
Abstract
Background:
Osteosarcoma is the most frequent bone cancer occurring in children and adolescents aged 10–20 years. Several prognostic factors have been identified by studies done at western centers. The aim of our study was to identify the prognostic factors in Tunisian patients in order to improve their management.
Methods:
We reviewed the data of localized limb osteosarcoma patients treated in Salah Azaïz Institute from January 1980 to December 2018. Patient’s treatment and survival variables were assessed. Patients received a neoadjuvant chemotherapy and underwent surgery in an expert center. They received afterward an adjuvant chemotherapy depending on the tumor necrosis assessed by Huvos.
Results:
Eighty-five patients were enrolled. Mean duration of follow-up was 30 months (range 1–297 months). Males were 1.6 times more frequent, median age was 17 (from 1 to 62 years). Conventional osteoblastic osteosarcoma was the most frequent histological subtype (77%). Median tumor size was 10 cm. Femoral location was the most frequent (60%). The overall average history of symptoms was 103 days (4 to 423 days). The 5-year overall-survival was 38% and the event free survival 32%. Tumor site, lactate dehydrogenase levels, high methotrexate levels at 24 h, clinical evaluation of the tumor perimeter, surgery type and delay of relapse were found to affect overall survival. Tumor site, Lactate dehydrogenase levels and clinical evaluation of the tumor perimeter affected the progression free survival.
Conclusion:
Demographic characteristics of Tunisian patients are mainly the same than worldwide. Femoral site, normal level of lactate dehydrogenase, a clinical response during neoadjuvant treatment, an R0 surgery, a delay of relapse over 2 years and Median H24 Methotrexate level superior to 4.4 µmol/l were associated with a better prognosis in our study.
Keywords
Introduction
Osteosarcoma is the most frequent bone cancer occurring in children and adolescents aged 10–20 years, but still is a rare pathology representing 0.2% of all cancers. 1 The seventies witnessed a revolution in osteosarcoma treatment by the adjunction of chemotherapy to the conventional surgery, thus, transforming its prognosis. 2 Since then, very little has been accomplished. Several prognostic factors have been identified, but the vast majority of studies have been conducted by western centers.
The aim of our study was to review data of patients treated in the largest cancer institute in Tunisia, The Salah Azaïz Institute, in order to identify the prognostic factors of our population, which would be valuable to improve the management of Tunisian patients.
Methods
We reviewed the data of patients with localized osteosarcoma of the extremities treated in Salah Azaïz Institute from January 1980 to December 2018. Patients with metastatic or axial disease were excluded from this study. Medical records were reviewed retrospectively to assess patients-related variables, treatment related variables and survival variables. In order to complete missing data, we reached patients by phone. Lacking Methotrexate levels in medical records were obtained via the National Center of Pharmacovigilance data.
For the sake of homogeneity and comparison with literature data, 80 days was taken as the threshold for long symptoms history. Lactate Dehydrogenase and Alkaline Phosphatase levels were measured before treatment onset. All patients included underwent a biopsy (core needle or surgical) and histologic classification was established according to the World Health Organization classification of 2013. Histopathologic slides of patients treated before 2013 were reviewed according to the new classification.
Preoperative chemotherapy was based on Rosen T8–T12 regimens (including Methotrexate, Cisplatin, Doxorubicin, Bleomycin, Dactinomycin, Cyclophosphamide), API/AI regimens (Cyclophosphamide, doxorubicin, ifosfamide) or etoposide ifosfamide Methotrexate regimen, depending on the age of the patient. Patients aged under 18 were treated with Methotrexate-based regimens . Patients older than 25 received API/AI chemotherapy. Intermediate aged patients (18–25 years) were treated with Methotrexate regimen for the majority.
The patients underwent a surgery (amputation or limb-sparing surgery) in an expert center and received afterward an adjuvant chemotherapy. The adjuvant chemotherapy drugs depended on the tumor necrosis rate assessed by Huvos. Ninety percent of tumor necrosis was the threshold for a good response.
Follow-up consisted of clinical examination and a yearly chest computed tomography (CT). It was scheduled every 3 months during the two first years, than every 6 months during the following 3 years and yearly for the five following years. Patients could consult only in case of need after 10 years of follow-up.
Statistical data were calculated using SPSS Version 20. Survival curves were calculated according to Kaplan Meier method and compared using log-rank test. Significance was set at P < 0.05.
Results
From January 1980 to December 2018, 85 patients with a localized peripheral osteosarcoma treated in the Salah Azaïz Institute were enrolled.
Tumor related variables
Of the 85 patients, 62% (53) were males and 38% (32) were females with a median age of 17 ± 9 years (from 1 to 62 years).
The osteoblastic conventional osteosarcoma was the most frequent histological subtype (66 cases, 77%), followed by the chondroblastic (8 cases, 9,4%), the anaplastic (4 cases, 4,7%), the telangiectatic (3 cases, 3,5%), the fibroblastic (2 cases, 2,4%) and the high-grade intramedullary tumors (2 cases, 2,4%).
Median tumor size was 10 cm. Of 85 patients, 51 were located in the distal femur (60%), 26 in the proximal tibia (30%) and 8 in the proximal humerus (10%). Among all age groups, the femoral location was the most frequent. No humeral location was recorded in patients older than 19 years old.
The distribution of histologic subtype by age and by tumor site are shown in Figures 1 and 2.

