
Abstract
Purpose:
Defect of Achilles tendon and overlying soft tissue remains a surgical challenge due to its insufficient blood supply and high requirement of function. This study aims to report the clinical efficacy of the composite sural neurocutaneous composite flap with gastrocnemius tendon on the complicated defect of Achilles region.
Methods:
Seven cases of defects of Achilles tendon and overlying soft tissue were reconstructed by the composite sural neurocutaneous composite flaps with gastrocnemius tendons. It is important to keep the connection between gastrocnemius tendon and deep fascia of the composite flap during operation. The smallest and the largest areas of transferred skin flaps were 7.5 cm × 4.5 cm and 11 cm × 10 cm respectively. The size of gastrocnemius tendon ranged from 5 cm × 3 cm to 9 cm × 4 cm. Patients was evaluated by using the Arner-Lindholm scale at the last follow-up.
Results:
Six flaps survived completely with no complication. One flap developed wound dehiscence and went on to heal by daily dressing. With 12–60 months follow-up, all patients gained satisfactory appearance and function of ankle, without tendon re-rupture or recurrent infection. Based on Arner-Lindholm scale, six cases were noted to be excellent and one was good.
Conclusion:
The composite sural neurocutaneous flap with gastrocnemius tendon is a viable and practical method to salvage Achilles tendon defect and overlying soft tissue coverage, with minimal adhesion and satisfactory function.
Introduction
Defects of the Achilles tendon and overlying soft tissue are not infrequent, and the reconstruction of the complex defects is still Challenging. 1,2 Bicycle and motorcycle wheel spoke injury often result in the complex defect at the Achilles tendon region, especially in children. 3,4 The Achilles tendon is the most easily ruptured tendon, and surgery is a commended solution. 5 –7 Wound complications are common following the open Achilles tendon operation due to limited vascularity and insufficient soft tissue. 8,9 Besides, systemic illness and iatrogenic complications following steroid infiltration are also causative factors. 1 Infection, soft tissue necrosis and exposure of Achilles tendon usually result in superficial erosion or necrosis of the tendon, which in turn lead to partial or complete defect of the tendon after debridement.
Repairing the combined loss of Achilles tendon and overlying integument must maintain the stability and durability of skin and guarantee enough strength and mobility of Achilles tendon. There are many reconstructive strategies reported for this area, such as anterolateral thigh flap, 2 temporoparietal fascial flap, 10 reverse sural artery flap 11 and propeller flaps 12,13 based on posterior tibial artery perforator or peroneal artery perforator. Each approach has its own drawbacks and the adequate treatment is still controversial. Since the anatomy and clinical application of the sural neurocutaneous flap were reported by Masquelet et al. in 1992, 14 this flap has gradually become a mainstream for repairing soft tissue defects in the lower leg, foot and ankle. 15 –17 The reversal sural flap has advantages of simple process, no need of vascular anastomosis, reliable blood supply and high survival rate. 18,19 This study aims to describe the use of the composite sural neurocutaneous flap with gastrocnemius tendon for simultaneously repairing the combined loss of Achilles tendon and regional soft tissues.
Patients and methods
Over a period of 3 years (October of 2014 to September of 2017), seven composite sural neurocutaneous flaps with gastrocnemius tendons were applied to reconstruct the complicated defects of Achilles tendon and soft tissue surrounding the area. This retrospective study included four males and three females with an average age of 23.7 years (range, 7 to 44 years), who suffered from motorcycle spoke injury (n = 3), traffic accident (n = 2), cut injury (n = 1) and sports injury (n = 1). All patients had previously undergone at least one operation for the defects of Achilles tendon region before this flap surgery, and the average time elapsed from injury to the reconstruction procedure was 33.3 days (range, 17 to 45 days).
The affected Achilles tendons presented complete rupture in one case and partial loss in six cases after debridement. The complete ruptured tendon was sutured end to end at the plantarflexion position of the ankle and had a 1-cm gap remained in the middle section. In this study, partial loss of each Achilles tendon was more than half of the tendon and was further divided into width loss and thickness loss. The mean length of lesion was 5.0 cm (range 4 to 6 cm) in width loss cases (n = 3), and 2.3 cm (range, 2 to 3 cm) in thickness loss cases (n = 3). All patients understood the information about the surgical procedure and signed informed consent. The patient demographics and defect characters were displayed in Table 1.
