
Abstract
Purpose:
The aim of the study was to evaluate whether or not there was any incompatibility between two-strand hamstring tendons taken from the same knee and the ATFL and it was the determination of suitable footprint points in the fibula and talus for anatomical ATFL reconstruction.
Methods:
16 fresh frozen cadaver specimens were dissected to gracilis and semitendinosus tendons and the anterior talofibular ligament. The origins, insertions, distances from osseous landmarks of fibular talus of ATFL were determined. The diameters of gracilis, semitendinosus and ATFL were calculated. There was a moderate correlation between body height and the distance between the distal of inferior lateral malleolus and the fibular adhesion site of ATFL (r: 36.5 p: 0.036). There was a weak correlation between body height and the distance between the apex of the lateral talar process and the talus adhesion site of ATFL in a single bundle (r: 28.4 p: 0.002). There was no correlation between the distance from proximal and distal adhesion side of ATFL and body height in the double bundle (p: 0.241).
Results:
There was no significant relationship between ATFL diameter and gracilis, semitendinosus and both hamstring in women. A significant relationship at 80.5% was determined between the ATFL and the gracilis diameter in man. A significant relationship at 92.6% was determined between the ATFL and the semitendinosus diameter in man.
Conclusion:
It was determined that there is not compatibility between the gracilis tendons, the semitendinosus tendon and ATFL in women. It should be supported by biomechanical and clinical studies whether this incompatibility has a clinical effect or not.
Introduction
Ankle lateral collaterals consist of three ligaments: anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), posterior talofibular ligament (PTFL). The anatomical location of the ATFL starts from 10 mm proximal to the type of the distal fibula and ends 18 mm below the articular cartilage of the talus. 1 ATFL plays an important role in limiting anterior displacement of the talus and plantar flexion of the ankle thus ATFL provides primary stability in internal rotation and inversion that is the most common mechanism of injury to the ankle ligaments. 2,3
In ankle sprains, ATFL is affected by 66–85%. 4,5 Although most of the patients with ATFL injuries were successfully treated with conservative methods such as splinting and rehabilitation. Chronic instability were observed 20% of patients who were not treated correctly in clinical studies. 6 –8 20–40% of these patients needed surgical intervention. 9 Surgical methods such as anatomic ligament repair, nonanatomic tenodesis and anatomical ligament reconstruction are used for ATFL rupture. 1 In chronic ankle instability, surgical methods such as nonanatomic tenodesis or anatomic ligament repair are used when primary repair is not sufficient because of defects due to degeneration at ATFL. Although nonanatomic techniques have been successful in patient satisfaction, they are often not preferred because of instability of the subtalar joint, long-term osteoarthritis and limited ankle movements. 1 Therefore, anatomic ligament reconstruction is preferred in chronic ankle instability and in cases where primary repair cannot be performed.
In the literature, gracilis, semitendinosus and patellar tendon are frequently used as grafts for reconstructive surgery in chronic ATFL injury. 10 –12 It has been shown that the thickness and length of hamstring tendons vary according to body mass index, gender and side. 13 Variations of the starting and ending point in different joints have been shown to have an effect on tendon survival, stability and joint movements in reconstructive surgery. 14,15 Therefore, evaluating the relationship of these variations with ATFL and the anatomic origin and endpoint for ATFL could have an impact on surgical success.
We had two purposes in this study, first to compare the ATFL and hamstring tendons on the same knee. Second to evaluate appropriate starting points and endpoints for ATFL reconstruction surgery.
