
Abstract
Purpose:
This study aimed to assess the accuracy of MRI in identifying ulnar collateral ligament (UCL), radial collateral ligament (RCL), and volar plate (VP) injuries of the metacarpophalangeal joint (MCPJ) of the thumb by comparing with diagnostic arthroscopy.
Methods:
A total of 56 consecutive patients (56 thumbs) who underwent arthroscopy of MCPJ of thumb were enrolled. MRI findings reviewed by consensus reading of two blinded radiologists were compared with arthroscopic examination. Statistical data, including sensitivity, specificity, accuracy, were analyzed. Additionally, the performance characteristics between 3.0-tesla (39 thumbs) and 1.5-tesla (17 thumbs) MRI and acute (≤4 weeks after injury) and chronic (>4 weeks) injuries were compared.
Results:
Of the 56 thumbs, 38 thumbs (67.9%) showed complete correspondence between MRI and arthroscopic findings. The sensitivity, specificity and accuracy of MRI for detecting UCL injuries were 78.8%, 87.0%, and 82.1%, respectively. The sensitivity, specificity and accuracy of MRI for detecting RCL injuries were 85.7%, 91.4%, and 85.7%, respectively. The sensitivity, specificity, and accuracy of MRI for detecting VP injuries were 89.5%, 89.2%, and 81.0%, respectively. 3.0-tesla MRI showed higher correspondence with arthroscopic observation (76.9%) than 1.5-tesla MRI (47.1%) (p = 0.028). For acute injuries, 78.4% showed complete correspondence between MRI and arthroscopic findings, whereas 47.4% with chronic injuries revealed complete agreement (p = 0.019).
Conclusion:
Overall, MRI is moderately effective in evaluating ligamentous lesions around MCPJ of thumb, but MRI is more sensitive in diagnosing acute injuries. Furthermore, 3.0-tesla MRI can provide results with better accuracy for diagnosing ligamentous lesions around MCPJ of thumb. However, the sensitivity and the specificity are not applicable to all ligament injuries, but only the severe one which would agree for surgical options.
Keywords
Introduction
Injuries around the metacarpophalangeal (MCP) joint (MCPJ) of the thumb, including ulnar collateral ligament (UCL) injuries, radial collateral ligament (RCL) injuries, and volar plate (VP) injuries, are common during contact sports or falls on an outstretched hand with the thumb hyperabducted or hyperadducted in a hyperextension position of the MCPJ. 1
Accurate identification of ligament injuries around the thumb MCJP is clinically important because it guides appropriate treatment, either immobilization or repair. 2 Most ligament injuries around the MCPJ of the thumb can be indirectly identified through physical stress tests and stress radiography that are considered first-line investigation methods if the injuries lead to gross instability. 3 However, when the instability is subtle, additional ancillary imaging studies that can accurately reveal the minute soft tissue structures may be required. 4 Magnetic resonance imaging (MRI) has been used for detecting intra- and extra-articular lesions in all joints of the body. 5 –8 Furthermore, MRI also can play an important role in surgical planning for better prognosis. 9, 10 While there is a large amount of scientific data on the use of MRI, establishing the injury pattern and a correct diagnosis in patients with hand injuries using MRI still remains a challenge. 11 –13
Although arthroscopy of the MCPJ of the thumb is even less commonly performed compared to other joints such as knee and shoulder joints, it presents a much clearer picture of the pathology compared with other imaging techniques or even open surgery. 9 There are no studies that assess the collateral ligaments and VP injuries of the MCPJ of the thumb while comparing MRI findings with arthroscopic examination. Therefore, this study aimed to elucidate the accuracy of MRI for diagnosing and identifying unstable ligament injuries around the thumb MCPJ and comparing the MRI findings with the arthroscopic examinations. The aim of this study was whether the accuracy of MRI was comparable to arthroscopy for the diagnosis of ligamentous pathology around the thumb MCPJ.
Materials and methods
Patient selection
The retrospective study was approved by the Institutional Review Board of the author’s institution. The data of all patients who underwent diagnostic arthroscopy for unstable ligament injuries around the thumb MCPJ, including UCL, RCL, and VP injuries, between September 2011 and August 2017 were identified from a clinical database and were used to establish the source of this study.
