
Abstract
Introduction:
Patient-reported outcomes recently have been used to assess treatment outcomes. The Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) is a particularly convenient and useful tools. However, data on the normative values of Japanese population are lacking, so the present study was conducted to gather this information.
Methods:
We assessed 1098 volunteers over 18 years of age (363 men and 735 women, average 50 years old) who had not received upper limb treatment in a medical facility. These participants included our institution’s staff, their family members, and the participants in the group meetings held by institution’s staff. Their occupations were also examined. We divided occupations into nonmanual and manual labor. These factors of the participants were then analyzed to clarify which (if any) influenced the QuickDASH.
Results:
Valid answers were obtained from 961 subjects (87.5%). The median score was 2 (mean: 4.8) in the overall population, 0 (mean: 2.6) in men, and 2.5 (mean: 6.0) in women. The scores increased with age and were higher in women than in men. There were no significant differences by manual labor. Female sex and older age were identified as factors that influenced the QuickDASH score in the multiple regression analysis. There were high correlations among QuickDASH, work and sports/music scores.
Conclusions:
The present study provided QuickDASH scores for Japanese volunteers who had not received upper limb treatment in a medical facility. The scores were associated with older age and female sex. This study helps us to know the degree of potential upper limb impairment in the general population, and will help in populational strategies as primary and secondary preventive medicine for upper limb-related diseases.
Introduction
Patient-reported outcomes recently have been used to assess treatment outcomes as well as clinician-reported outcomes, such as range of motion, muscle strength, or radiographic outcomes. Several tools have been developed to evaluate the function of the upper extremities, e.g. Disabilities of the Arm, Shoulder, and Hand (DASH), QuickDASH, Patient-Rated Wrist Evaluation (PRWE), and Hand20. 1 –4 These tools have no cut-off values and are appropriate for evaluating treatment effects and changes over time in the same patient. The QuickDASH score represents the disability/symptom score, which includes 11 items from the original DASH’s 30 questions. In addition, both the answer time and the evaluation time are shorter than with DASH. These are merits for both patients and evaluators. The QuickDASH has been reported to have a high correlation with the DASH and is therefore convenient and useful for evaluating PROs of the upper extremities. 2,5,6 There is no set age limit for DASH and QuickDASH, and the general guidelines recommend it be performed for patients 18 to 65 years of age. 7 However, Aasheim and Finsen reported normative values in the general population aged 20 to ≥80. 5
Previous reports on DASH in the general population clarified that the score increased with age and was higher in women than in men. 5,8,9 In addition, among subjects under 65 years old, manual laborers had higher scores than nonmanual laborers. 8,9 Although Aasheim and Finsen reported the QuickDASH scores in a general Norwegian population, data on general Japanese population are lacking. The purpose of the present study is to investigate the QuickDASH scores among Japanese subjects over 18 years of age to examine the factors that influence the QuickDASH score and to understand the degree of potential upper limb impairment in the general population.
Methods
We assessed the QuickDASH Japanese version (QuickDASH-JSSH), 6 using volunteers including our institution’s staff, their family members, and the participants in the group meetings held by our institution’s staff. The study was approved by the Institutional Review Board, and informed consent was obtained from all of the subjects. Between October and December in 2019, we distributed the QuickDASH forms to 1133 subjects. The subjects wrote down their age, sex, dominant hand, and QuickDASH answers. In addition, we asked them about their occupations, and then the forms were collected. Subjects who failed to fill out their age or sex (n = 18), who were <18 years old (n = 8), or who were seeing a medical facility for a condition related to an upper extremity disorder (rheumatoid arthritis [n = 3], upper limb paralysis [n = 3], or current treatment for upper limb injury [n = 3]) were excluded from this study. The remaining 1098 subjects who were not receiving upper limb treatment in a medical facility at that time were therefore assessed in the present study, and those for whom a valid QuickDASH score was obtained additionally had their optional work score and sports/music score measured. A valid QuickDASH score was obtained in 961 subjects (87.5%), a valid work score in 779 subjects (70.9%), and a valid sports/music score in 285 subjects (26.0%) (Figure 1).
