
Abstract
Purpose:
This study aimed to use MRI to evaluate the fibula and talus position difference in functional and mechanical ankle stability patients.
Methods:
61 and 68 patients with functional and mechanical instability, and 60 healthy volunteers were involved. Based on the axial MRI images, the rotation of the talus was identified through the Malleolar Talus Index (MTI). The position relative to the talus (Axial Malleolar Index, AMI) and medial malleolus (Intermalleolar Index, IMI) were used to evaluated the displacement of the fibula.
Results:
Post hoc analysis showed that the values of malleolar talus index was significantly larger among mechanical instability (89.18° ± 2.31°) than that in functional instability patients (86.55° ±61.65°, P < 0.001) and healthy volunteers (85.59° ± 2.42°, P < 0.001). The axial malleolar index of the mechanical instability patients (11.39° ± 1.41°) were significantly larger than healthy volunteers (7.91° ± 0.83°) (P < 0.0001). There were no statistically significant differences in the above three indexes between the functional instability patients and healthy volunteers.
Conclusion:
The functional instability patients didn’t have a posteriorly positioned fibula and an internally rotated talus. The malleolar talus index was significantly larger among mechanical instability patients than that in functional instability patients. Increased malleolar talus index may become a new indirect MRI sign for identifying functional and mechanical instability patients.
Introduction
Acute ankle sprains are the most common injuries sustained during sports activities. 1 More than 20% of these patients undergo chronic symptoms, including ankle swelling, pain, and sense of instability or giving away. 2,3 Chronic ankle instability (CAI) is one of the results after one or more ankle sprain, and it can be subdivided into functional ankle instability (FAI) and mechanical ankle instability (MAI). 4,5 The lateral ankle ligaments in FAI patients are normal. 6 And the sense of instability may be resulted by specific impairments in neuromuscular control, proprioception, postural control, and/or muscle strength. 7,8 On the contrary, physical and radiological examination could find that the MAI patients have obvious lateral ligaments laxity and excessive ankle range of motion. 9
In clinical practice, it is very important for surgeons to accurately identify the type of ankle instability for providing corresponding treatment strategies, since the treatments for FAI and MAI are quietly different. MRI is an important tool in assessing the status of the lateral ankle ligaments. However, the published sensitivity and specificity of MRI in directly diagnosing chronic anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) injures are 44–75% and 53–86%, respectively. 10,11 Therefore, it is necessary to explore indirect MRI signs to better identify FAI and MAI.
Previous studies have demonstrated that the anatomical variations were associated with CAI. 12,13 Eren et al. and Scranton et al. adopted the axial malleolar index (AMI) as a means of evaluation and suggested that the patients with ankle sprain or MAI were more likely to have a posteriorly positioned fibula. 14,15 However, recent studies demonstrated that the AMI was inaccurate, and suggested that the patients with MAI had no significant posteriorly positioned fibula. And MAI patients were more likely to have an internally rotated talus, which would result in misleading AMI value. 16,17 In addition, all the previous studies did not include the FAI patients, what has changed in the ankle joint of FAI patients remains unknown
This study aimed to compare the anatomical variations with MRI axial tomographic in patients with MAI, FAI and the healthy participants, and to introduce an indirect MRI sign to identify the patients with FAI and MAI. We hypothesized that the patients with FAI did not show an internally rotated talus like the patients with MAI.
Materials and methods
The present study retrospectively reviewed MRI scans taken from January 2013 to December 2018 of 61 patients (31 female and 30 male) with FAI and 68 patients (22 female and 46 male) with MAI in our center. Arthroscopic ankle evaluation and debridement were performed in all CAI patients. ATFL tears were identified during ankle arthroscopy. Clinical evaluations were made on the basis of history, physical examination, and radiographic findings (anteroposterior, lateral, and MRI). Only those who did not suffer from ankle lateral ligament tears were diagnosed as FAI patients. All operations were performed by a senior surgeon specializing in ankle arthroscopy and foot and ankle surgery.