The indications for thumb MCPJ arthroscopy in our clinical practice are persistent pain or instability in the thumb, which was exacerbated by applying valgus and varus stress tests, regardless of MRI findings, despite conservative management for a 12-week period after injury or one of following conditions: (1) volar subluxation of the MCPJ, indicating complete tears of either or both of the radial and ulnar collateral ligaments 14 ; (2) avulsion fractures of the proximal phalanx at the insertion of the collateral ligament involving ≥10% of the articular surface and being displaced 2 mm or more; and (3) the complete tears of the ligaments including the UCL, RCL, or VP, diagnosed by MRI.
Surgical repair for unstable ligamentous lesions that were proven under arthroscopy was performed, but if the lesions were stable, only arthroscopic debridement was performed. All intra-articular avulsion fractures were reduced and set with K-wire (Kirschner wire) fixation under arthroscopic guidance. 15 All arthroscopic and surgical procedures were performed by the same surgeon.
The inclusion criteria for this study were the patients who were diagnosed with UCL and/or RCL rupture of the thumb MCPJ and who underwent arthroscopy. Patients with VP injuries were also included. The exclusion criteria were (1) concomitant open injuries or infection around the MCPJ of the thumb, (2) previous history of injection or surgery around the thumb MCPJ, (3) radiographic evidence of deformities or congenital anomalies of the thumb, (4) inflammatory or degenerative arthritis, and (5) instability similar to the unaffected side, indicating an extremely pliable joint.
MRI analysis
MRI studies were performed using either a 3.0-T imaging system (Ingenia; Philips Healthcare, Best, Netherlands) or a 1.5-T imaging system (Signa Excite, GE Healthcare, Chicago, IL USA). The patients were examined in the supine position with a neutral wrist position. Sagittal and coronal fat-suppressed T2-weighted images were obtained with an echo time of 65 ms and a slice thickness of 2 mm with no interslice gap. Sagittal and coronal T1-weighted images were obtained with an echo time of 15 ms and a slice thickness of 2 mm with no interslice gap. Axial fat-suppressed T2 and T1-weighted images were obtained with an echo time of 65 ms, and 15 ms, respectively, and a slice thickness of 3 mm with no interslice gap.
The collateral ligaments of the thumb MCPJ are composed of the proper collateral component, which inserts into the volo-ulnar base of the proximal phalanx, and the accessory collateral component, which locates volar to the proper collateral component and inserts into the volar plate. 16 If the MRI configuration of one or two components showed the separation between the ends of the ligament, the separation of the ligament from its bony points of insertion, or a Stener lesion, the ligament was assessed as a tear. 17 In a chronic injury, if the ligament showed thickening, thinning, irregularities, discontinuity, non-visualization, and alteration of the signal on MRI, we assessed the collateral ligament as injured. 18
The VP has a proximal attachment to the first metacarpal and a distal attachment to the proximal phalanx with extension between the radial and ulnar sesamoid bones. Volar plate injuries were recorded if MRI images revealed ligament disruption. 19
All MRI images were retrospectively interpreted, first independently and then in consensus, by two radiologists who had 14 years and 3 years of experience, respectively, in musculoskeletal imaging. The radiologists were unaware of the patients’ clinical information during their evaluation.
The sensitivity and specificity of MRI evaluation of both collateral ligaments and VP injuries around the thumb MCPJ were assessed using arthroscopic examination, which was performed by a hand specialist who had 13 years of experience, as the reference standard, according to the established procedure for the diagnosis and treatment of the thumb MCPJ injuries. 14,20
Surgical procedure
The patient was placed in a supine position under brachial plexus block anesthesia with shoulder abducted and the upper arm held on a hand table. The MCPJ of the thumb was stretched by applying about 10 lbs of tension after the arm was placed in a traction tower (Figure 1). Two standardized portals (dorso-radial and dorso-ulnar) were established in the interval between the collateral ligaments and either side of the central extensor tendon. 18 After about 2 mL of normal saline was instilled using a 23-G needle, an approximately 0.5 cm transverse incision was made along the skin crease, and the subcutaneous tissue was dissected using a fine mosquito forceps. A 1.9-mm arthroscope (30° lens; Smith & Nephew, London, UK) was introduced into the portal with caution not to scratch the articular surface of the joint. After debridement and synovectomy were performed with a 2.0-mm full-radius debrider and loose bodies were removed when encountered, the joint was inspected with continuous saline infusion.
