
Abstract
Background:
In view of preventing surgical site infection (SSI) in the orthopedic operating room (OR), evidence concerning types of footwear and clothing is limited. This study aimed to investigate how different footwear and clothing affect the cleanliness of the OR environment.
Methods:
The airborne dust concentration in a bioclean room (NASA class 100) was measured around an operator by using a handheld particle counter under the following conditions: (I) wearing a sterilized full-type space suit with OR dedicated clean sandals; (II) wearing a sterilized full-type space suit with non-dedicated (outside) shoes or severely contaminated outside shoes with surgical glove powder (2 µm mean particle size); and (III) wearing an unsterilized medical scrub uniform with OR dedicated sandals. The participant was standing still or stepping in place at 1 Hz during the testing.
Results:
The concentrations of airborne dusts in the operative field were independent of footwear and clothing types under the stand-still condition. However, these values significantly increased 1.96- to 16.23-fold after simple stepping motion in all the test conditions, and often became dissatisfaction level with the NASA100 requirement for the OR cleanliness. The worst contamination occurred when an operator wore the powder-contaminated shoes and also the unsterilized scrub uniform.
Conclusion:
The present study showed that the stepping motion triggered a considerable contamination in the operative field (beyond the level of NASA100 threshold) particularly when an operator used the outside shoes or unsterilized scrub uniform. Therefore, these results tell us that the one-footwear system (i.e., no use of OR dedicated clean shoes) and unsterilized scrub are likely to be a potential risk factor for SSI. Nevertheless, further studies are necessary to conclude the real efficacy of OR dedicated shoes and sterilized clothes on the SSI prevention.
Keywords
Introduction
Airborne wound contamination and surgical site infection (SSI) remains a concern in patients who underwent total joint replacement (TJR), potentially leading to a disastrous infection. The risk of SSI can be divided into intrinsic and extrinsic factors. The former factors generally include a surgical history, diabetes mellitus, undernutrition, excessive obesity, hepatic and renal dysfunction, heavy smoking, alcohol consumption, and drug addiction. 1 In recent years, preoperative nasal carriage was identified as an additional intrinsic factor for SSI. 2 –5 On the other hand, the latter factors are associated with the surgical environment such as cleanliness in operating room (OR), various intraoperative maneuvers and motions of medical staffs, and the presence of occasional staffs and visitors with unsterilized clothes. 6 –8 The measurement of airborne dust/bacterial concentration in the operative field is an important approach to evaluate a potential extrinsic risk factor for SSI. 9 –11 A source of airborne contamination in OR is redispersed floor bacteria. 12 Thus, OR staffs, their motions, and shoe/clothing types can be a potential contamination source, and their impacts under different air-distribution strategies on intraoperative contamination and infection control should be considered quantitatively.
According to the national survey on SSI conducted by the Japanese Orthopaedic Association (JOA), the incidences of SSI were reported as 1.36% (134 of 9882 patients) after TJR. 13 This survey reported the use of outside shoes in OR as a potential extrinsic risk factor for SSI. In opposition to such finding based on the nationwide data, there is an increasing recent trend toward “the one-footwear system” in Japanese hospitals, i.e. no use of OR dedicated clean shoes. This circumstance may arise as a result of a lack of clear scientific evidence to support the use of OR dedicated shoes, and its effectiveness (or ineffectiveness) should be proved through further experimental as well as clinical studies. In fact, very few evidences have been reported so far on the effects of footwear and surgical clothes in combination with surgeon’s motion on the operative field contamination. In the above context, the present study was designed to experimentally clarify the impact of footwear and clothing on intraoperative contamination by measuring airborne dust concentration in the operative field.
Methods
This study was preliminary approved by the Institutional Review Board (IRB) and has been performed in accordance with the ethical standards as certified by our ethics committee board.
The airborne dust concentration in a bioclean room was measured around an operator by using a handheld particle counter (KC-52, Rion Co., LTD., Tokyo, Japan). All testing was performed in a vertical laminar airflow surgical theater (room volume: 130.75 m 3 ; floor area: 44.25 m 2 ) which satisfies a standard for clean room of National Aeronautics and Space Administration (NASA class 100). The particles were counted one by one using a photodiode detector, and coincidence loss occurs when two particles pass through the sensor at the same moment. In the counter used, the coincidence loss is within 10% of the indicated readings at a count of 1.4 × 105 particles per cubic meter. The airborne particles in the size of ≥0.3 µm (roughly corresponding to a diameter of squamous epithelial cells 14 ), were counted within the volume of ≈2.83 m 3 around the detector for 1 min.