Patients would be included as MAI under the following conditions: (1) A history of the previously injured ankle joint “giving away,” and/or recurrent sprain and/or “feeling of instability”; (2) Associated with inflammatory symptoms (pain, swelling, etc.); (3) Positive physical examination of anterior drawer test (ADT); (4) Identified with lateral ligament injuries using MRI, B-ultrasound and ankle arthroscopy); (5): Cumberland Ankle Instability Tool (CAIT) score <24. 18 Patients would be included as FAI under the following conditions: (1): A history of the previously injured ankle joint “giving away,” and/or recurrent sprain and/or “feeling of instability”; (2) Associated with inflammatory symptoms (pain, swelling, etc); (3) Negative physical examination of ADT; (4) Identified with no obvious lateral ligament injuries using MRI, B-ultrasound and ankle arthroscopy; (5): Identification of functional ankle instability (idFAI) score >11. 19
The control group consisted of 60 healthy volunteers (32 female and 28 male) who had undergone MRI scan in our center. The exclusion criteria were as follows: (1) A history of previous fracture, ankle sprains, ligamentous laxity in either lower extremity requiring realignment; (2) A history of previous surgeries to the musculoskeletal structures in either lower extremity; (3) Deformity of foot and ankle, such as high arch, varus heel, flat foot; (4) Patients with PTFL injury and/or deltoid ligament injury; (5) Age less than 16 or older than 60 years; (6) Acute or previous soft tissue and tendon injury around the ankle, such as old Achilles tendon rupture, posterior tibial tendon injury.
MRI scan and image analysis
All of the MRI computer axial tomographic (CAT) scans were performed with a 3.0-T MRI scanner (MAGNETOM Verio, A Tim system, Siemens, Germany) in a standardized fashion. Axial images were taken at PD FSE TR/TE 2600–2800/24–30 ms, matrix 512 × 320, slick thickness 3 mm. Axial images were obtained from the distal tibial diaphysis to the inferior aspect of the calcaneus with hips and knees extended and both feet resting against a footplate. 20 All the measurements were performed in the level where fibula, talus and medial malleolus were most clearly shown.
The axial malleolar index (AMI), which was first described by Scranton et al., 15 was calculated in the following manner (Figure 1): the plane of the talus was determiner, and a line (A) was drawn that bisected the talus axis. A second line (B) was drawn, running perpendicular to the talar axis from the anterior border of the medial malleolus laterally. A third line (X) was drawn from the intersection of line (A) and (B), running to the anterior border of the fibula. The angle between B and X represented the AMI. For the accuracy of AMI values, the alignment of the talus and position of the fibula were required in this measurement. A positive value indicates the lateral malleolus was posterior to the plane of the medial malleolus. A negative value indicates the lateral malleolus was actually anterior to the plane of the medial malleolus.

MRI axial tomographic illustration of the left ankle demonstrating the AMI as originally described. The angle between line B and X represented the AMI.
The IMI was measured in the following manner (Figure 2): the plane of the articular surface of the talus was determined, and a line (A) was drawn that paralleled the articular border of the medial malleolus. A second line (B) was drawn perpendicular to line (A) from the anterior border of the medial malleolus. A third line (X) was drawn from the intersection of line (A) and (B) to the anterior border of the fibula. The IMI was the angle formed between line (B) and (X). Since the measurement of IMI was only based on the medial malleolus, the rotation of the talus was not taken into account in this measurement. A positive value indicates the lateral malleolus was posterior to the plane of the medial malleolus. A negative value indicates the lateral malleolus was actually anterior to the plane of the medial malleolus.

MRI axial tomographic illustration of the left ankle demonstrating the IMI as described in text, which referenced from the medial malleolus. The angle between line B and X represented the IMI.
The malleolar talus index (MTI) was described calculated in the following manner (Figure 3): the plane of the articular surface of the talus was determined, and a line (A) was drawn that bisected the talus axis. A second line (B) was drawn, running perpendicular to the talus axis from the anterior border of the medial malleolus. A third line (X) was drawn parallel to the articular border of the medial malleolus. And the position of the fibula did not need to be measured. The MTI was the angle formed between line (B) and (X). The increasing MTI value indicated the internal rotation of the talus. In order to make the ankle joint in a fixed position and reduce the error, an ankle fixation and positioning device were designed and used during the MRI scanning. Therefore, every ankle of participant was scanned under a same position.

MRI axial tomographic illustration of the left ankle demonstrating the MTI as described in text, which indicated the degree of internal rotation of the talus. The angle between line B and X represented the MTI.
The line and angle measurement were performed with a picture archiving and communication system (PACS version 11.0, Carestream Healthcare, Rochester, NY, USA). An independent observer, who was blinded to the group assignments, measured all the values on the MRI scans. Each measurement was repeated 3 times for intra-observer analysis, as well as calculating of mean values. For the purpose of eliminating any effects of memory, the interval between each measurement is at least 1 week. As a test of interobserver, all the participants’ values in each ankle instability group and control group were measured independently by 2 of the authors (the first and the second authors).