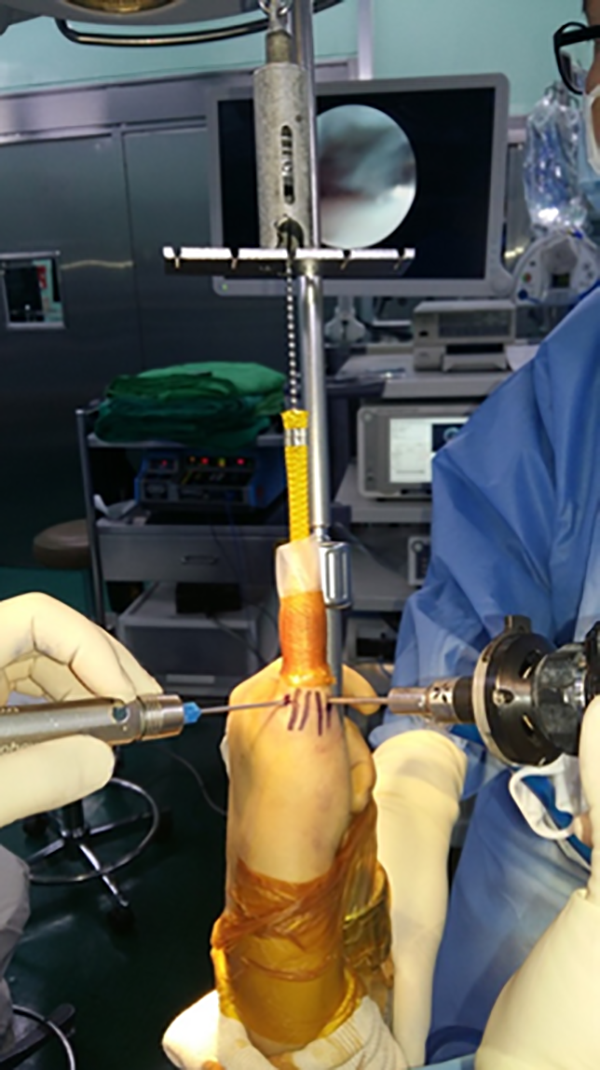
Arthroscopic examination of the metacarpophalangeal joint of thumb. About 10 lbs of tension of traction was applied to the thumb using a traction tower.
Collateral ligament tears at the base of the proximal phalanx or at the midsubstance were easily identified by simple observation, while avulsion injuries of the ligaments at the metacarpal head were detected by pulling the ligament into the joint using a probe (Figure 2). Avulsion fractures involving the articular surfaces were frequently noted. The Stener lesion initially showed a lack of UCL in the joint, which was easily reduced and repositioned back to its original position using a probe (Figure 3). 20 VP injury was identified by the hook test, which applies traction to the most-proximal border of the VP with the probe, or by observing a sesamoid fracture (Figure 4). If the VP was easily displaced toward the joint in the hook test or a sesamoid fracture was noted, the VP was considered to be injured. A sesamoid fracture occasionally accompanied collateral ligament injuries.

MRI and arthroscopic appearance of complete RCL tear. (a) Coronal view of T2-weighted MRI shows complete RCL tear at the proximal attachment site (arrow). (b) Arthroscopic findings demonstrated that the tear was detected by pulling the ligament into the joint using a probe (arrow heads). RCL, radial collateral ligament; MC-H, metacarpal head; PP-B, base of the proximal phalanx.

MRI and arthroscopic findings of Stener lesion. (a) Fat-suppressed T2-weighted coronal and (b) axial images reveal that the proximal part of the ruptured UCL (arrow) was displaced to a position proximal to the adductor aponeurosis which also shows a full thickness tear (arrow heads).