Distribution of histologic subtype by age.

Distribution of histologic subtype by tumor site.
At initial presentation, males had an average 97 days history of symptoms and girls 113 days. The overall average history of symptoms was 103 days ± 83 days (range, 4 days to 423 days).
Before treatment onset, average Lactate dehydrogenase levels were 475 IU/L.
Treatment
Time to start of treatment was 27 days (±15 days, range 3 days to 85 days) after the bone biopsy.
Of the 85 patients, 68 (80%) received a methotrexate-based chemotherapy according to Rosen protocols T8–T12 (median age 17 years) and 17 (20%) received other chemotherapy regimens (median age 24 years). Median treatment time duration was 12 weeks. Patients treated with Methotrexate regimens received a median number of 7 ± 2 cures, while patients treated with Adriamycin-Cisplatinum-Ifosfamide received 3 ± 1 cures.
The median dose of Methotrexate was 12 g/m2. Of the 68 patients treated by Methotrexate, the drug levels have been measured in 21 of them, as before the 2000’s, Methotrexate levels were not measured in Tunisia. The median methotrexate levels at 24 h, 48 h and 72 h after the infusion are summarized in Table 1.
Median methotrexate levels after 24 h, 48 h and 72 of the infusion.

After neoadjuvant treatment, 33% of patients responded to the treatment, 27% were stable and 27% progressed. Data was missing for 13%. Seventy patients out of 85 underwent surgery (82% of patients). The 15 remaining patients either progressed or were lost to follow-up.
Restaging was done prior to surgery in order to choose the type of intervention. Surgery was performed after a median time of 31 days (range, 6 days to 380 days) after the neoadjuvant treatment. Patients with neurovascular structures involvement or with insufficient skin coverage possibilities were treated with an amputation. All other patients had a limb-sparing surgery. Thirty-four patients (40%) underwent limb-salvage treatment and 31 (36.5%) had an amputation. Seventy-five percent of them (54 patients) had an R0 oncologic surgery. We could not find the data relative to the type of surgery (limb-salvage or amputation) of five patients. Patients with R1 and R2 surgery did not undergo any further surgery.
The assessment of the histologic response was available for 59 patients. Of 59 patients, 13 patients (22%) were good responders while 46 patients (78%) didn’t achieve a good response. The median tumor necrosis rate was 70%.
Adjuvant chemotherapy was resumed after a median delay of 41 days (range, 5 days to 146 days) for 76 patients. 9 patients were lost to follow-up.
Overall survival and progression free survival
The 5-year overall survival (OS) was 38% and the Progression free survival (PFS) 32%. At 3years, the overall survival was 49% and the event free survival 37%. The overall survival curve reached a plateau at 60 months (5 years) (Figures 3 –6).