The measurements were performed at the height of an operating field (100 cm from the floor) (Figure 1a–b). The distance between the measurement equipment and the experimenter was set at 30 cm. A data-sampling interval was set at ≥10 min to stabilize a baseline particle level in the OR, and the recorded data of six successive measurements were averaged in each test condition. Note that the OR cleanliness of <100 n/ft3 is necessary to satisfy the NASA100 criteria.

Photographs of clothing (sterilized full-type space suit or unsterilized scrub uniform) and footwear (OR dedicated sandals or outside shoes) to represent the test conditions (I)–(III). The arrows indicate a handheld particle counter.
As shown in Figure 1a–d, all testing was conducted by the same single participant (TT) under the following conditions: (I) wearing a sterilized full-type space suit (Stryker Instruments, Kalamazoo, MI, USA) with OR dedicated clean sandals; (II) wearing a sterilized full-type space suit with non-dedicated (outside) shoes or severely contaminated outside shoes with surgical glove powder (2 µm mean particle size); and (III) wearing an unsterilized medical scrub uniform (FOLK Co., LTD., Tokyo, Japan) with OR dedicated sandals. The data comparison between the above test conditions (I) and (II) can emphasize the effect of footwear types on the intraoperative contamination (i.e., OR sandals vs. outside shoes), whereas the comparison between the test conditions (I) and (III) can emphasize the effect of clothing types on the contamination (i.e., space suit vs. scrub uniform). The space suit used had the battery-operated cooling fan incorporated into the inner helmet, and, as in the routine preoperative procedure for a clean operation, the participant with the space suit put on the double gloves using the closed-gloving technique. The participant was standing still or stepping in place at 1 Hz during the testing, whose motion conditions were referred to as stand and step, respectively. The condition using powder-contaminated shoes were referred to as powder. The powder contamination was made by intentionally touching the outer surfaces of outside shoes with surgical gloves (i.e., contaminating the shoes with the powder of the gloves), and subsequently the gloves were disposed of before testing so that the influence of residual powder in the gloves were not included as a part of the experimental condition. The OR used in this study was cleaned and the floor was wiped before testing in each condition.
Data was presented as mean ± standard deviation (SD) and was analyzed using the Mann–Whitney U test with the aid of the Graphpad Prism software, version 8 (GraphPad software, Inc., San Diego, CA), to test for statistically significant differences of the concentrations of airborne dusts among the different experimental conditions. The statistical differences were considered significant at the P < 0.05 level.
Results
Effect of footwear types on airborne contamination
The mean concentrations of airborne dusts (mean ± SD) in the operative field were 49.3 ± 4.1 and 49.5 ± 13.4 n/ft3 in the test (I)-stand and (II)-stand, respectively, and no significant difference was found between the stand conditions (P = 0.5628) (Figure 2 and Table 1). These contamination levels significantly increased up to 96.8 ± 17.2 n/ft3 in the test (I)-step (1.96-fold increase compared to the (I)-stand, P = 0.0022) and 118.8 ± 31.3 n/ft3 in the test (II)-step (2.40-fold incrase compared to the (II)-stand, P = 0.0022), potentially leading to dissatisfaction with the NASA100 requirement for the OR cleanliness due to the simple stepping motion. However, no statistical significance was noted between the (I)-step and (II)-step (P = 0.1190). On the other hand, the significantly greater dust concentration (198.3 ± 67.4 n/ft3) was noted in the (II)-step_powder as compared to the (I)-step (2.05-fold increase, P = 0.0022) as well as (II)-step (1.67-fold increase P = 0.0087), suggesting the degree of surface dirtiness of footwear may affect the risk of intraoperative contamination.