Patient demographics and defect characters.

M: male; F: female.
a The type and length of the Achilles tendon defect were assessed at the neutral position of the ankle after debridement.
The dimension of the sural flaps ranged from 33.75 to 110 cm2 (mean, 59.3 cm2), and the size of gastrocnemius tendon strips ranged from 15 to 36 cm2 (mean, 21.9 cm2). The fascia pedicle of the flaps, with a 2-cm-wide skin strip overlaying it, was 3 to 9 cm in length and 3 to 4 cm in width. The pivot point of the flaps located 6 to 11 cm proximal to the tip of the lateral malleolus. The details of surgical information were showed in Table 2.
Surgical information and clinical outcomes.

Composite flap: the composite sural neurocutaneous flaps with gastrocnemius tendons; PBG: peroneus brevis graft; PF: plantar flexion; DF: dorsiflexion.
a The pivot point refers to its distance proximal to the tip of the lateral malleolus.
Surgical technique
Under continuous epidural or general anesthesia, the patients underwent the surgery in the lateral decubitus position with the affected limb lying above. A tourniquet was routinely used to prevent bleeding during the procedure. After debriding the infected, erosional and necrotic tissues of Achilles tendon and soft tissue, a paper pattern was cut out in line with the defect shape and the location and size of Achilles tendon defect was drawn on the pattern. The design of the sural neurocutaneous flap has been described detailly in the previous literature (Figure 1(a)). 20 The incisional border of the gastrocnemius tendon was drawn correspondingly at the flap according to the pattern. The tendon strip was 3 to 4 cm in width generally and 1 to 2 cm longer than each end of the Achilles tendon defect in length.
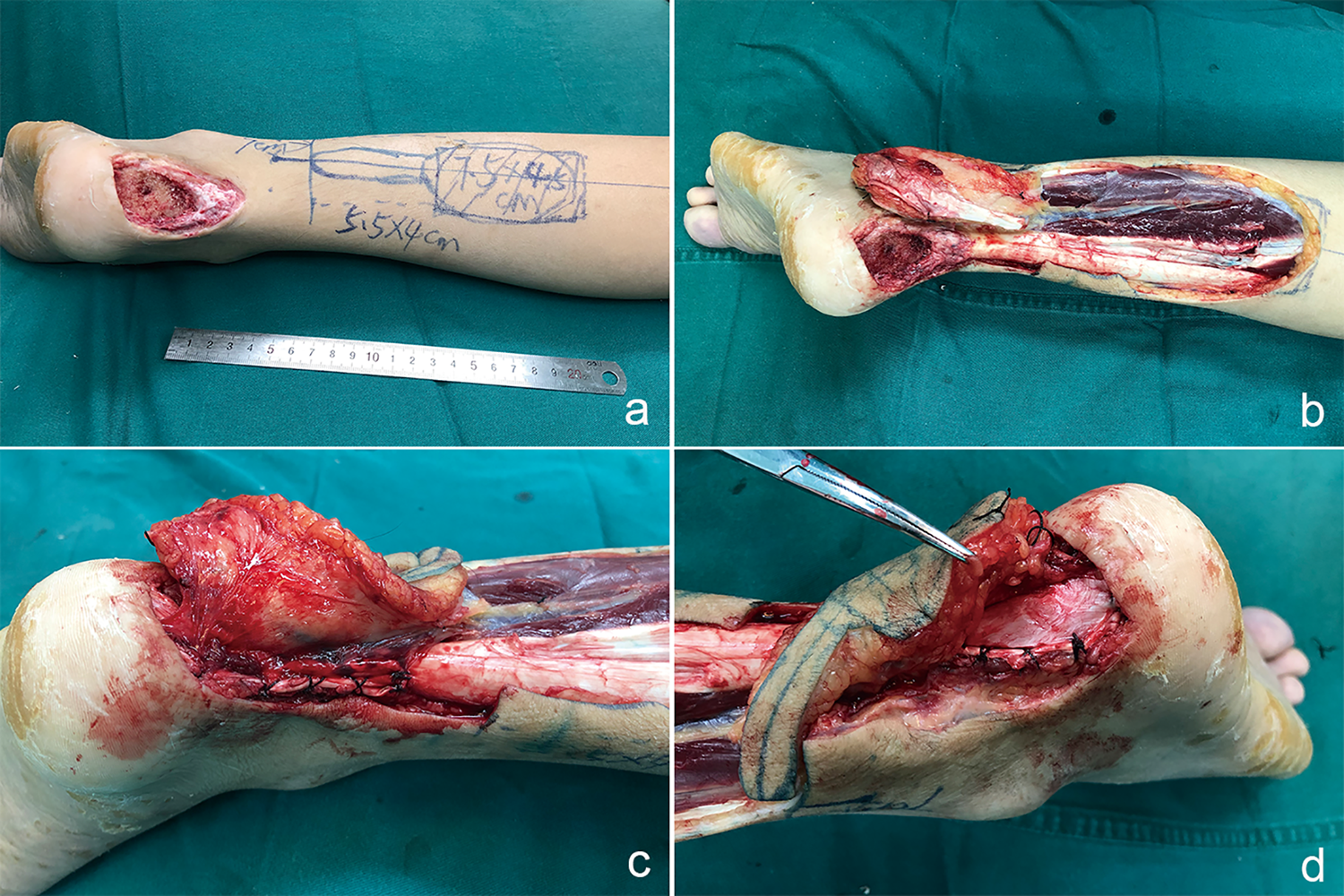
Photographs of surgical procedure of composite sural neurocutaneous flap with gastrocnemius tendon. Design of flap and tendon strip (a). Harvested composite flap (b). Gastrocnemius tendon covered Achilles tendon defect and was sutured with residual tendon medially and laterally (c and d).