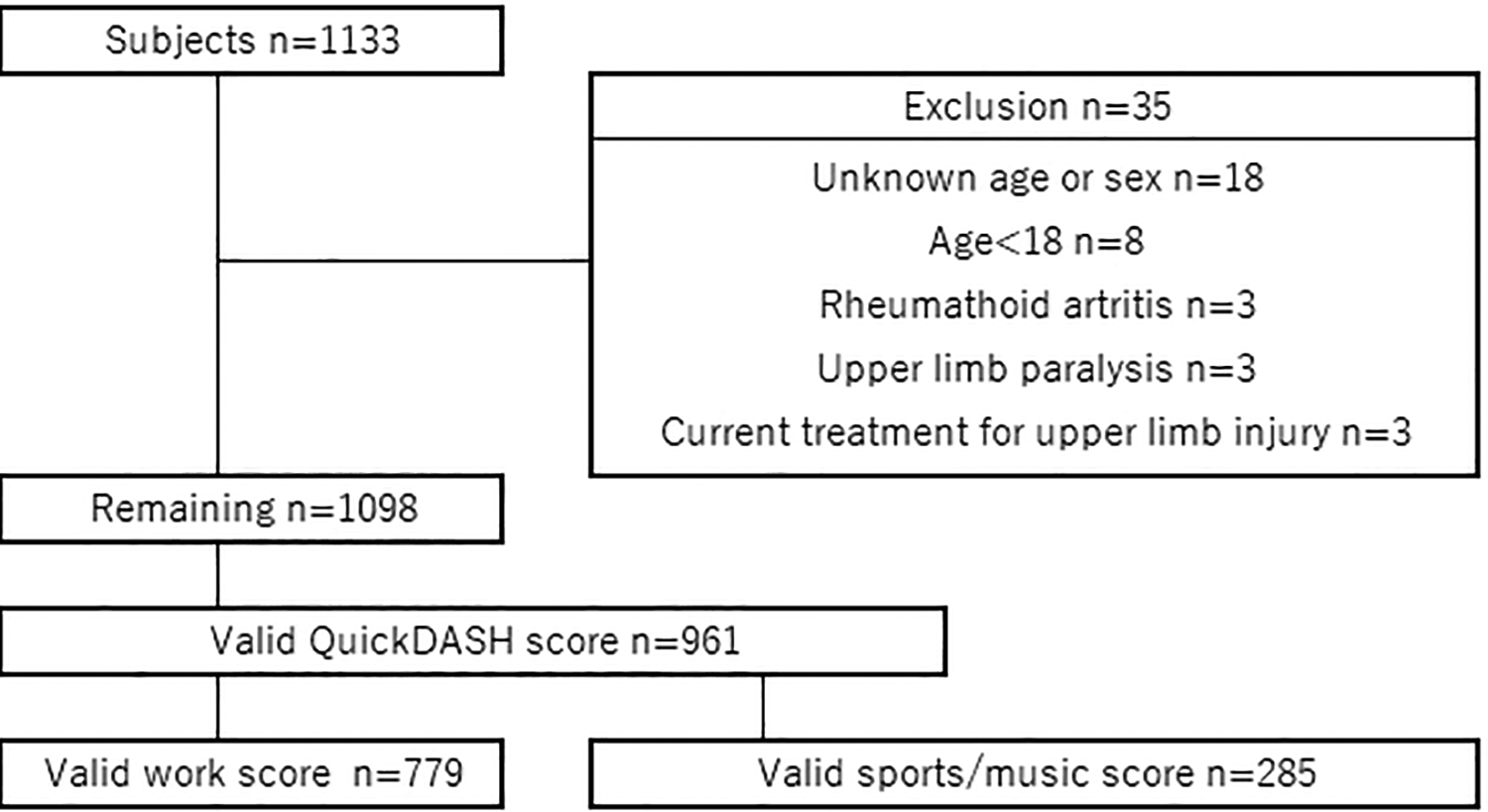
Participants flowchart.