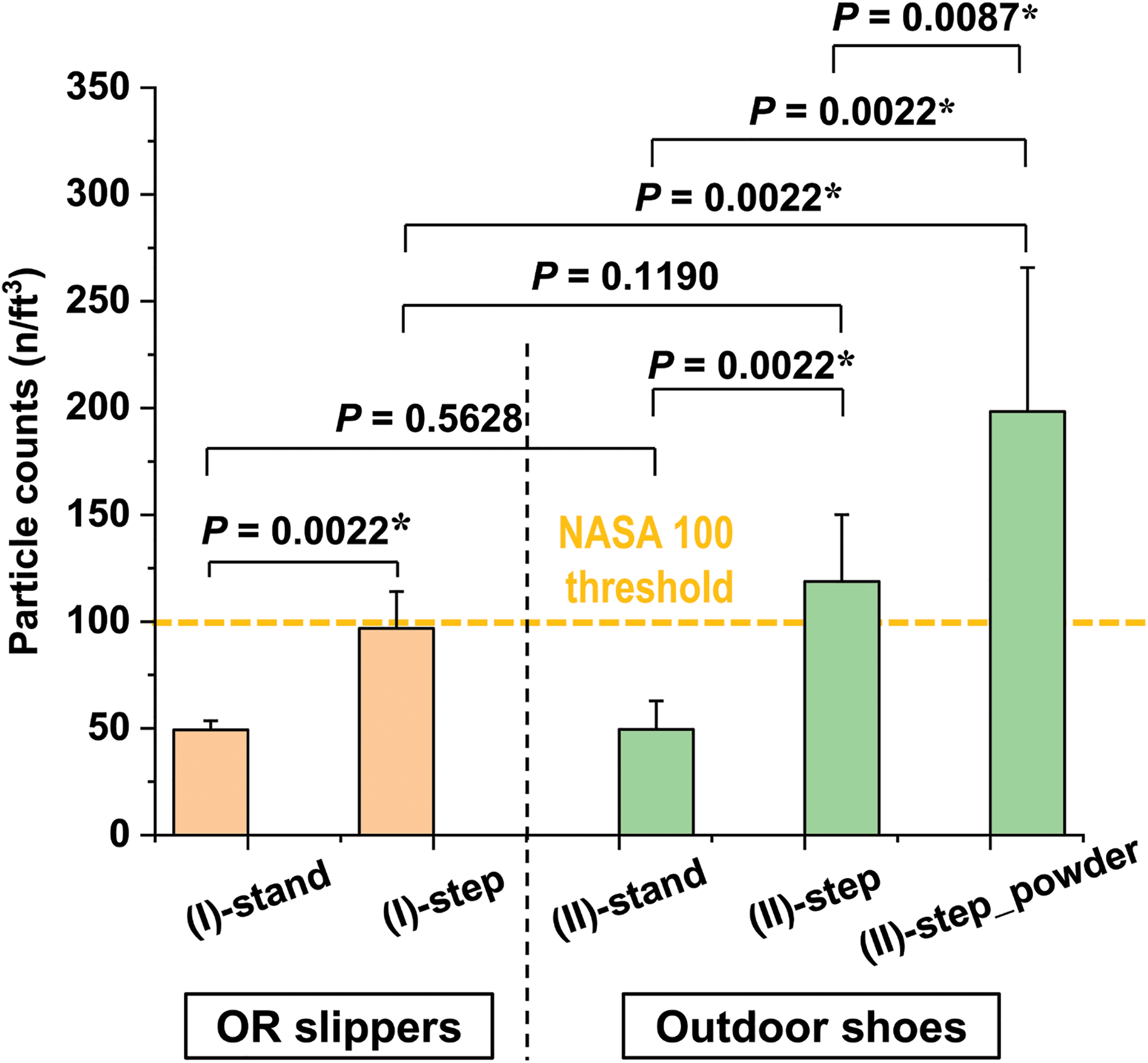
Comparisons of the airborne dust concentrations between the test (I) and (II). The statistical significances for each comparison assessed by the Mann–Whitney U test were given in each comparison. The bars and error bars indicate mean ± SD. The asterisks represent P < 0.05.
The airborne dust concentrations (n/ft3) in each condition tested in this study.