The composite sural neurocutaneous flap with gastrocnemius tendon was harvested by the anterograde–retrograde approach, 20 that the peroneal artery perforator nearby the pivot point was explored and identified firstly then the flap was elevated retrogradely below the deep fascia plane. When reaching the designed tendon area, the gastrocnemius tendon was incised as designed in the space between the gastrocnemius tendon and soleus tendon. This space was relatively loose in the middle and upper sections of Achilles tendon and could be bluntly separated, and in the lower section of Achilles tendon it was unobvious and required a sharp separation. Attention was paid to protecting the connection between the gastrocnemius tendon and the deep fascia to prevent the tendon strip separating from the flap. Temporarily suture the tendon and skin when necessary. Dissection was stopped until the composite flap and its fascia pedicle were raised up just above the identified peroneal perforator (Figure 1(b)). And transpose the flap to the defect through the incised path.
The Achilles tendon defects were directly repaired with the gastrocnemius tendon by covering and suturing with the tendon defect in three thickness loss cases and two width loss cases (Figure 1(c) and (d)). Peroneus brevis graft was applied in a width loss case and a complete rupture case after the Achilles tendon was end-to-end anastomosis in the plantar flexion position. Then the sutured area was covered with the gastrocnemius tendon to augment the reconstruction. The flap was sutured with the defect without tension.
The donor site of the gastrocnemius tendons was sutured with absorbable sutures to rebuild the integrity. The donor site of the flaps was closed by direct suture in four cases and being resurfaced with full-thickness skin grafting in three cases after appropriately narrowing down.
Postoperative, the affected limb was externally fixed for 3 weeks by a long plaster with 45° of knee flexion and 30° of ankle plantar flexion and immobilized by a short plaster at 30° of ankle plantar flexion for another 3 weeks. After removing the plaster, patients were instructed to gradually begin flexion and extension of ankle. Eight weeks after surgery, the patient was allowed to begin slow weight-bearing progression. Full weight bearing was allowed no earlier than 12 weeks after the reconstruction surgery. During the follow-up, physical examination of all patients was performed, and the rating of the clinical results was evaluated using the Arner-Lindholm scale. 21 The details of Arner-Lindholm scale were showed in Table 3.