Statistical analysis
All values were reported as means and standard deviations (SD). After checking of normal distribution of the variables by Kolmogorov-Smirnov test, the comparison of control and two ankle instability groups was performed with the use of a one-way ANOVA and Post Hoc Multiple Comparisons. Receiver operating characteristic curves (ROC) were used to analyze the MTI of participants with FAI versus MAI. The sensitivity and specificity of this method for identifying FAI and MAI were calculated. All statistical analyses were performed with SPSS 21.0 (IBM Corporation, Armonk, New York, USA). Intra- and interobserver reliabilities of measurements were analyzed with the intraclass correlation coefficient (ICC). An ICC <0.4 was considered poor; between 0.4 and 0.7, moderate; and >0.7, excellent. A reliability analysis of scale was used to calculate the ICC values. All statistical analyses were performed with SPSS 21.0 (IBM Corporation, Armonk, New York, USA). Significance was set at P = 0.05.
Results
No significant differences were found in age, sex, height, weight or BMI between the groups. Participants’ demographic data is shown in Table 1. And the inter- and intra-observer reliabilities are shown in Table 2.
Participants’ demographic data.

BMI: Body Mass Index; FAI: Functional Ankle Instability; MAI: Mechanical Ankle Instability.
Intra- and interobserver reliabilities.

ICC: Intraclass Correlation Coefficient; AMI: Axial Malleolar Index; IMI: Intermalleolar Index; MTI: Malleolar Talus Index.
The average AMI of the FAI patients was 8.68 ± 2.09° (range, 3.51–19.17°). The average AMI of the MAI patients was 11.39 ± 1.41° (range, 7.77–17.49°). The average AMI of in the control group was 7.91 ± 0.83°(range, 5.14–10.45°). There was statistically significant difference in the AMI between the FAI, MAI and control group (F = 54.80, P < 0.001). No statistically significant difference was shown in the AMI between the FAI and control group (P = 0.183). There was a statistically significant difference between the MAI and FAI (P < 0.001)
The average IMI of FAI patients was 9.74 ± 1.41° (range, 5.26–13.80°). The average IMI of MAI patients was 9.79 ± 1.50°(range, 4.67–15.52°). The average IMI of control group was 9.36 ± 0.92°(range, 5.45–11.07°). The one-way AVONA showed no statistically significant difference in the IMI between the FAI, MAI and control group (F = 0.86, P = 0.427). Both the FAI and MAI patients have no statistically significant difference with the control group respectively (P = 0.780; P = 0.627). And there was no statistically significant difference between the MAI and FAI (P = 1.000)
The average MTI of FAI patients was 86.55 ± 1.65° (range, 79.40–91.78°). The average MTI of MAI patients was 89.18 ± 2.31° (range, 80.19–94.30°). The average MTI of control group was 85.59 ± 2.42° (range, 81.12–94.84°). The one-way AVONA showed statistically significant difference in the MTI between the FAI, MAI and control group (F = 34.58, P < 0.001). No statistically significant difference was shown in the MTI between the FAI and control group (P = 0.189).
It was important that the patients with MAI had a significantly larger MTI value than that in patients with FAI (P < 0.001). The results of one-way ANOVA and Post Hoc Multiple Comparisons were shown in Table 3.
Results of one-way ANOVA and post hoc multiple comparisons.a
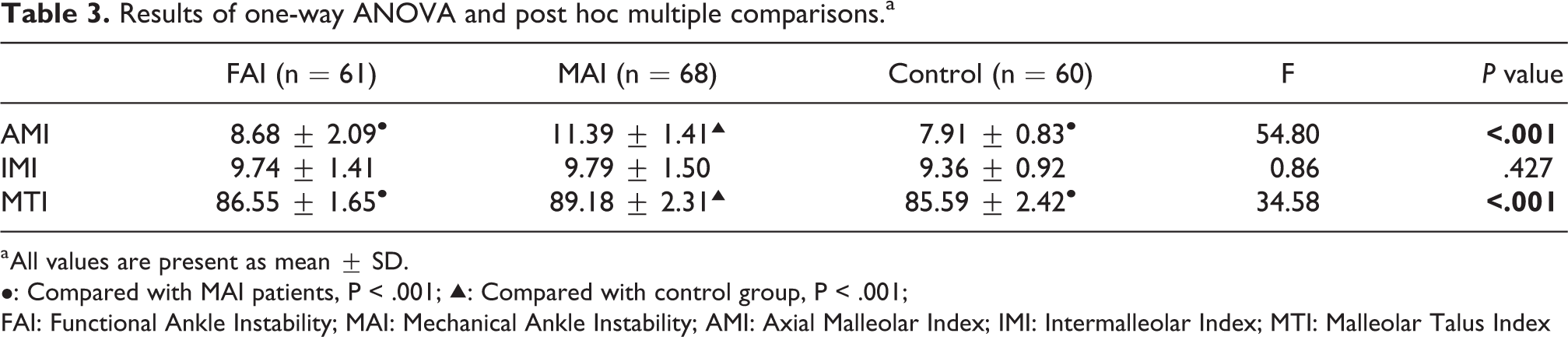
a All values are present as mean ± SD.