Material and method
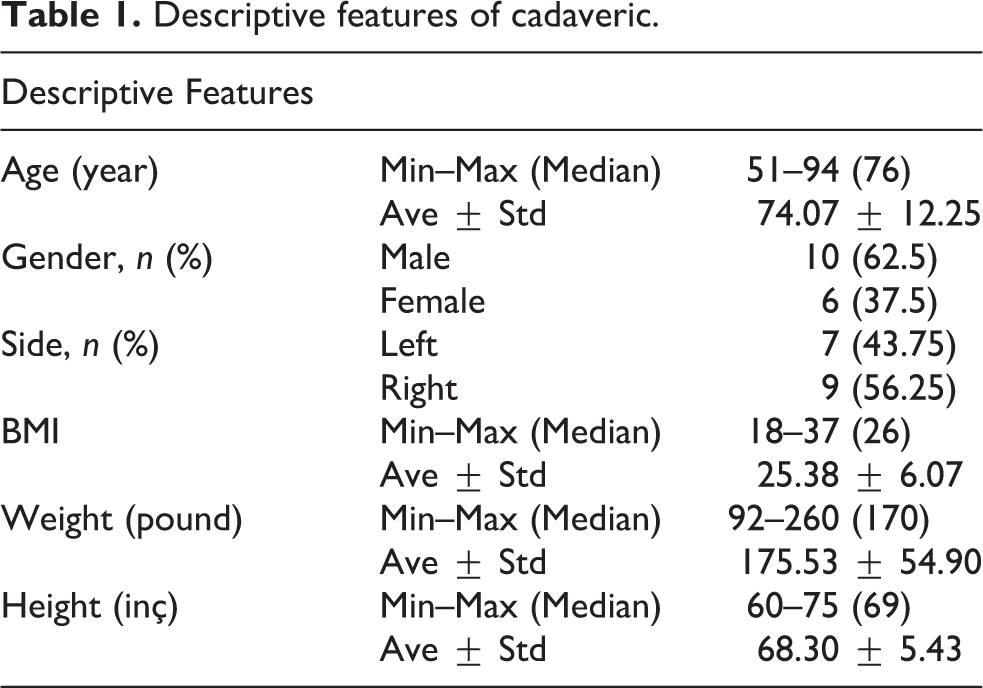
This anatomical study included 16 nonpaired leg of fresh frozen cadavers which had been stored at +4°C. No leg showed any scar of previous surgery or evidence of clinical deformation in the frontal plane (Table 1). The average conservation time from death to dissection was 1 month. Preoperative ankle roms were measured by goniometer and ankle movements were normal.
Descriptive features of cadaveric.
Exclusion criteria were: significant osteoarthritis (>Outerbridge grade 3), ligament injury to the medial or lateral ankle, damage hamstring tendons.
Superficial muscle tendons and fascia were carefully removed and exposed the ankle lateral collaterals. The lateral aspect of the ankle was carefully dissected with 2.5 surgical loupes. ATFL starting points and end points were evaluated at the ankle neutral position (plantarflexion/dorsiflexion of 0°). ATFL width was measured using calipers at three sites, a proximal site (fibular attachment), an intermediate site, and a distal site (talar attachment), and the mean values were used. 16 All dissections were done by same person because of eliminating interobserver variability.
Evaluating starting points and end points
The centers of osseous adhesion points of the ATFL in the fibula and the talus were defined. These points were measured between the distal of inferior lateral malleolus and the fibular adhesion site of ATFL and the distance between the apex of the lateral talar process and the talar adhesion site of ATFL. In those with two bundle, this method was measured as proximal bundle and distal bundle.
Hamstring graft preparation
A standard open anteromedial approach of the joint was carried out. Gracilis and semitendinosus tendons were identified at their tibial insertion site and harvested using a closed stripper after a standard release procedure. After the graft was prepared and cleansed from adherent muscle and adipose tissue, the tendon was applied to a 89 newton load for 15 minutes and each tendon diameters were calculated from the surroundings of the double-strand tendons with a digital microcaliper with a resolution of 0.1 mm and an accuracy of 0.02 mm (Neiko 01407A Electronic Digital Caliper, Neiko Tools, China), separately. The thickness was measured at three different points of each specimen and the mean width recorded. 17 –19
Statistical analysis
The results were analyzed by using IBM SPSS v. 22 (IBM Corp.; Armonk, NY, USA). Descriptive statistical methods (mean, standard deviation, median, frequency, percentage, minimum, maximum) were used to evaluate the study data. The suitability of the quantitative data for normal distribution was tested with the Shapiro-Wilk test. Student T test was used for comparison of two groups of quantitative variables showing normal distribution. Mann Whitney U Test was used for comparison of two groups of quantitative variables that did not show normal distribution. Pearson correlation test was used to evaluate the relationships between the parameters. Significance was evaluated at least p < 0.05.