Details of Arner-Lindholm scale.

a The evaluation indexes are estimated comparing to the unaffected side.
Results
Six flaps survived completely with no complication. Minor wound dehiscence occurred in the margin of one flap, and the residual wound continued to heal with daily dressing without additional surgery. The donor sites in all seven patients healed uneventfully. Mean follow-up was 35 months (range, 12 to 60 months). No re-rupture of the Achilles tendon or recrudescent infection was observed. All patients gained satisficed appearance of flap. The patients had no difficulty walking in shoes and the gait was normal. The ankle activity function was satisfactory (Figures 2 and 3). The ankle mobility of the affected limb decreased no more than 5° in dorsiflexion or plantar flexion compared to the unaffected limb. Only one patient had calf circumference decreased 2 cm and felt weak to stand on tiptoe with slightly decreased myodynamia. In this series, the clinical outcomes presented excellent in six cases and good in one case (Table 2).

Patient 1 presented with left Achilles tendon exposure and overlying soft tissue defect. Preoperative appearance (a). Postoperative appearance (b) and functional result (c and d) at 50 months follow-up.

Patient 3 suffered from soft tissue infection after tenorrhaphy. Preoperative appearance (a). Interoperative photograph of flap design (b). Tiptoe ability of operative leg at 22 months follow-up (c) and 60 months follow-up (d).
Discussion
As the thickest and strongest tendon in the body, Achille tendon plays an essential role in daily activities and sport. This tendon is a confluence of gastrocnemius tendon and soleus tendon at the middle of the lower leg. The combination is loose in the proximal and middle Achilles tendon, which is easy to separate, and tight in the distal part (Figure 4). The entire tendon is surrounded by delicate connective tissues, which is an extension of the triceps surae aponeurosis, and then covered with paratenon. 22 On the dorsal superficial surface of the Achilles tendon, there are four to eight lubricating layers between deep fascia and the tendon. Each layer has independent nutritional vessels and can slide past each other to adapt to dorsiflexion and plantar flexion of ankle. The blood supply of Achilles tendon and overlying integument is provided by the posterior tibial artery medially and the peroneal artery laterally. 23 The midsection of Achilles tendon, supplied by the peroneal artery, is the thinnest segment with comparatively hypovascular. 23 The posterior zone directly over the Achilles tendon has a poor vascularized integument. 8

Photograph of dissected Achilles tendon. Gastrocnemius tendon and soleus tendon combined loosely in middle and proximal of Achilles tendon and tightly in distal Achilles tendon.
The distally based sural neurocutaneous flap is supplied by the septocutaneous perforators of the lower peroneal artery. 24 Anatomical observation was done on two fresh amputated lower leg specimens, injected with 20 ml of methylene blue solution through the peroneal artery at 18 cm above the lateral malleolus. It showed that the peroneal perforator sent branches to Achilles tendon and overlying skin, the posterolateral skin of the middle and distal lower leg and the dorsal side of Achilles tendon were stained, and there were small communicating branches between the dorsal vascular network of the tendon and the deep fascial vascular network (Figure 5). These results suggested that the perforator of the lower peroneal artery could provide blood supply to the gastrocnemius tendon and the skin surrounding this area. In this series, all flaps survived without additional surgery and minor wound dehiscence occurred in only one patient with diabetes mellitus.
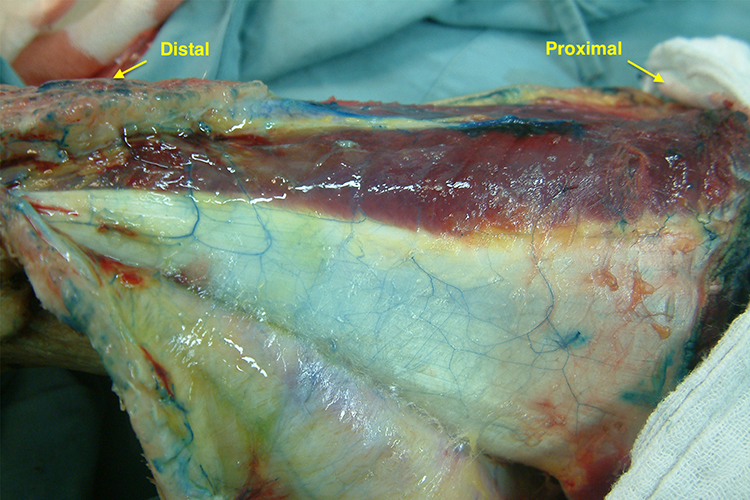
Lower leg specimen injected with methylene blue solution. Branches of peroneal perforator reach spread dorsal vascular network of Achilles tendon, which connects with deep fascial vascular network by small communicating vessel.