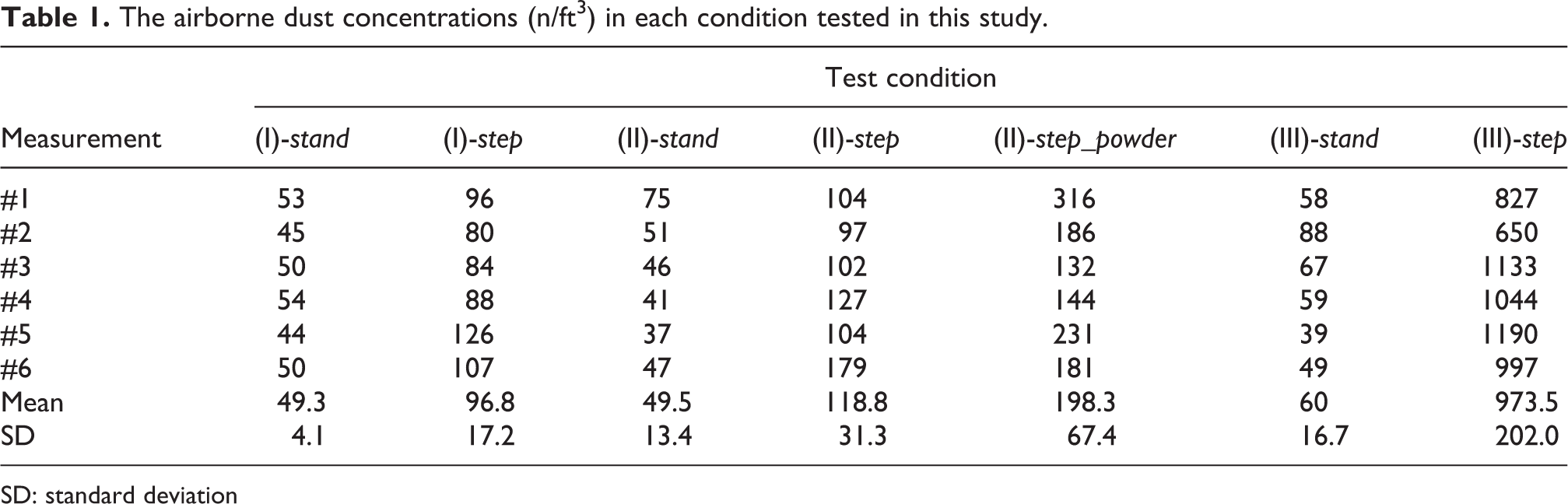
SD: standard deviation
Effect of clothing types on airborne contamination
The dust concentration was 60.0 ± 16.7 n/ft3 in the test (III)-stand and no significant difference was found between the (I)-stand and (III)-stand (P = 0.2208, Figure 3 and Table 1). However, a dramatic increase was observed after stepping (973.5 ± 202.0 n/ft3), which substantially exceeded the NASA 100 threshold for OR cleanliness. Statistically significant contamination was noted in the (III)-step as compared to the (III)-stand (16.23-fold increase, P = 0.0022) and the (I)-step (10.06-fold increase, P = 0.0022). In this context, stepping with an unsterilized medical scrub uniform in OR may entail significant risk of intraoperative contamination.
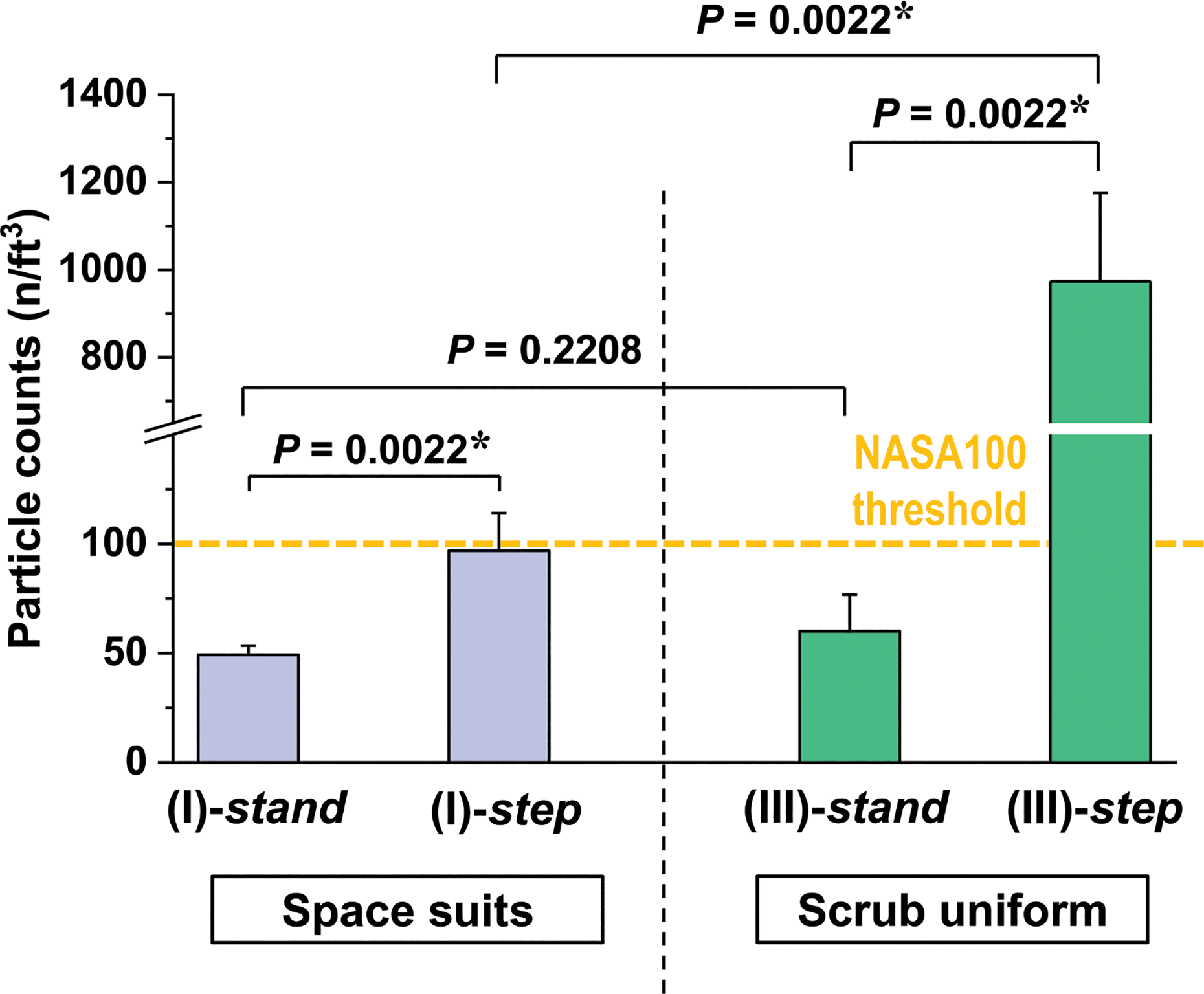
Comparisons of the airborne dust concentrations between the test (I) and (III). The statistical significances for each comparison assessed by the Mann–Whitney U test were given in each comparison. The bars and error bars indicate mean ± SD. The asterisks represent P < 0.05.
Discussion
Regarding the footwear types, the Centers for Disease Control and Prevention (CDC) guidelines supported the one-footwear system on the basis of the finding that no significant difference was observed in the incidence of SSI between outside shoes and OR dedicated shoes. 15 In Japan, it was previously reported that no use of OR dedicated shoes did not significantly affect environmental cleanliness in OR as well as intensive care units (ICU) under the legally-approved air-conditioning. 16 So far, there remains little or no evidence to suggest the use of OR dedicated shoes, and accordingly the number of hospitals adopting the one-footwear system is currently growing in Japan. Nevertheless, outside shoes should present a potential source for postoperative infection by carrying numerous bacteria. 