With respect to occupations, blue-collar workers were basically defined as manual laborers and white-collar workers as nonmanual laborers. However, people who were involved in occupations that were judged to involve a high use and load on the upper limbs were arbitrarily defined as manual laborers, and vice versa. Nurses, for example, were defined as manual laborers, as they were in Klum et al.’s study.
9
Manual laborer: nurse (including nursing assistant), caregiver, physical therapist, occupational therapist, ambulance crew, fireman, farmer (including vegetable gardener), gardener, forestry worker, builder, transporter, delivery person, manufacturing industry worker, mechanic, electrician, welding worker, cleaner, cook, barber, seamstress, rafting guide.
Nonmanual laborer: doctor, dentist, dental hygienist, medical engineer, system engineer, laboratory technician, radiological technician, pharmacist, dietician, service industry, teacher, clerk, office worker, water analyst, driver, guard, houseworker, not working.
QuickDASH scores were compared between men and women across five generations of 18–29, 30–49, 50–64, 65–74, and ≥75 years old. Scores were also compared among five generations by sex. Correlations among the QuickDASH score, work score, and sports/music score were calculated. Regarding manual labor, the QuickDASH scores and work scores were compared between nonmanual and manual laborers for 18–64 or ≥65 years old, divided by sex to avoid any influence. In addition, to detect which factor (if any) affected the QuickDASH, the influence of age, sex, hand dominancy, or manual labor on the QuickDASH scores was analyzed.
Statistical analyses
Regarding statistical analyses, the Shapiro-Wilk test was used to assess the normality of distributions. As the data were not normally distributed, the Mann-Whitney U-test was used to compare two groups and the Kruskal-Wallis analysis and Bonferroni’s correction were used to compare the values among five generations. Spearman’s rank correlation was calculated to examine the correlations among the QuickDASH, work, and sport/music scores. Correlations were characterized as low (rs = 0.10–0.29), medium (rs = 0.30–0.49), or high (rs = 0.50–1.00). 10 A multiple regression analysis was conducted to detect the subjects’ factors that affected the QuickDASH score. P values of <0.05 were considered to indicate statistical significance. This was a cross-sectional study and all subjects collected over a period of time were included in this study. Thus, the sample size was not calculated.
Results
The 961 subjects included 327 men and 634 women, with an average age of 49.1 ± 17.7 years old. Their demographics and the breakdown of the manual laborers are shown in Tables 1 and 2, respectively. Nurses and caregivers were the most common manual laborers in both sexes.
Demographics and characteristics of all subjects (n = 961).

Breakdown of manual laborers.a

a Values are the number of subjects.
Table 3 and Figure 2 shows the QuickDASH score. The median [25th percentile, 75th percentile] score of all subjects was 2.3 [0, 6.8]; the mean score was 4.8. The mean scores increased with age in both sexes. Women had significantly higher QuickDASH scores than men in age groups under 75 years of age and total subjects. The age groups of 65–74 and 75+ had significantly higher scores than those of 18–29 and 30–49 in men, and the age groups of 50–64, 65–74 and 75+ had significantly higher scores than those of 18–29 and 30–49 in women.
