
Abstract
Purpose:
This study aimed to evaluate the clinical outcome and graft survival following coronoid reconstruction with osteochondral bone grafts for post-traumatic coronoid deficiency treatment. We hypothesized that coronoid reconstruction using an osteochondral bone graft will provide favorable results in treating post-traumatic coronoid deficiency.
Methods:
A retrospective review was performed on eight patients (mean age = 45.8 years) who underwent osteochondral bone graft reconstruction indicated for post-traumatic coronoid deficiency. The osteochondral bone grafts were obtained from the radial head remnant (four patients), olecranon tip (two patients), and iliac crest (two patients). All the injuries were terrible triad. The mean duration from injury to surgery was 79.3 weeks. The visual analog scale (VAS) for pain, motion arc, and Mayo elbow performance score (MEPS) were used to evaluate the clinical outcome. Radiologic evaluation of graft healing and integrity was performed using computed tomography at 19 months and plain elbow radiography at 24.1 months after reconstruction. The immediate graft height was measured.
Results:
VAS and MEPS values improved from 4.1 ± 1.2 to 1.1 ± 0.3 and 34.2 ± 16.9 to 85.0 ± 7.1, respectively (p = 0.018, p = 0.018) after reconstruction. The motion arc significantly improved from 84.2° ± 16.1° to 102.1° ± 18.2° at the final follow-up of 39.1 ± 18.8 months (p = 0.048). All the osteochondral grafts survived, with nonunion in two patients (25%). The mean immediate graft height was 15.4 ± 2.6 mm. Among the eight patients, three (37.5%) developed secondary osteoarthritis of the ulnohumeral joint.
Conclusions:
Coronoid reconstruction with osteochondral bone graft may serve as an option to salvage post-traumatic coronoid deficiency. Sufficient graft height was required for graft survival. Secondary osteoarthritis of the ulnohumeral joint should not be underestimated during follow-up.
Keywords
Introduction
Coronoid fractures are a complex issue in elbow surgery that results from failure to withstand axial loading of an upper extremity when the elbow is flexed from 0° to 35°. 1 The traditional classification by Regan and Morrey has widely been used to characterize coronoid fracture configuration, and it serves as a simple guideline for treatment. 2 Treatment options depend on fracture severity and elbow stability as well as the associated lesions of the elbow joint.
The role of the coronoid process is gaining more recognition as an important anterior buttress to the ulnohumeral joint. The critical threshold of elbow stability requires at least half of the coronoid height (Regan–Morrey type III). 3,4 The problem arises when surgeons deal with a complex coronoid that may compromise elbow stability. When the fragment of the coronoid fracture is extremely small, which is not amenable for fixation, coronoid fractures are occasionally debrided or left unfixed at the initial injury. Under these conditions, the elbow develops a chronic instability pattern for which an accepted treatment has not yet been developed. 5
We have managed chronic post-traumatic coronoid deficiency using structural osteochondral graft in eight patients with chronic elbow instability. The procedure to buttress the anterior ulnohumeral joint was borrowed from the Eden–Hybbinette procedure, which has been used for treating anterior instability of the glenohumeral joint with a bone block procedure. 6 All the patients had a previous terrible triad injury. The primary aim of the present study was to evaluate the clinical outcome of this reconstruction method. The secondary aim was to evaluate osteochondral graft integrity and healing following reconstruction.
Materials and methods
Institutional review board approval was obtained prior to the study initiation (No. 2019-0829). A retrospective review of the medical records revealed that structural osteochondral bone graft was used to reconstruct a deficient coronoid process in eight patients from 2012 to 2018. All procedures were conducted by a single senior elbow surgeon (I.H.J.). Medical record review was performed to obtain demographic data including age, sex, and site of elbow involvement. Patients were excluded from retrospective review in case of the following conditions: (1) the coronoid process was removed, (2) patients underwent open reduction and internal fixation of the coronoid fracture, (3) there was no complete medical record regarding the functional outcome score and radiologic assessment, and (4) patients had <24-month follow-up period. In all patients, the injury was closed. All the injuries were terrible triad: elbow dislocation with a lateral collateral ligament tear and fracture of the coronoid and radial head (Figure 1). Overall, one patient had concomitant posterior interosseous nerve injury. The coronoid fractures were classified as Regan–Morrey type II (four patients, 50%) and type III (four patients, 50%). According to the O’Driscoll classification, five and three patients had anteromedial- and basal-type fractures, respectively (Table 1). Among the eight patients, four had a subacute case (<1-month injury), whereas the remaining four had a chronic case.