17 One recent study introduced in JOA Clinical Practice Guideline on the Prevention of SSIs in Bone and Joint 18 showed a greater rate of SSI in outside shoes than OR dedicated shoes in spinal instrumentation surgery. In view of the fact that shoes worn outside may be grossly contaminated, the 2018 International Consensus Meeting (ICM) on Musculoskeletal Infection recommended with a strong consensus that outside shoes should not be worn in orthopedic ORs, or shoes covering should be worn to prevent the contact of outside shoes with OR floors, although the level of evidence is still limited. 19
Our study demonstrated that footwear types did not significantly affect the airborne dust concentration under the stand-still condition (Figure 2). However, it is noteworthy that the effect of different footwear types was significantly enhanced by operator’s stepping with the powder-contaminated outside shoes, suggesting that higher degree of footwear dirtiness may be associated with greater risk of intraoperative contamination. In practice, since cleanliness level of outside shoes is uncertain, its use may not be recommended. It should be also noted that simple stepping alone substantially increased the dust level regardless of the footwear types and even OR dedicated shoes potentially lead to dissatisfaction with the NASA100 requirement for the cleanliness after stepping. Thomas et al. 20 previously investigated the degree of contamination of OR dedicated shoes after cleaning. They concluded that current shoe cleaning practices are still ineffective and the clean appearance of OR dedicated shoes showed unreliable indication of bacterial contamination. In the above contexts, even when the OR dedicated shoes were used, intraoperative movement should be minimized to maintain the NASA100 requirement.