The complicated defects of Achilles tendon and overlying region are common, mainly caused by systemic illness, trauma and iatrogenic complications. 1,4 The common complications of open operative treatment for Achilles tendon rupture are re-ruptured and infection (including superficial infection and deep infection). 7,25 The incidence of deep infection is 1% to 5%, while the rate of superficial infection is up to 20% resulting in delayed wound healing. 5,9,26 The Achilles tendon needs enough strength and mobility for weight-bearing and activity. 27,28 Simultaneously, the posterior heel requires a durable and sensitive coverage for repeated friction by footwear. The complex defect in Achilles region poses a surgical challenge to surgeons to achieve both requirements.
Many one-stage reconstructive strategies have been reported for the Achilles region and can be divided into four types, as free flap or local pedicled flap in combination with vascularized or no vascularized fascia, tendon or allograft tendon. 29 The composite anterolateral thigh flap with the fascia lata has been widely applied in Achilles region, especially in massive deficit. 30 –32 There are some unignorable drawbacks including vascular crisis, secondary thinning procedures for bulky flap and deficit of quadriceps femoris muscle contraction forces. 2,31 The radial forearm flap with palmaris longus tendon provides thin and pliable integument and long tendon, while it has significant donor-site morbidity and is better suited for small rather than massive defects. 33,34 Dobke et al. 35 reported satisfactory outcomes of the extended temporoparietal fasciagaleal flap for a long-term follow-up. Wurzer et al. 10 described the use of free temporoparietal fascial flap with a plantaris transposition and obtained aesthetical and functional satisfaction. However, this fascial flap with limited capacity requires complicate microsurgical technique and an overlap of skin graft, and lack of tendon sliding layers as well as free muscle flaps. 10,36 Step-advanced rectangular flap 37 and bi-pedicled flap 38 were easy and simple method for small defects in the Achilles area. Posterior tibial artery perforator flap, reverse sural flap and propeller flap have been reported as fast and effective procedures. 12,13,29,39
The composite sural neurocutaneous flap with gastrocnemius tendon is capable of reconstructing of the Achilles tendon and regional soft tissue defects simultaneously. This surgical approach shows reliable survival rate of the flap with technical simplicity and no need of vascular anastomosis. 40 All flaps in the present study survived. Postoperative adhesion is reduced by retaining the lubricating layers between the deep fascia and tendon strip of the flap, which promotes the motional rehabilitation of the Achilles tendon. In this study, all patients gained normal-like ankle function, and the mobility of operated side was restricted no more than 5° either in dorsiflexion or plantar flexion comparing with the healthy side. Besides, the transposed gastrocnemius tendon is wrapped with vascularized fascia attaching to the sural neurocutaneous flap, thus the tendon strip has well blood supply. The vascularized tendon strip facilitates the healing of the suture areas of the affected Achilles tendon, enhances the tensile strength of the reconstructed tendon and contributes to the control of the local infection. 41 –44 In this series, no re-ruptured Achilles tendon or recurrent infection was noticed. However, the gastrocnemius tendon is relatively thinner than the Achilles tendon, and its tensile strength is not enough. It needs further observation to simply apply the gastrocnemius tendon to repairing the complete rupture of the Achilles tendon.