Preoperative plain elbow radiograph of terrible triad case.
Preoperative patient characteristics.

M: male; F: female.
Surgical technique
Patients were placed in the supine position with a 250-mmHg inflated tourniquet at the affected arm. A standard Kocher lateral approach using an interval between the anconeus and extensor carpi ulnaris was used to address the radial head fracture. Fixing the radial head was always attempted before the salvage procedure (radial head replacement). Radial head replacement was performed with anatomic radial head implant (Anatomic radial head system; Acumed®, Hillsboro, OR).
An anterior window approach was used to reach the coronoid process. A lazy “S”-type incision was made across the elbow crease along the medial border of the biceps. During the procedure, the medial antebrachial cutaneous nerve was identified and protected. The bicipital aponeurosis was exposed and incised following the identification of the brachial fascia. The brachial artery, brachial vein, and median nerve were identified following an interval split between the brachial artery and median nerve. The lateral insertion of the brachialis muscle was incised to expose the anterior capsule of the ulnohumeral joint. A longitudinal incision was performed to expose the coronoid fracture in elbow extension. The deficient coronoid process was prepared flush with the ulna prior to graft fixation. The graft was obtained from the radial head remnant, olecranon tip, or iliac crest. The radial head remnant was used in cases when it was unsalvageable and required replacement. The olecranon tip was used in cases where there was no objective sign of valgus instability. The last resort for the osteochondral graft was the iliac crest. The harvested graft was then shaped to the desired shape of the coronoid using an oscillating saw and bone rongeur. Thereafter, the graft was positioned and temporarily fixed with a 2.0-mm Kirschner wire. A headless compression screw system (2.4 mm; DePuy Synthes, West Chester, PA) was used in all patients for final graft fixation under an image intensifier (Figure 2). The screws were used as lagged screws to provide compression at the site of osteosynthesis. The lateral collateral ligament complex was reconstructed if persistent instability occurred following coronoid reconstruction. 7

Graft height measurement at immediate postoperative plain elbow radiography following coronoid reconstruction with ipsilateral olecranon tip.
Outcome assessments
Pre- and postoperative outcome assessments were performed by a single independent clinical examiner who was not involved in the surgery. Functional outcome included pain evaluation using the visual analog scale (VAS), Mayo elbow performance score (MEPS), and motion arc. Complications of the procedures were recorded. Radiologic outcome was evaluated using plain elbow radiography and computed tomography. 8 The graft height was measured immediately after the operation (Figure 2). Graft integrity and healing were postoperatively documented during the follow-up period (Figure 3). The presence of post-traumatic osteoarthritis of the elbow joint was evaluated using Broberg and Morrey classification. 9

Postoperative CT scan evaluation following hardware removal showing healed graft (a) with mild arthritic changes of ulnohumeral joint (b).
Postoperative protocols
The patients were postoperatively immobilized for 3 weeks in a long-arm splint in 90° elbow flexion with neutral rotation. Subsequently, the splint was removed to allow gentle and supervised range of motion (ROM) exercises in the overhead position for another 3 weeks. The splint was weaned off over the subsequent 6 weeks depending on the elbow stability and mobility.
Statistical analysis
The Kolmogorov–Smirnov test was used for normal distribution. Post hoc power analysis was performed to detect a mean difference of 50 between the pre- and postoperative MEPS. The study would require a sample size of at least five for each pair to achieve 80% power with a 5% significance level. 10 The data set for the VAS, motion arc, and MEPS showed a skewed distribution; therefore, the Wilcoxon signed-rank test was used for statistical comparison. The Wilcoxon signed-rank test was also chosen because of the modest sample number, which required a nonparametric test to proceed with the statistical analysis. A correlation matrix was performed to assess the binary correlation of each continuous variable. The Pearson correlation test was performed following the significant interpretation of the correlation matrix table. Significance level was set at <0.05. All descriptive and statistical analyses were conducted using SPSS Version 22.0 (SPSS, Inc., Chicago, IL).
Results
Overall, six men and two women with a mean age of 45.8years at the time of surgery (range = 22–66 years) were analyzed in this study. Among the eight patients, five (62.5%) were involved in deskbound jobs and three (37.5%) performed manual labor. There were no professional athletes in this study. Further, four elbows (50%) involved the dominant arm. The mean duration from injury to surgery was 79.3 weeks. The coronoid injuries were classified as type II (four patients, 50%) or type III (four patients, 50%) according to the Regan–Morrey classification. 2 All patients were free of elbow arthritis as assessed by preoperative CT scans. The preoperative patient characteristics are presented in Table 1.