On the other hand, regarding clothing types, infection rates after TJR were previously reported to be higher in sterilized space suits than in standard gowns. 21 Nakajima et al. 11 recently pointed out a problem of increased contaminants due to a full-type space suit. They demonstrated that simple stepping of a single surgeon with space suit resulted in 31-time greater contaminants in the operative field than the stand-still condition whose increase was interpreted as a consequence of the outflow of cooling air from the hem of the space suit. Our current study also demonstrated that clothing types significantly affect the airborne contamination (Figure 3) and it was likely that their effect on infection risk was rather greater than that of footwear types. The important finding was that unsterilized scrub uniform was associated with a great risk of airborne contamination. Therefore, the OR admission should be restricted to staffs wearing unsterilized scrub, and again this data suggest that intraoperative movement should be minimized to maintain the NASA100 requirement.
As to the association between airborne bacteria and SSI, a strong consensus was achieved at the 2013 ICM on Periprosthetic Joint Infection (PJI) as follows 1 ; “airborne particulate bacteria are a major source of contamination in the operating room environment and that bacteria shed by personnel are the predominant source of these particles. The focus of our recommendations is to reduce the volume of bacteria in the operating room with particular attention to airborne particles.” Furthermore, regarding the movements of staffs in OR, the meeting participants unanimously agreed to recommend that “operating room traffic should be kept to a minimum.” The experimental evidence obtained from the present study can strongly support the above statement. In addition, since the number of airborne microorganisms increases proportionally to the number of staff members in OR, the following considerations should be taken into account: (1) minimizing the number of staffs coming in and out from OR 22 ; (2) maintaining higher air pressure in OR than outside; and (3) using air filters. 23,24 Nevertheless, in a real clinical practice, many staff members move around during the period from anesthetic induction to extubation. Especially in teaching hospitals, relatively many people can enter and exit OR for education of medical students, healthcare professionals, et al. For prevention of SSI, it would be necessary to implement measures concerning the movement of individuals involved in OR procedures.
This study has limitations. First, there are differences in the environmental conditions between the present study and actual arthroplasty (e.g., the number of medical staffs, their motions, door opening/closing frequency). We included only 1 participant during standstill and intraoperative motion, and the door in the OR was kept closed throughout the test. Therefore, the tested OR environment is less number and activity of people compared to actual arthroplasty. Second, the particle size of <0.3 µm was not considered. Third, the detection of airborne particles was approximately limited within the volume of 2.83 m 3 (with radius of sphere ≈88 cm) around the handheld counter placed at a height of an operative field, and we did not consider the influence of airborne contaminants and microbial level in the outside of the detection area. In the above contexts, our testing condition can be regarded as a milder simulation for intraoperative contamination as compared to that in the actual arthroplasty. The number of airborne microorganisms in the OR are directly proportional to the number of staff present in the OR, 24 and also linked to the frequent opening of the OR door. 24,25 In addition, door openings increase in direct proportion to case length, and have an exponential relationship with the number of persons in the OR. 8 During surgery, multiple medical staff members can make various motions in the OR such as ambulation of surgeons/ nurses, holding patient’s legs and feet by assistants, and preparation for implantation materials and bone cement, et al. In a normal OR condition, the main surgeons wear the condition either (I) or (II), while supporting staff tends to wear the condition (III), and each often at different distances from the OR table. The traffic across all specialties may be a potential risk factor to compromise the sterile environment of the OR. The borderline distance from the operative field remains unknown, and it may change depending on the conditions of airflow as well as the number/ sizes of contaminants attached to each staff present in the OR. However, the investigation on the above influence is beyond the scope of this study. Fourth, the measured concentration of airborne dusts may not reflect directly the occurrence of SSI. Nevertheless, it was previously reported by a Medical Research Council that there was a correlation between contamination level in air and frequency of postoperative SSI. 26
Despite the aforementioned limitations, the present study showed that the intraoperative motion triggered a considerable contamination in the operative field (beyond the level of NASA100 threshold) particularly when an operator used the outside shoes or unsterilized scrub uniform. Therefore, these results tell us that the one-footwear system and unsterilized scrub are likely to be a potential risk factor for SSI. Nevertheless, further studies are necessary to conclude the real efficacy of OR dedicated shoes and sterilized clothes on the SSI prevention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.