Comparison of the QuickDASH scores (n = 961).a
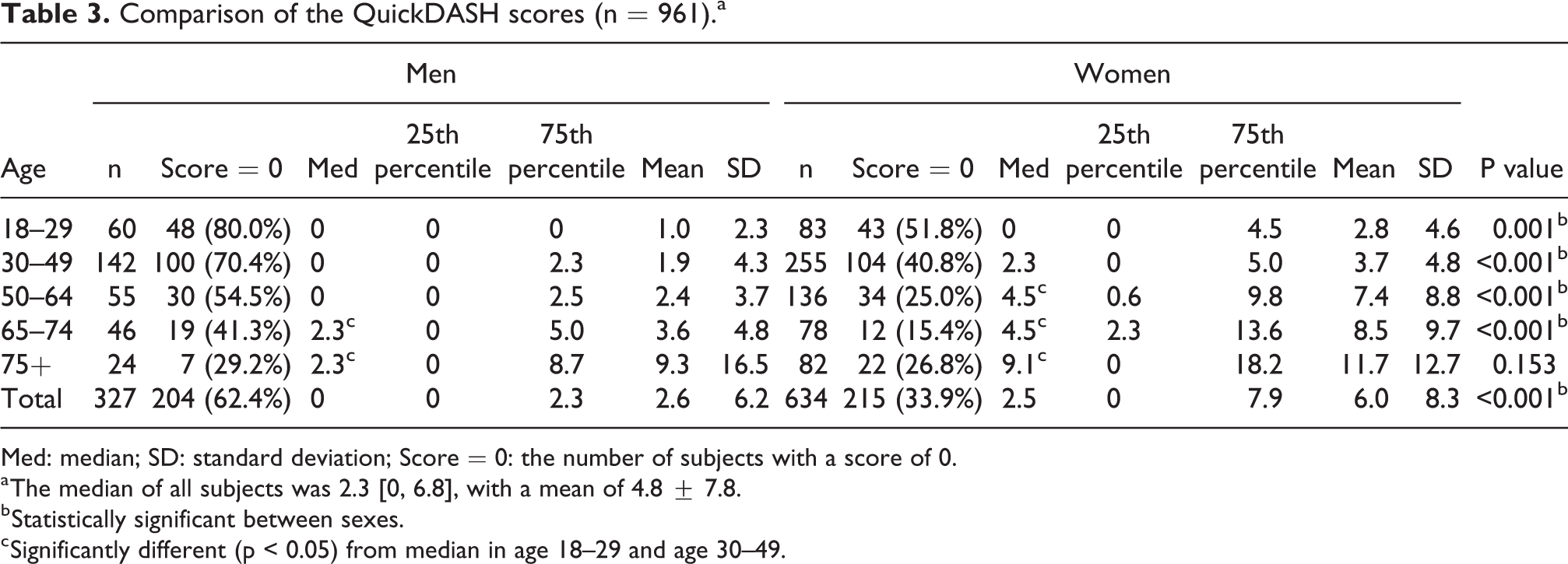
Med: median; SD: standard deviation; Score = 0: the number of subjects with a score of 0.
a The median of all subjects was 2.3 [0, 6.8], with a mean of 4.8 ± 7.8.
b Statistically significant between sexes.
c Significantly different (p < 0.05) from median in age 18–29 and age 30–49.
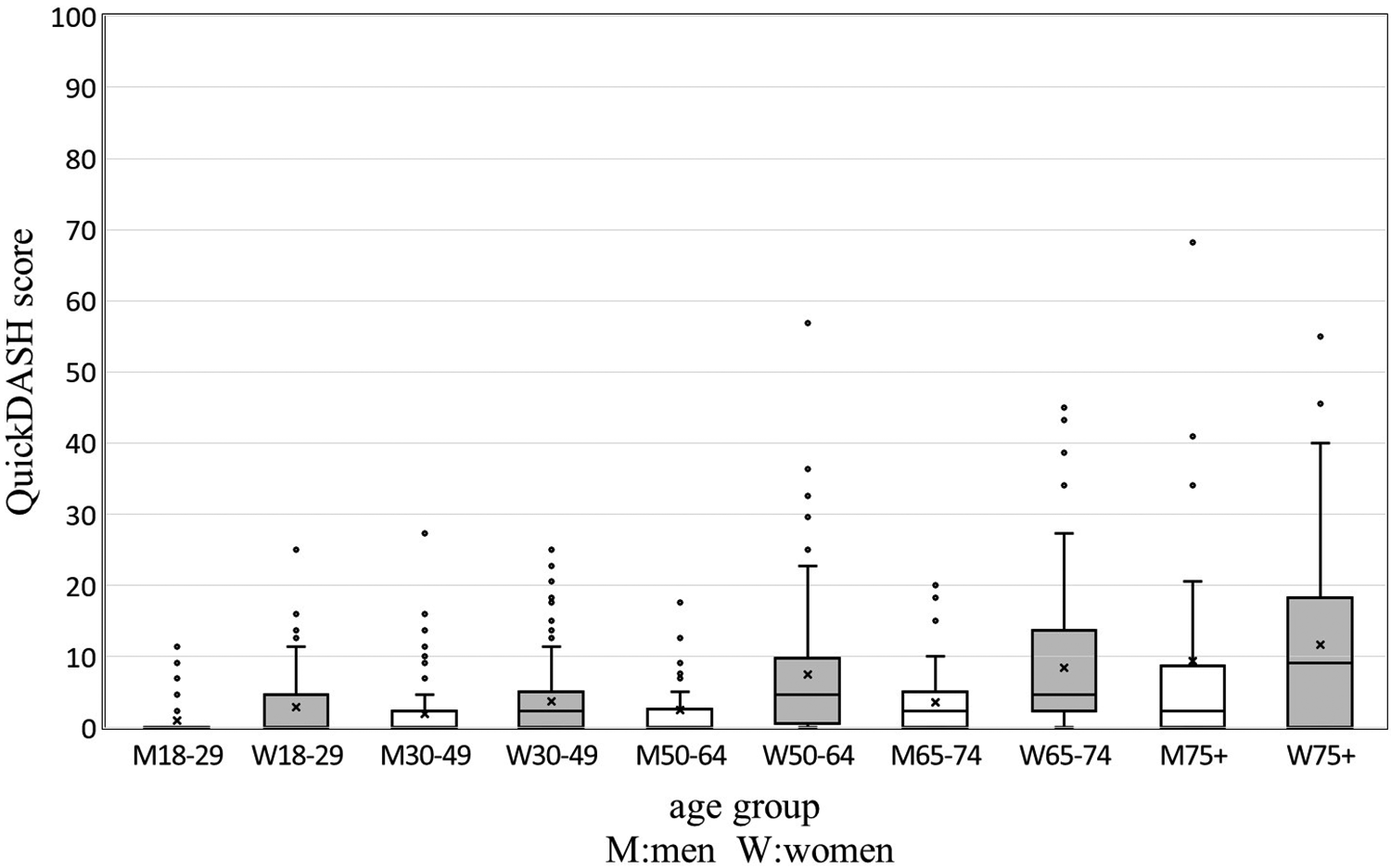
Box-and-whisker plot of the QuickDASH scores.
Table 4 shows the work score. The median of all subjects was 0 [0, 0], with a mean of 3.5. Women’s mean scores increased with age. Women showed higher work score than men in the age group of 75+ (p = 0.05) and total subjects.
Comparison of the work scores (n = 779).a

Med: median; SD: standard deviation; Score = 0: the number of subjects with a score of 0.
a The median of all subjects was 0 [0, 0], with a mean of 3.5 ± 9.4.
b Statistically significant between sexes.
Table 5 shows the sports/music score. The median of all subjects was 0 [0, 0], with a mean of 4.7. Although women’s mean scores increased with age, there were no statistically significant differences between sexes.
Comparison of the sports/music scores (n = 285).a

Med: median; SD: standard deviation; Score = 0: the number of subjects with a score of 0.
a The median of all subjects was 0 [0, 0], with a mean of 4.7 ± 12.8.
There were high correlations among the scores (QuickDASH score and work score: rs = 0.537, QuickDASH score and sports/music score: rs = 0.548, work score and sports/music score: rs = 0.639).
Tables 6 and 7 show the comparison between nonmanual and manual laborers in the QuickDASH score and work score respectively. In both sexes, there were no significant differences in QuickDASH and work scores between nonmanual and manual laborers.
Comparison of the QuickDASH scores between nonmanual and manual laborers.