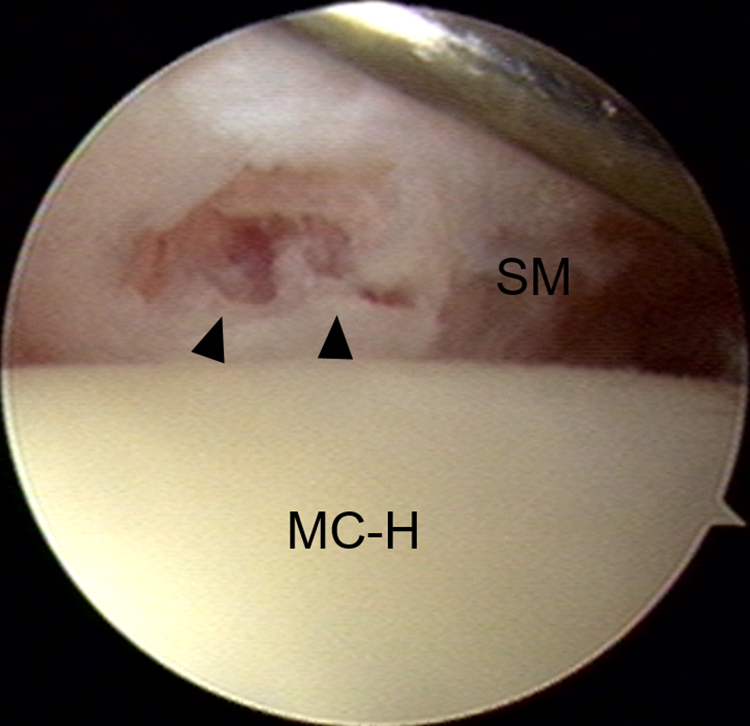
Arthroscopic findings of sesamoid fracture. Arrow heads indicates radial sesamoid fracture. MC-H, metacarpal head; SM, sesamoid.
Surgical options for the injuries were selected depending on the nature of the tear. Thus, complete tears of the collateral ligament were treated with open repair using suture anchors, while solitary injuries at the accessory collateral ligament without proper component injuries were treated with only arthroscopic debridement and immobilization, using a thermoplastic thumb spica cast. Avulsion fractures involving the articular surfaces were treated with an arthroscopically assisted reduction and percutaneous K-wire fixation. The injured sesamoid bone was excised using an arthroscopic small bur or shaver.
Statistical analysis
Statistical analysis was performed by an independent statistician. The sensitivity, specificity, and positive predictive value, negative predictive value, and accuracy of the MRI evaluation of the RCL, UCL, and VP injuries of the MCPJ of the thumb were assessed using arthroscopic findings as a reference standard according to the established procedure for the diagnosis. The performance characteristics of the 3.0-T and 1.5-T MRI as well as chronicity (≤4 weeks and >4 weeks after injury) for the diagnosis of ligamentous lesion around the thumb MCPJ were compared using a chi-squared test. Data were analyzed using SPSS software (version 18.0; IBM Corp., Armonk, NY USA).
Results
A total of 56 eligible patients (56 thumbs) met the criteria. There were 47 males and 9 females, with a mean age of 38.3 years (range, 15–62 years). The dominant hand was involved in 37 patients. 23, 15, and 7 patients were injured during sports activity, due to fall on outstretched hand, and from a traffic accident, respectively, and the other 11 patients were injured at work. 37 and 19 patients were treated acutely (≤4-week interval from injury to surgery) and subacutely or chronically (>4-week interval from injury to surgery), respectively.
The frequency of tears to ligamentous structures of the thumb MCPJ diagnosed by MRI and the surgery details are summarized in Table 1. According to the reference standard of operative findings, 19 thumbs involved an isolated UCL injury (33.9%), 10 thumbs involved an isolated RCL injury (17.9%), and 10 thumbs involved an injury to both collateral ligaments (17.9%). 17 of 56 thumbs (30.4%) were identified with having volar plate injuries. Among them, 14 thumbs (25%) involved an isolated volar plate injury and three thumbs had concomitant volar plate injury with collateral ligament injuries.
MRI and arthroscopic findings of the UCL, RCL, and VP injuries around the metacarpophalangeal joint of the thumb in patient group.

