). No significant difference was observed between the NDSHRA values of the three groups.
In all participants, DSHRA values (89.0222 on average) were higher than their NDSHRA values (82.4444 on average; p < 0,001) (Table 1).
External rotation motion
Rotation degrees of all groups.

Statistical comparison of rotation degrees between each group.

Internal rotation motion

Distribution of DSIR degrees according to groups.

Distribution of DSTROM degrees according to groups.
Distribution of weight, height and BMI for each groups.

Intraclass correlation coefficient (ICC) for DSER was 0.979 (ICC using an absolute agreement definition of 97.9%), and ICCs were 0.948, 0.952, 0.946, 0.965 and 0.967 for NDSER, DSIR, NDSIR, DSHRA and NDSHRA, respectively.
Discussion
In the study published by Edelson in 1999, reported that right HRA is significantly higher than the left one, which is associated with being the dominant shoulder. In addition, Edelson also reported that HRA is significantly higher in male cadavers than in female ones. 2 The mean HRA of Turkish people, measured by Öztuna et al. and they reported no significant difference between dominant and non-dominant sides. 5 In the present study, HRA was not conventionally measured but using a US-assisted HR measurement technique that has been proven to be valid in previous studies. 6,10 The present study reports that HRA increases in favor of dominant shoulder when dominant and non-dominant shoulders are compared. And there is a significant difference for all groups as reported in the cadaver study conducted by Edelson 2 (Table 1).
Increased HRA is reported as one of the adaptive changes that occur in thrower’s shoulder and this change is observed as an over-increase that occurs as a result of the decrease in HRA’s decrease speed caused by aging, rather than an increase. 14 This increase in retroversion is accompanied by increase in posterior capsule thickness. 15 There are studies that compare shoulder HRA in throwers’ shoulders and athletes not engaged in overhead sports or normal individuals. This comparison has been recently based on whether the dominant side is right or left and on the effects of the age of starting playing baseball for the HRA of those engaged in baseball. It’s reported that increased HRA might be both reason and a protective mechanism for a possible shoulder injury. 3,4,10,16 –19 The present study includes both ROM comparison between dominant and non-dominant sides in all the groups and a comparison of HRA. It also deals with whether there is a correlation between HRA and the age of starting wrestling or the number of years spent engaged in wrestling professionally to find the reason of increased shoulder injuries in wrestlers. In Group 1, there was no correlation between DSHRA and the age of starting wrestling or the number of years spent engaged in wrestling. Similarly, there was no correlation between the age of starting wrestling and shoulder joint motion angle. The external rotation and HRA values of the dominant shoulders were significantly higher than the ones in non-dominant shoulders in all groups. These results are similar with the ones reported in the study by Nakase et al. as detected in those who are not throwers. 17 As for HRA and ER values, they are similar to the literature in terms of higher values in dominant sides. 16,18
Age of 11 years is considered as the critical starting age for playing baseball because of the development of the proximal humerus and HRA is different in the ones starting playing baseball before 11 years old and in the ones starting baseball after 11 years old. 10 One of the reasons is the change that occurs in the proximal physis line in time. In 1991, Pritchett 20 reported that the growth that occurs on proximal physis after the age of 11 years in 90% of cases; and in 2000, Edelson 1 reported that the change in HR is almost completed by the age of 16 years and might continue by the age of 19 years. In the present study, Group 1 included participants that are at minimum age of 13 years and have been doing wrestling professionally for at least 2 years; Group 2 comprised participants between the ages 16–20 years; and Group 3 comprised participants between the ages 11–13 years; therefore, these age ranges have been selected by paying attention to this varying process of epiphyseal development and HR. The reason why these age ranges were selected is to minimize the effects of the changes that occur during the normal development process and to maximize the reliability of the results.
Wrestling is one of the old Olympic sports branches and requires discipline during the phase of physical preparation. 21 As shoulder is the most injured part of wrestlers’ body those with ligamentous laxity has lower risk of a shoulder injury. 12,13 In the study by Bigliani et al. 22 in 1997 on shoulder ROM of baseball players, the average shoulder ROM values in dominant shoulders measured with shoulders in 90° abduction were higher than that in the present study. However, the contrary applies to the non-dominant shoulders. Much lower IR values were reported for dominant and non-dominant shoulders compared to the values presented in the current study. 22 Glenohumeral Internal Rotation Deficiency (GIRD), which is reported as the change that occurs on the posterior capsule due to recurring microtraumas, is reported to be of significance in ethological terms. 23 Excluding IR values, the evaluation of the shoulder motions in all the groups reveals that Group 3 has the highest values in terms of all the ranges of motion. However, as for the shoulder joint IR values, contrary to the GIRD described in the literature for thrower’s shoulder, wrestlers have significantly higher IR values both on dominant and non-dominant sides than other groups. When compared with the group of participants aged 11–13 years, the changes in IR values can be explained based on previous studies. 24,25 However, the reason why it has increased compared to a similar age group is the differences that wrestlers’ shoulders have. This situation and the statistical differences are the answers to the “does the wrestler’s shoulder have any difference in its bone or soft tissues in terms of shoulder development compared to the normal population?” question.
According to the present study, the reason why DSIR, NDSIR and DSTROM, NDSTROM values were significantly higher in the group of wrestlers than in the same age group is that wrestlers, contrary to other overhead sports branches (volleyball, handball, baseball, swimming, etc.), are exposed to continuous external rotation exerted by their opponents in the competition; therefore, they exert excessive effort for IR, which they do intensively. We believe that the term “
Number of the participants, the range of the age differences, engaging time with wrestling and excluding the wrestlers who had shoulder injury are some of the limitations of our study. The new studies with more participants with the minimum standard deviations of the age and wrestlers engaged with wrestling more years with starting earlier age would be more powerful.
Conclusion
There is no significant change in terms of HRA in people aged between 11–13 and 16–20 years because of natural development or wrestling. In Turkish population, DSHRA values are higher than NDSHRA ones. In contrast to the shoulders of throwers, the shoulders of wrestlers are characterized by an increase in internal rotation, described as “Wrestler’s shoulder.”
Footnotes
Acknowledgment
Haluk Özcanlı: Thanks for the giving some new ideas about the method. Ali Cavit: Thanks for giving some new ideas about the procedures used in method and discussing about the wrestler’s shoulder. Salih Şentürk: Head coach of the wrestlers. Co-operation with the wrestlers and the families.
Author contributions
Conception or design of the work: OC, AMÖ. Applied procedures: OC, AE. Analysis or interpretation of data: OC, AC, AE, AMÖ. Revised the manuscript critically for important intellectual content: OC, AC, AMÖ.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was granted by the Institutional Review Board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Provided from each participant or from their families.