All the donors for the osteochondral grafts were autologous, which varied from the olecranon tip (two patients), bicortical iliac crest (two patients), and radial head remnant (four patients). The mean graft height was 15.4 ± 2.6 mm as measured by immediate postoperative plain radiography. The osteochondral graft was evaluated using CT (at mean duration of 19 ± 7.4 months postoperatively) and plain radiography (at a mean duration of 24.1 ± 8.6 months postoperatively) in all patients. All grafts survived at the final radiologic evaluation. However, two patients (25%) experienced nonunion of the grafts. The perioperative details are summarized in Table 2.
Perioperative surgical details.

LUCL: Lateral ulnar collateral ligament.
The mean follow-up duration was 39.1 ± 18.8 months. At the final follow-up, VAS, motion arc, and MEPS significantly improved (Tables 3 and 4). Heterotopic ossification developed in one patient, and radial head nonunion was observed in one patient. Among the eight patients, three (37.5%) developed secondary osteoarthritis of the ulnohumeral joint (one patient with grade 1 and two patients with grade 2 elbow arthritis). 9 No postoperative infections were reported. Implant was removed in one patient due to the personal preference. The correlation matrix showed significant value for height of the osteochondral graft to flexion ROM gain. The height of the osteochondral graft showed moderate negative correlation with flexion ROM gain (correlation coefficient, r = −0.688, p = 0.044).
Pre- and postoperative VAS, functional score, and complications.

ROM: range of motion; VAS: visual analog scale; MEPS: Mayo elbow performance score; HO: heterotopic ossification; OA: osteoarthritis.
Summary of functional outcome comparison for VAS, motion arc, and MEPS.
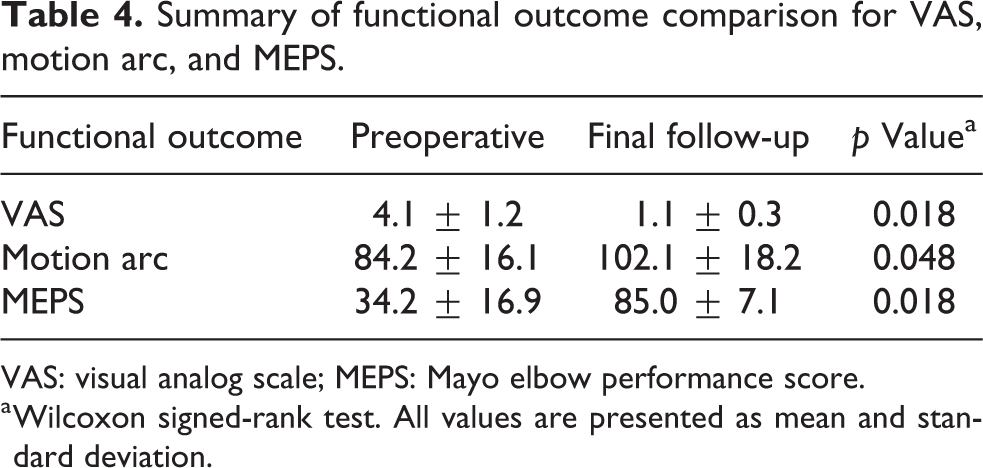
VAS: visual analog scale; MEPS: Mayo elbow performance score.
a Wilcoxon signed-rank test. All values are presented as mean and standard deviation.