Results
In a single bundle, the distance between the distal of inferior lateral malleolus and the fibular adhesion site of ATFL was averaged 14.42 (13.50 to 15.6) mm, the distance between the apex of the lateral talar process and the talus adhesion site of ATFL was averaged 11.62 (10.40 to 12.40) mm (Figure 1). There was a moderate correlation between body height and the distance between the distal of inferior lateral malleolus and the fibular adhesion site of ATFL (r: 36.5 p: 0.036). There was a weak correlation between body height and the distance between the apex of the lateral talar process and the talus adhesion site of ATFL in a single bundle (r: 28.4 p: 0.002). There was no statistically significant difference between the distance adhesion side and gender in a single bundle (p: 0.412).

Lateral view of a right ankle in neutral position, showing attachment sites of single bundle of ATFL.
In the double bundle, the fibular footprint centers of the superior and inferior bands of ATFL were averaged 16.45 (15.8 to 17.05) mm and 10.73 mm (9 to 12.1) mm, respectively, from the inferior tip of the lateral malleolus at the anterior fibular border. The talar footprint centers of the superior and inferior bands of ATFL were averaged 21.40 (20.5 to 21.90) mm and 11.40 (9.20 to 12.50) mm, respectively, from the apex of the lateral talar process. There was no correlation between the distance from proximal and distal adhesion side of ATFL and body height in the double bundle (p: 0.241) There was no statistically significant difference between the distance from proximal and distal adhesion side of ATFL and gender in the double bundle (p: 0.16) (Figure 2).

Lateral view of a right ankle in neutral position, fibular and talar foot prints of the superior and inferior bands of ATFL.
There was no statistically significant difference between ATFL, gracilis, semitendinosus, and both hamstring (gracilis + semitendinosus) tendon diameters according to descriptive data of cadevery (p > 0.05).
There was no significant difference between the number of bundles and gender. Single bundle thickness was 7.29 ± 0.28 mm and double bundle thickness was 7.96 ± 0.55 mm. There was no significant difference between bundle number and gender and height groups (p > 0.05). Tendon and ligament diameters according to gender and side are shown in Table 2.
The diameter of tendons and ligaments according to side and gender.a

a Values are mean ± SD.
A strong correlation was observed between ATFL diameter and gracilis and semitendinosus diameter (respectively; 80%, 92%). Strong correlation between ATFL diameter and gracilis (r: 0.79) and semitendinous (r: 0.98) and both hamstring (gracilis + semitendinosus) (r: 0.95) tendons was observed in males. There was no correlation between ATFL diameter and gracilis, semitendinosus and both hamstring (gracilis + semitendinosus) tendon diameters in women (Table 3).
Correlations of the hamstring tendons diameter with the ATFL diameter.

a p < 0.001: Pearson correlation analysis.
b p < 0.05: Pearson correlation analysis.
Discussion
The most important findings of the study was a strong correlation between ATFL diameter and gracilis, semitendinosus tendon diameter in men, whereas no correlation was observed between ATFL diameter and gracilis, semitendinosus tendon diameter in females. It was observed that the mean diameter of semitendinosus was closer to the ATFL diameter than the average diameter of gracilis.
Edama et al. in a cadaver study of 83 legs, the ATFL ligament was closely associated with the ankle capsule and was seen as 33% single band, 57% two band, and 10% three band. 20 Milner and Soames cadaver study, 38% single bundle 50% double bundle 12% three bundle was observed. 21 In our study, we observed a single bundle in 5 patients and a double bundle in 11 patients during ankle dissection. Three bundles were not seen. We used 16 cadavers in this study, and this difference in bundle numbers could be due to the different number of cadavers used in other studies. However, there is no study available evaluating whether anatomical variations have clinical and functional significance in the literature.