38 of 56 thumbs (67.9%) showed a complete correspondence between the MRI findings and surgical arthroscopy. Among the 18 cases that had a different diagnosis between the MRI and arthroscopic findings, five thumbs that seemed to have both UCL and RCL injuries on MRI were diagnosed to have an injury to only one collateral ligament based on arthroscopic examination: three UCL and two RCL injuries (Figure 5). Among six thumbs that presented as isolated collateral ligament injuries on MRI, five thumbs showed injuries at both the UCL and the RCL in arthroscopy, and the other thumb showed VP injury with sesamoid fracture, which required VP repair with sesamoid excision. Two thumbs identified as having an isolated VP injury on MRI showed associated tears of either the UCL or RCL in arthroscopy. Two cases were suspected to have both RCL and VP injuries on MRI, but arthroscopic findings revealed RCL injury alone in one thumb and both UCL and RCL injuries in the other thumb. The last case was suspicious of VP and both RCL and UCL injuries, but arthroscopic findings revealed an isolated RCL injury alone.

MRI and arthroscopic findings showing incomplete agreement between them. (a) Fat-suppressed T2-weighted MR image was interpreted to have both of RCL and UCL tears: arrow head; arrow, respectively. (b and c) Arthroscopic examination revealed proper component tear of the RCL alone without UCL tear (asterisk). RCL, radial collateral ligament; UCL ulnar collateral ligament; MC-H, metacarpal head.
The performance characteristics of MRI for the diagnosis of collateral ligaments and VP injuries are summarized in Table 2. No significant differences could be detected in the accuracy of the RCL, UCL, and VP injuries (p > 0.05) between MRI and arthroscopy. The overall sensitivity and specificity of MRI for detecting collateral ligament injuries and volar plate injuries were 84.7% and 89.2%, respectively. The overall accuracy of MRI was estimated to be 86.9%.
Sensitivity, specificity, positive predictive value, negative predictive value, accuracy and balanced accuracy for diagnosis of volar plate, ulnar and radial collateral ligament injuries on MRI.

* PPV: positive predictive value, NPV: negative predictive value.
When the performance characteristics of the 3.0-T and 1.5-T MRI for the diagnosis of ligament injuries around the thumb MCPJ were compared, the results for 30 of the 39 thumbs (76.9%) that used the 3.0-T MRI imaging corresponded with the arthroscopic findings. In contrast, when the 1.5-T MRI was used in 17 cases, and imaging results for 8 of them (47.1%) corresponded with the arthroscopic findings. The difference was significant (p = 0.028).
For acute injuries, 29 of 37 thumbs (78.4%) showed a complete correspondence between the MRI findings and surgical arthroscopy, whereas 9 of 19 thumbs (47.4%) with chronic injuries revealed a complete agreement between the MRI and arthroscopy (p = 0.019).
Inter-observer agreement was in “almost perfect agreement” with a weighted kappa coefficient of 0.84.
Discussion
Attempts to elucidate collateral ligament injury in a standardized manner, such as by clinical and radiological evaluations, may play a major role in determining the appropriate treatment such as immobilization or repair. 2 Failure to resist the stress test at the MCPJ of the thumb, where a laxity of 35° or more is noted when examined in full flexion, indicates a complete collateral ligament tear. However, the accuracy of the assessment of joint stability remains controversial due to practical difficulties, including local edema, poor patient compliance owing to pain, generalized laxity, and differences in collateral ligament laxity between the right and left thumbs. 21 Furthermore, radiological quantification of the laxity to stress is similarly difficult because the measurement of the laxity can be frequently affected by the patient’s position and the examiner’s interference.
According to early reports, the assessment of ligament injuries around the MCPJ of the thumb using MRI is highly accurate. 11, 22– 24 The sensitivity and specificity of MRI for diagnosing UCL tears of the thumb MCPJ approach 90 to 100% 2,25 Ahn et al. 11 examined 18 cadaveric thumbs using MRI and reported 90% accuracy for detecting the presence of UCL tears. Plancher et al. 12 reported 96% sensitivity and 95% specificity for MRI, which correlated with the surgical findings for identifying UCL rupture of the MCPJ of the thumb. On the contrary, Kevin et al. 22 who compared the preoperative imaging studies with surgical findings for the evaluation of UCL tear reported that the sensitivity of MRI was 64%. Even in all three digits where 3.0-T MRI scanning was used and documented, the MRI results did not correlate with the intraoperative findings. In the present study, 38 of 56 thumbs (67.9%) showed a complete correspondence between the MRI findings and surgical arthroscopy. However, we found that the correlations between preoperative MRI findings and arthroscopic examination for diagnosing each of the RCL, UCL, and VP injuries were moderately accurate. The overall sensitivity and specificity of MRI for detecting ligamentous injuries around the thumb MCPJ were 84.7% and 89.2%, respectively. The overall accuracy of MRI was estimated at 86.9%. On the basis of each specific injury, the accuracy of MRI for detecting UCL, RCL, and VP injuries was 82.1%, 85.7%, and 81.0%, respectively.