Discussion
Post-traumatic coronoid deficiency is challenging in both acute and chronic settings owing to the limited knowledge regarding treatment for post-traumatic coronoid deficiency. Currently, the treatment options are soft tissue reconstruction and bone graft reconstruction, in case fixation is not amenable. 5,11 –17 Soft tissue reconstruction is not supported by evidence with questionable value. Therefore, the feasible option is bone graft reconstruction. 12
The focus of our study was to define the clinical outcome of performing osteochondral reconstruction in post-traumatic coronoid deficiency. The first important finding of our study is that osteochondral reconstruction for post-traumatic coronoid deficiency resulted in an improved functional score despite the expected occurrence of secondary osteoarthritis of the ulnohumeral joint. The result of osteochondral coronoid reconstruction for post-traumatic coronoid deficiency has been reported as favorable in several studies. 5,11,13 –17 Bain et al. described the use of costochondral rib grafts as another option for a graft source for coronoid reconstruction. 18 Most of the available literature include case reports with short-term follow-ups. Van Riet et al. have reported that reconstruction in six patients with radial head auto- and allograft resulted in variable outcomes (excellent in one, good in two, fair in one, and poor in two patients). 5 The type of fixation varied according to screws, Steinmann pins, and one-third tubular plate. Ring et al. evaluated eight patients in whom reconstruction was performed using radial head autografts and one fixation screw; these patients were followed up for an unspecified duration. The result was excellent in four, good in one, and fair in three patients. 11 Nevertheless, the injuries varied in the patients evaluated. Bellato et al. evaluated three patients in whom reconstruction was performed with the concave proximal articular surface of the radial head, reportedly preventing osteoarthritis. 13 The postoperative evaluation was performed using CT scans at early postoperative times (3 months for two patients and 6 months for one patient) in the study by Bellato et al. However, in the current study, three patients (37.5%) developed secondary osteoarthritis, which is inconsistent with the results obtained by Bellato et al. We postulated that because all our patients had high-energy injuries and their mean age was relatively greater than those reported from Bellato et al., the findings in the previous studies 5,11,13 –17 may have been resulted from short-term radiologic follow-up which underestimated the risk of secondary osteoarthritis. We suggest that surgeons should educate patients regarding the risks and benefits of osteochondral reconstruction for post-traumatic coronoid deficiency.
The second finding in our study is that none of the osteochondral graft was resorbed at the final radiologic follow-up. One patient with healed osteochondral grafts did not undergo CT scan evaluation for personal reasons; nevertheless, the interpretation of the plain radiographs was definite. From our clinical experience, we believe that a graft should be sufficiently large to ensure its survival. A considerable graft size will provide better contact area to the native olecranon for even distribution of the load. We only measured the graft height because it is difficult to measure the width in the immediate postoperative radiographs. The mean height of our osteochondral graft was 15 mm. We believe that this height is sufficient considering that none of the grafts were resorbed. Furthermore, the bone graft quality determines the rigidity of fixation, and this is important in achieving excellent initial stability, which will favor the clinical outcome. Additionally, the number of fixation screws is important to achieve excellent initial stability with the concern of graft failure for overcrowded fixation. In the current study, at least two screws were used in each case. The use of an additional screw (more than one) provided stability, as adapted from the treatment of medial malleolar fractures with one fixating screw and one anti-rotation screw. 19 We did not use a hinged external fixator as described by van Riet et al. 5 because we believe that a stable fixation will preclude the need of it. The application of external fixation will prolong the operative time and may increase the risk of pin site infection.
Another contingent finding in our study is that most patients exhibited limited flexion postoperatively, which was observed more in patients with radial head remnant and iliac crest graft than those with an olecranon tip graft. The mean height of the radial head and iliac crest grafts was 16.4 and 17.4 mm, respectively, whereas that of the olecranon tip graft was 11.9 mm. Consequently, a more prominent graft was expected from patients with radial head and iliac crest graft, which resulted in slight flexion loss. Regardless of this slight flexion loss, we believe that this height is acceptable considering that the ulnohumeral joint will gain more stability.
The coronoid process plays a major role in maintaining elbow stability and function. 3 The coronoid osteochondral reconstruction procedure can salvage a complex elbow injury with acceptable outcomes at the final follow-up assessments. A sufficient graft size is important to avoid graft resorption despite the potential limitation of postoperative flexion.
Limitations
This study has some limitations. First, the study design was a retrospective case series from a single surgeon without a control arm. Second, the sample size was small owing to the rarity of the procedure. However, the number of cases performed was, to the best of our knowledge, the largest reported in the English literature. These limitations may lead to the possibility of limited external validity of our findings. We believe that further clinical studies with a larger sample size are required to confirm the ideal graft and surgical technique for post-traumatic coronoid deficiency. Third, the study did not investigate the optimum graft size that would balance stability versus ROM. With advancements in reverse engineering technology, we believe that digital imaging and three-dimensional reconstruction can be used to assist graft selection matching.
Conclusions
Osteochondral coronoid reconstruction can be a salvage option for post-traumatic coronoid deficiency. Sufficient graft size is pertinent to avoid graft resorption. Secondary osteoarthritis of the ulnohumeral joint might be expected in the long term.
Footnotes
Acknowledgments
We thank Park Jong Hwee CNS for her assistance in collecting medical information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the convergence technology development program for bionic arm through the National Research Foundation of Korea (NRF) funded by the Ministry of Science & ICT (No. 2014M3C1B2048422).