It is important to define ligament footprint centers for success in anatomic reconstruction of injured lateral ankle ligaments. Open or arthroscopic techniques for ATFL reconstruction including different tunnel and tendon configurations have been described. For isolated ATFL injury, fixation with single or double tunnel, gracilis and/or semitendinosus graft has been identified, but different tunnel position and tendon configurations are also available due to CFL injury, which is often associated. 12,22 –24 However, there are not enough studies comparing these surgical techniques. In cadaver studies, there were variations in ATFL fibular and talus adhesion sites and bundle number and the bundle type has been shown to have an impact on fibular and talar adhesion footprint. 21,25 Similarly, in our study, variations between bundle type and adhesion points were observed. We think that tunnel position and tendon selection may affect clinical outcomes by evaluating these variations. On the other hand, it may not be possible to evaluate the bundle type and footprint of the injured ATFL in chronic cases because of degeneration at ATFL. In our study, similar to the literature, it was observed that the fibular and talar adhesion point has a wide variation. When we evaluate the height and the adhesion points, a moderate correlation was observed in the talar footprint and a weak correlation was observed in the fibular footprint in the single bundle. On the other hand, no correlation was observed in the double bundle. This suggests that it is more difficult to determine the exact footprints in people with multiple bands. In the literature, anatomical variations were observed in the number and thickness of ATFL bundles according to gender. Even differences between the right and left sides of the same cadaver were observed. 26 In our study, variations by gender was not observed. According to side, variation was not evaluated because the cadaveric legs were not paired in our study. In the light of these data, we think that anatomical footprints may not be fully evaluated in chronic cases.
It has been shown that the thickness of hamstring grafts varies according to gender and that is correlated with ACL and PCL tendon thickness. 13,17 In the literature, there is no study showing the relationship between the thickness of ATFL and the thickness of hamstring tendons. In our study, it was found that the thickness of ATFL was correlated with the thickness of hamstring tendons in men. However this correlation was not seen in women. Suitable tendon type and diameter for ATFL surgery have not been defined in the literature. It should be supported by biomechanical and clinical studies whether this incompatibility has a clinical effect or not.
In comparison with other cadaver studies which have defined ATFL, the mean age of the cadavers, the mean BMI measurements have been reported to be similar to our study but this cadaveric specimens mostly embalmed specimens. 26,27 In our study, we used fresh-frozen, nonpaired specimens that is proper evaluation of tendons and ligament of anthropometry. 25 The diameters of the hamstring tendons were measured while applying 89 newtons of force for reduce graft creep in our study that is similar to literature. 18,28 This force pass from the toe region to the elastic region in the yield curve and provide a more uniform measurement. 29,30 To reduce the effects of the irregular shapes of the tendons, a double strand was made and measured from the thickest part. Although there are different instruments in the literature as measurement material, digital microcaliper was preferred because it is more sensitive and reliable. 17
In the literature, lots of osseous references point defined for the locations of origins and insertions. Two osseous reference points, anterior tubercle of fibula and tip of the fibula, have been identified for the origins of ATFL. 31,32 Two osseous reference points, apex of lateral talar process and inferior corner of talar body, have been identified for the insertions of ATFL 25,31 but there is no reproducible and consistent osseous landmark. 23,33 In our study, we evaluate the distance from the tip of the fibula and inferior corner of talar body. We believe that these osseous marker is the most reproducible reference landmark because it is easily palpated during lateral ankle surgical exposures. We use small measured parameters, that was reported ±0.1 mm, so the measured parameters was accurate to that scale. 25
There are several limitations in our study. First was the low number of cadavers and second was the average age of cadavers exceeding the average age of patients undergoing ATFL surgery. The absence of any intra-articular pathology, different tendon and ligament pathologies in the evaluated cadavers reduces the possible measurement changes due to degeneration. Third was average results are used in the measurement of irregular shapes of tendons and ligaments. Lastly, the tendons and the ligaments were evaluated only according to their diameters, thus, they should be confirmed by biomechanical and clinical studies.
Conclusion
It was determined that there is not compatibility between the gracilis tendons, the semitendinosus tendon and ATFL in women. It should be supported by biomechanical and clinical studies whether this incompatibility has a clinical effect or not.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This experimental animal study was approved and confirmed that all experiments were performed in accordance with relevant guidelines and regulations by the Acıbaden University’s Ethics Committee, Decision no: 2020-15/12.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.