Since a clear demarcation between the proper and accessory collateral ligaments is not present on MRI, those ligaments run along the dorsal-to-volar course, which require additional sequential coronal images, and the signal intensity variation commonly presented in the collateral ligament may interrupt accurate assessment of ligament injuries around the thumb MCPJ. 3 Moreover, to acquire MR imaging of the thumb with a dedicated hand coil that is necessarily required in a high-resolution MRI, the patient could be positioned prone, with the arm positioned over the head in the so-called Superman position, which is not comfortable for all patients. This eventually can cause assessments with inaccurate images. Furthermore, the length of time from injury to presentation appears to have a negative effect on the accuracy of MRI, which was demonstrated in our study. Nonetheless, previous investigators reported a high accuracy of high-resolution MRI in diagnosing small joint lesions. 26,27 Anderson et al. 26 reported that the sensitivity, specificity, and accuracy of 3.0-T wrist MRI for the detection of triangular fibrocartilage complex injuries were consistently higher compared with those of 1.5-T wrist MRI. Hafezi-Nejad et al. 27 documented that 3.0-T MRI was superior to 1.5-T MRI in the diagnostic performance for the detection of scapholunate interosseous ligament injuries. Accordingly, our study demonstrated that 3.0-T MRI was considered superior to 1.5-T MRI for detecting collateral ligament or VP injuries of the MCPJ of the thumb. When classified according to the resolution of MRI, the agreement rate of arthroscopic examination with 3.0-T MRI findings was 76.9% and that with 1.5-T MRI findings was 47.1%, which was significantly different. However, there can be a high rate of false-positive results with high-resolution MRI, although the reproducibility of high-resolution MRI was superior. 28,29
To the best of our knowledge, no studies have assessed all of the collateral ligaments and VP injuries of the MCPJ of the thumb using MRI and compared the MRI findings with arthroscopic examination. There are a large number of studies comparing MRI findings with arthroscopic examination for other big joints. 17,30 –33 The reported sensitivity and specificity of MRI for assessing ligament injuries around the major joints were 9 to 100% and 38 to 100%, respectively. Therefore, in addition to MRI findings, the history of the patient, and physical and radiological findings, arthroscopic examination is important for assessing the extent of the injury and optimizing the surgical treatment of ligament injuries around the thumb MCPJ. 34,35
This study has several limitations. First, it is a retrospective study where we examined only those patients undergoing surgical intervention and were highly suspected of RCL, UCL, and/ or VP injuries of the thumb MCPJ. Thus, a selection bias may exist since the patients who were treated non-operatively, in whom MRI may have accurately identified the extent of the injury, were not included in our data analysis. In contrast, given that these patients would have been treated non-operatively, it would have been impossible to confirm the imaging findings. Second, this study did not assess the inter-observer reliability for assessing MRI findings and this might increase the accuracy of MRI because inter-observer agreement for MRI findings for soft tissue disruption has been reported to be low. 36 Finally, this study included acute (<4 weeks after injury) and chronic (>4 weeks after injury) injuries, which may not reflect the true accuracy of the MRI. 30
Conclusion
Overall, MRI is moderately effective in evaluating the ligamentous lesions involving the UCL, RCL, and VP around the MCPJ of the thumb. MRI is more sensitive in diagnosing acute injuries and the 3.0-T MRI can provide results with higher accuracy for diagnosing small ligamentous lesions around the MCPJ of the thumb. However, the greater emphasis for optimizing surgical treatment of unstable ligament injuries around the thumb MCPJ remains on arthroscopic findings and physical examination.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.