Progression free survival.
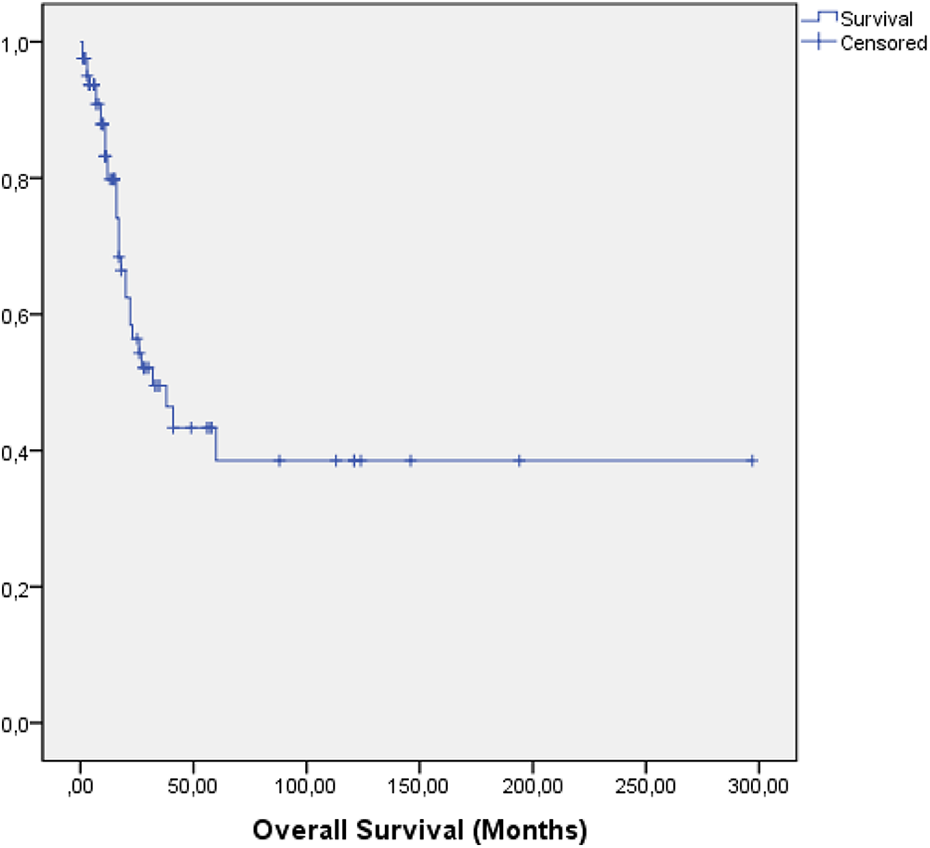
Overall survival.

Overall survival depending on histologic response.

Disease free progression depending on histologic response.
At the last follow-up, 34 patients were alive and 33 died. Eighteen patients were lost to follow-up. The prognostic factors are reported in Table 2.
Prognostic factors influencing overall survival.

* Missing data.
On univariate analysis, tumor site, lactate dehydrogenase levels, Methotrexate levels at 24 h, clinical evaluation of the tumor perimeter, surgery type and delay of relapse were found to affect overall survival. Tumor site, Lactate dehydrogenase levels and clinical evaluation of the tumor perimeter affected the progression free survival in univariate analysis (Table 3).
Prognostic factors influencing progression free survival.