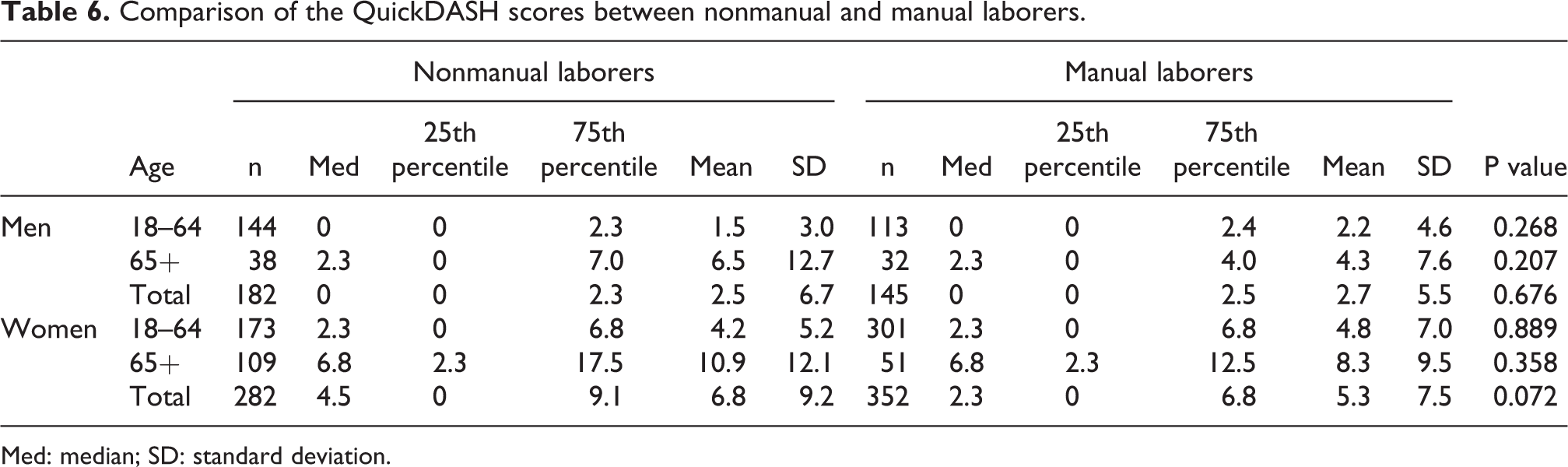
Med: median; SD: standard deviation.
Comparison of the work scores between nonmanual and manual laborers.

Med: median; SD: standard deviation.
A multiple regression analysis with the QuickDASH score as the objective variable and patients’ factors (“age,” “female sex,” “left-handedness” and “manual laborer”) as the explanatory variables was calculated by the stepwise method. Calculations were performed for the overall population, 18–64 years of age, and 65+ years of age. The factors that significantly affected QuickDASH scores were “female sex” and “age” in all three analyses. Manual laborer and left-handedness did not affect the QuickDASH score. The formula for calculating the QuickDASH score in these analyses was as follows:

Discussion
In the present study, the QuickDASH score increased with age and was higher in women than in men. This is similar to past reports. 5,8,9 Haugen et al. reported that osteoarthritis of the hand developed more often in women and the elderly than in others and they also reported that, even in the absence of symptoms, radiographic osteoarthritis and erosive osteoarthritis were more common in women and progressed over time. 11 Fillingim et al. reported in their review that women were at substantially greater risk for many clinical pain conditions than men, and the prevalence of any chronic musculoskeletal pain condition was higher among women than men. 12 Mani and Gerr found that the rates of work-related upper extremity musculoskeletal disorders increased with age and in women, particularly trigger finger and carpal tunnel syndrome. 13 Although we did not conduct a detailed study of the aforementioned diseases in each subject, the fact that the QuickDASH scores were higher for women and the elderly would suggest that the general population—especially women and the elderly—who did not receive treatment at a medical facility included people with conditions related to upper limb disorders. To understand the degree of potential upper limb impairment in the general population is important for preventive medicine and may help provide opportunities for the prevention and treatment of upper limb-related diseases, especially in women and the elderly.