The composite sural neurocutaneous flap with gastrocnemius tendon is suitable for the repair of the partial Achilles tendon defect and the overlying soft tissue defect caused by wound infection and tendon exposure. The gastrocnemius tendon of the composite flap has advantages of repairing partial tendon defect, controlling infection, increasing the strength against tendon tension and decreasing the adhesion. When the strength is insufficient with the graft of peroneus brevis tendon, plantar tendon, or hamstring tendon to reconstruct the Achilles tendon, the gastrocnemius tendon strip is applied to cover the reconstructed area to reinforce the suture and provide lubricating layers for tendon sliding. 45 –47 It is consistent to suture the Achilles tendon with a tendon gap smaller than 3 cm directly by end-to-end anastomosis. 7,48 We recommend the composite sural flap with vascularized gastrocnemius tendon to overlap the sutured region for an augmented connection, gliding plane and durable coverage.
In this study, the composite sural neurocutaneous flap is a perforator-plus 49 sural flap rather than a pedicle sural flap, as its pivot point is nearby the site of distal peroneal perforator (Figure 6). With specifically identifying and protecting the distal peroneal perforator to the flap, the composite sural flap has dual blood supply from the dominant perforator and the random supply from its base. 49 It is a reliable surgical management of lower limb injuries. 40 However, the perforator-plus sural flap has a similar rotation arc as the pedicle sural flap, which causes a bloated appearance of the fascia pedicle and restricts its ability in the reconstructing the extensive defect. If the donor area cannot be closed by direct suture, skin graft will be used to resurface the donor area, which will cause significant scar and maybe slightly affect the motor function.
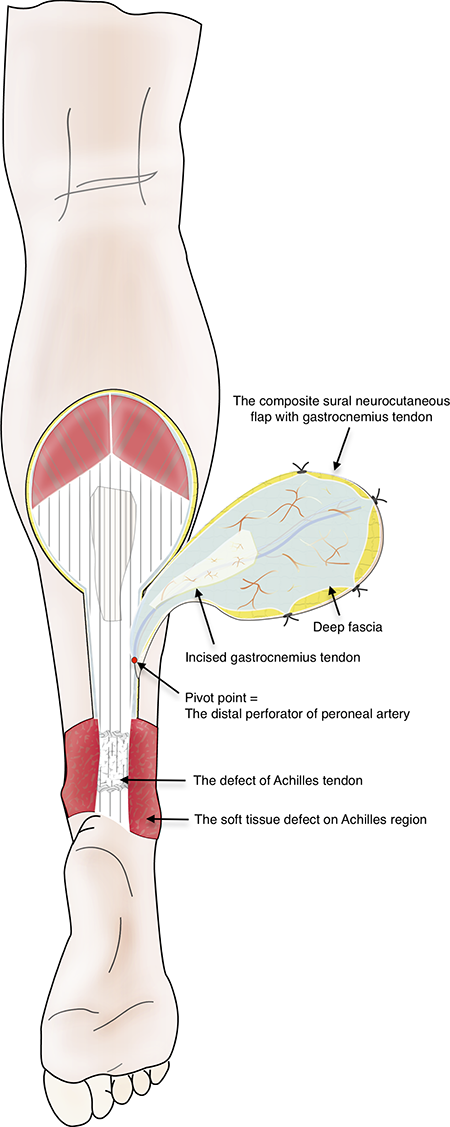
The schematic of composite sural neurocutaneous flap with gastrocnemius tendon. The composite sural flap is elevated below the deep fascia plane and connected with the incised gastrocnemius tendon by small communicating vessels. The pivot point is near by an identified distal perforator of peroneal artery. The composite sural flap rotates at the pivot point and reconstructs the defect of Achilles tendon and the soft tissue defect on Achilles region.
This study is limited for its retrospective design, small size of patients, lack of controlled group and relatively short follow-up. The included patients were relatively young and most of them without comorbidity.
Conclusion
The composite sural neurocutaneous flap with gastrocnemius tendon is an effective and economical method for reconstruction of the combined defects of Achilles tendon and overlying soft tissue. This surgical technique has advantages of operative simplicity, minimal adhesion and satisfactory function, especially in partial rupture and augment of completely rupture of Achilles tendon.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (no. 81672188) and Health and Family Planning Commission of Hunan Province (no. B20180313).