Of 85 patients, 30 patients (35%) relapsed. Nineteen patients (63%) developed distant metastases, 11 patients had a local recurrence (37%). Among the latter patients, 6 (55%) have had a limb-salvage surgery and 5 (45%) have had an amputation.
Discussion
Demographic characteristics of our patients were similar to those in other series, particularly Chinese series. Males were affected 1.6 times more than females (1.35 according to the Surveillance, Epidemiology and End Results Program (SEER) study 3 ). The peak of incidence, between 12 and 21 years, and the unimodal distribution of age were consistent with those in the Chinese population. 4 The absence of the commonly observed second peak in western series may be explained by the rarity of the Paget disease in Tunisia and by the absence of axial tumors in our study.
The femoral location was the most frequent (60%) followed by the tibial (30%) and the humeral location (10%). Even though the order was the same, frequency by tumor site was higher in our study compared to Ottaviani et al. which reported 42% and 19% of the tumors in femur and tibia respectively. 1 Seventy-seven percent of cases were conventional osteosarcomas. These data were analogous to the literature where the conventional subtype counts for 70–80% of cases. 5
Five-year overall survival was 38%, which is inferior to the data documented in other western series 6,7 (about 65.3% in Bielack’s series) but somehow similar to Indian series (49%). 8 These results may be explained by the large tumor size in both populations (median size of the tumor was 10 cm in Tunisian patients). Large tumor size has been reported as a poor prognostic factor previously. 9 In addition to that, chemotherapy resumption delays after surgery (41 days in our study) were to blame. These delays were higher than the threshold of 21 days found to be associated with an increased risk of death in Imran et al. study. 10
The low rate of tumor necrosis (22% of good responders in contrast with 55% in Bielack et al. study) 7 may also have impacted the patients survival. Both factors may be due to the long history of symptoms until diagnosis, meaning a higher delay of chemotherapy initiation 7 (103 days ± 83 days). Methotrexate levels in our series were similar to Saeters results (4.4 µmol/l vs 2.7 µmol/l at 24 h and 0.24 µmol/l vs 0.35 µmol/l at 48 h). 11
Several features including age, tumor size, axial tumors, surgical margins, histologic response and delay of relapse have been reported as prognostic factors. 9,12,13 Femoral site, normal levels of lactate dehydrogenase, a clinical response during neoadjuvant treatment, an R0 surgery, a delay of relapse over 2 years and Median H24 Methotrexate level superior to 4.4 µmol/l were associated with a better prognosis in our study.
Regarding the low response rate to neoadjuvant chemotherapy in our population, we considered dose escalation to enhance the oncologic outcomes. In fact, the question of Methotrexate dose-intensity remains unsolved. Taking into account that the histologic response has clearly been demonstrated to be linked to the prognosis, some authors tried to intensify the neoadjuvant treatment to reach better outcomes. Graf et al. identified methotrexate peak concentration at 1000 µmol/l as the efficiency threshold. 14 Saeter et al. demonstrated that Huvos I patients had lower H24 and H48 methotrexate levels, 11 Delepine et al. adapted chemotherapy doses to the excretory potential of each patient 15 increasing thus the tumor necrosis, and Bacci identified the 700 µmol/l Methotrexate level to be linked to a higher complete tumor necrosis rate. 16 On the other hand, Eselgrim et al. did not found any statistical relation between 200 days dose-intensity of chemotherapy and survival outcome, nor did the European Osteosarcoma Intergroup or Kushnir et al. 17 –19 These results suggest that patient prognosis is not threatened by inevitable treatments delays. Our patients received neoadjuvant chemotherapy in due time (median duration time of 12 weeks) and mostly accomplished all their scheduled cures (median number of 7 ± 2 cures for methotrexate-treated patients and 3 ± 1 for Adriamycin-Cisplatinum-Ifosfamide-treated patients).
In our study, we found that patients with H24 Methotrexate levels over 4.4 µmol/l had a better prognosis on survival. This may reinforce the necessity of dose-intensity in our population. If this hypothesis is confirmed by prospective studies, it will support the results of the mentioned studies in favor of dose-intensity chemotherapy.
Recurrence rate is still high with 35% of patients relapsed. Local recurrence rate (12% of all patients) is similar to results of the series of Puri and of Grimer 8,20 and is most probably due to adequate oncologic resection margins.
As demonstrated by various authors, limb-sparing treatment in our patients was linked to a slightly higher recurrence rate.
Femoral location, normal levels of lactate dehydrogenase, clinical response during neoadjuvant treatment were associated with lower recurrence in our study.
This study has multiple limitations: retrospective single institute study, a small number of patients and missing or insufficient data or dosages. Despite our efforts to reach patients and review medical records, missing data constituted a significant challenge because of the long period of study. On the other hand, it is the largest series of Tunisian patients presenting with localized osteosarcoma offering valuable information about our population and our oncologic outcomes.
Conclusion
In conclusion, this study shows the demographic characteristics of Tunisian localized osteosarcoma patients that are mainly the same than worldwide. Diagnosis is still delayed in our country leading to increased tumor size and possibly decreased tumor necrosis.
Femoral site, normal levels of lactate dehydrogenase, a clinical response during neoadjuvant treatment, an R0 surgery, a delay of relapse over 2 years and Median H24 Methotrexate level superior to 4.4 µmol/l were associated with a better prognosis in our study. Despite our efforts, some data are still missing in this retrospective series of 30 years. Further prospective studies are needed to affirm the utility of dose intensification of chemotherapy as a way to improve oncologic outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.