The normative mean DASH scores were reported to be 10.1 in the US according to Hunsaker et al., 14 13 in employed adults and 11.8 in non-clinical subjects in Germany according to Jester et al., 8,15 9.6 in working subjects according to Klum et al., 9 and 13 in Norway according to Aasheim and Finsen. 5 On the other hand, the normative QuickDASH scores—to the best of our knowledge—have only been reported from Norway by Aasheim and Finsen, who reported that the mean QuickDASH score was 14, which was 1 point higher than the mean DASH score. 5 Gummesson et al. examined various diseases and clarified that the QuickDASH score was 4.2 points higher than the DASH score at baseline and 1 point higher at a mean follow-up of 12 months. 16 We therefore cannot simply compare the DASH and QuickDASH scores. Since reports on normative QuickDASH values are still scarce, this data would be useful information.
Regarding manual labor, Jester et al. and Klum et al. conducted studies in German working subjects ≤65 years old and found that manual laborers showed a higher DASH score than nonmanual ones. 8,9 With respect to the decision on manual labor, Jester et al. let the examiners self-assess their own work as manual or non-manual, and Klum et al. defined assembly line workers, nurses, mechanics, construction workers, and gardeners as high manual strain jobs, and office workers, salesmen, administrators, and students as low manual strain job. In contrast, in the present study, although both men and women under 65 years of age showed higher mean QuickDASH and work scores in, the differences between non-manual and manual laborers were not statistically significant. The manual labor did not affect the QuickDASH score in a multiple regression analysis. Although our method of determining manual labor was similar to Klum et al.’s, unlike their results, the impact of manual labor on the QuickDASH score was deemed to be slight. This may have been due to the fact that nurses and caregivers accounted for about 72% of manual laborers under 65 years of age in this study, but a smaller proportion of workers engaged in more high-load tasks than nurses.
The DASH and QuickDASH are suitable for evaluating the same patient over time. It may therefore not be appropriate to compare these scores among patients. However, the scores of patients who have suffered an injury cannot be compared with the scores before the injury, and even if patients could recall their state before injury, the remembered QuickDASH score has been reported to be incorrect. Wormdal et al. found that the remembered preoperative QuickDASH score was 7.6 points higher than the actual score, 17 and Hillesund et al. reported a discrepancy of 9 points. 18 Therefore, understanding the normative values of general population of different ages, sexes, and occupations would be useful for think of the QuickDASH score of similar patients.
Two limitations associated with the present study warrant mention. First, it is preferred to target randomly extracted subjects in order to conduct surveys of the general population. However, it was difficult to actually randomly gather a large number of volunteers in our study, so we asked our staff, their families, and the participants in the group meetings organized regularly by our institution’s staff. Because the majority of subjects under 65 years old were members of our staff, i.e. many medical personnel, there was no denying the influence of an occupational bias. And the group meetings are for the purpose of health promotion. The elderly subjects who participated in these meetings may therefore have had a high interest in health, which would have resulted in selection bias.
Second, in the multiple regression analysis, the factors that influenced the QuickDASH score were “age,” and “female sex.” However, the adjusted R2 was 0.146, therefore, the influences of these two elements were not so great. The DASH or QuickDASH have been reported to correlate with the Short-Form 36 Health Survey (SF-36), 6,19 –21 EuroQol-5-dimension-3-level (EQ-5D-3L), sleep disturbance, 22 depression, psychological distress, 23,24 education or income. 25 From the above, various factors are thought to affect the QuickDASH.
However, the present data collected from a relatively large number of participants of various occupations with a wide age range might serve as one of the normative values for the average Japanese QuickDASH score. Further research is needed that includes many occupations and examines multiple factors that affect the QuickDASH.
The present study determined the QuickDASH scores for 961 Japanese volunteers who were not receiving upper limb treatment in a medical facility. The median was 2.3, with a mean of 4.8. The factors that affected the QuickDASH score were older age and female sex. This study helped us to understand the degree of potential upper limb impairment in the general population. We believe that this information will help educate people about the widespread distribution of risk for upper limb disorders, especially among women and the elderly, and be useful in the populational strategies to prevent and treat the development of upper limb-related diseases. 26
Footnotes
Acknowledgment
The authors would like to express their deepest gratitude to Dr Mitsuo Uchida, Associate Professor, Department of Public Health, Graduate School of Medicine, Gunma University, for his support of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.