•: Compared with MAI patients, P < .001; ▴: Compared with control group, P < .001;
FAI: Functional Ankle Instability; MAI: Mechanical Ankle Instability; AMI: Axial Malleolar Index; IMI: Intermalleolar Index; MTI: Malleolar Talus Index
Discussion
In the current study, we again confirmed that there was no posteriorly positioned fibula in patients with MAI, and the MAI patients were more likely to have an internally rotated talus. In addition, the present study first reported that the patients with FAI were significantly different from the MAI patients in ankle anatomical variation. And it has shown that the patients with FAI have neither internally rotated talus, nor do they have posteriorly positioned fibula. These findings indicated that the rotating position of talus as an indirect MRI sign could be used to identify the patients with FAI and MAI.
Lateral ankle sprains are among the most common injuries, it would result in CAI after one or more sprains. 21,22 Most of the CAI patients would complain about chronic symptoms, including ankle swelling, pain, and sense of instability or giving away. The diagnosis of CAI is based on clinical (history, symptoms, physical examinations) and radiologic (X ray, MRI, B-ultrasound) findings. CAI could be subdivided into FAI and MAI, according to the different symptoms and pathological changes. 6,23,24 Previous studies indicated that the patients with MAI have anatomical variation, especially the position of fibula and talus. 25 –27 However, researches on ankle anatomical variation in patients with FAI has rarely been done so far.
Although the ankle joint consisted of many complex ligaments, tendons and musculoskeletal tissue, the published studies mainly focused on analyzing the anatomical variation of lateral malleolus and talus. Previous biomechanical studies performed on cadaver specimens have found the phenomenon of internally rotated talus. Fujii et al. and Hollis et al. found that there was a significant increase in the internal rotation motion at the tibiotalar joint upon sectioning the ATFL, suggested that isolated ATFL injury was associated with internal rotation torque in cadaveric specimens. 25,26 And only few in vivo studies assessed the position of fibula and the rotational change of the talus in MAI or CAI patients. The position of the fibula in the patients with CAI was controversial. Hubbard et al. and Kavanagh et al. found that the subjects with ankle sprains have an anterior movement of fibula. 27,28 However, they only used fluoroscopy to recorded the fibular position. It is not standard to calculate the position only with 2 dimensional lateral images due to the potential ankle rotation. Moreover, only 30 patients with CAI and 6 patients with acute ankle sprain respectively in these 2 studies were involved. The relatively less sample size may result in bias to their studies.
Eren et al., Scranton et al., McDermott and Jv, and Berkowitz and Kim reported that the fibula was positioned posteriorly in the patients with CAI. 14,15,30,31 They used MRI or CT axial scan images to evaluated that fibular position relative to talus through AMI value. But Lebrun and Krause thought it was the potential internally rotated talus that may lead to the posteriorly positioned fibula. 17 Therefore, they proposed the IMI to evaluated the fibular position relative to the medial malleolus. They found that there was no statistically significant difference in the mean IMI value of CAI patients between the two groups (10.4 ± 3.5° vs. 9.4 ± 3.4°, P > 0.05), while there was a significant difference between the CAI patients and control group when using the AMI to assess the position of fibula (16.8° ± 6.3 vs. 11.36 ± 7.3°, P < 0.01). They concluded that the fibular position was still normal in the patients with CAI. However, they only analyzed the CAI patients in a general way, they did not subdivide the subjects into FAI patients and MAI patients. Calculating the parameters of two different ankle instability patients together may have a certainly misleading influence on the conclusion. Whether the interaction between FAI and MAI patients affects the results of the study was not known. Meanwhile, the hypothesis that the CAI patients had more internally rotated talus was also confirmed by Li et al. 16 They proposed the MTI to evaluated the degree of internally rotated talus, and found that the mean MTI value of MAI patients was significantly greater than the control group (89.63 ± 3.77° vs. 85.78 ± 4.40°, P < 0.01), which indicated that the MAI patients were more likely to have an internally rotated talus. They only analyzed the anatomical changes in MAI patients. Therefore, we still don’t know what the position of fibula and talus changed in the patients with FAI, and what the similarities and differences with MAI patients are. Moreover, the participants in the control group of previous studies could not be representative a normal healthy population.
We mainly adopted AMI, IMI and MTI to evaluate the position changes of fibula and talus in the patients with FAI and MAI. An advantage of the study was that 60 normal healthy volunteers instead of the patients for reasons unrelated to ankle sprain or instability were involved as control group. We believe that the ankle joint as the most matched joint in the whole body, the geometric changes will have a significant impact on the coupling activities of the ankle joint, and even lead to early pathological changes. Therefore, the anatomical faults or variations could be regarded as a risk factor in the development of both FAI and MAI. The MAI patients have been confirmed to have internally rotated talus and no posteriorly positioned fibula, which may be related to the objective injury of the lateral ligament complex. 16 FAI patients do not exist significant lateral ligament injuries, however, the proprioceptive impairment plays an important role in the development of FAI. 32 As the stability of the ankle joint is dependent on the passive stability imparted by ligamentous structures and the articular geometry, and active stability from muscular support controlled by advanced nerve center. 33 –35 Meanwhile, long-term weightbearing movement around an abnormal axis of rotation may produce altered proprioceptive input to the central nervous system. Therefore, there may be interaction between the proprioceptive impairment and anatomical variation. Furthermore, it is necessary to assess whether there are significant anatomical variations in FAI patients. If so, treatment strategies especially surgical intervention should be used to restore native ankle joint motion and normal mechanics.
The critical difference between FAI and MAI is whether there is objective lateral ligament injury. Different types of CAI require different treatment strategies. FAI patients usually rely on balance, strength and proprioception training and to reduce the risk of ankle re-sprain. 36,37 On the contrast, MAI patients often require lateral ligament repair or reconstruction to restore normal ankle anatomy. Therefore, it is very important to accurately identify the patients with FAI or MAI when determining treatment strategies. Meanwhile, the recent studies increasingly raise doubts about the accuracy of direct MRI sign in diagnosing the lateral ligament injuries and identifying these two patients. 10,11,29,32 Based on this study, we would conclude that the MTI measurement alone is adequate to identify patients with FAI and MAI in the clinical practice, and the AMI and IMI are not helpful in this identification. However, the MTI has very narrow differences in comparison groups. We considered that the ankle mortise is a highly matched joint, and that the ankle was scanned in neutral position. Therefore, the talus rotation angle (i.e. malleolar talus index, MTI) is not so significant in absolute value, and the differences of MTI in comparison groups was also narrow.
Some limitations of the current study have also been noted. The first one was that the MRI scans were obtained in a supine and non-weight bearing position, potentially altering the calculated values of AMI, IMI and MTI. An MRI study of the weightbearing ankle may be needed, especially it would be more informative if the MRI measurements can be taken with the ankle under varus loading. What’s more, currently this measurement method has not been performed on MRI films outside the console computer. We believe it is feasible to directly use geometric tools for this measurement on MRI films outside the computer. And it will be helpful to expand the application range of this measurement method. Another limitation was that the sample size of the current study. Although it has met the minimum requirements, a larger sample size could be more accurate for analyzing. And a multi-center, prospective study is needed in the future to explore the relationship between anatomical variation and ankle pathological changes in patients with FAI and MAI.
Conclusion
In the present study, we found that the anatomical variation of ankle in FAI patients was completely different from that in the patients with MAI. The FAI patients did not have an internally rotated talus. And the MTI value may provide a new indirect MRI sign to identify patients with FAI and MAI.
Footnotes
Abbreviations
FAI: Functional ankle instability; MAI: Mechanical ankle instability; MTI: Malleolar Talus Index; AMI: Axial Malleolar Index; IMI: Intermalleolar Index; CAI: Chronic ankle instability; BMI: Body Mass Index; ICC: Intraclass Correlation Coefficient; ADT: Anterior Drawer Test
Authors’ note
Chengjie Yuan, Genrui Zhu and Zhifeng Wang contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (81572176), National Natural Science Foundation of China (81772416), Pioneering Project of Academy for Engineering and Technology, Fudan University, and Science and Technology Commission of Shanghai Municipality Fund (17XD1401000).