
Abstract
Purpose:
The effectiveness of total knee arthroplasty (TKA) for recovering ambulation and balance functions has not been investigated in detail. The present study aimed to measure functional changes in the lower limb before and after TKA by measuring ambulation function with the 3 m Timed Up and Go (TUG) test and balance function using one-leg standing time (ST).
Methods:
The study included 137 patients (116 women and 21 men) with osteoarthritis of the knee who underwent primary TKA. The mean age of the patients was 74.4 years. The mean postoperative hospital stay for rehabilitation was 23.9 days. The TUG test and ST were performed preoperatively, 2 weeks postoperatively, at discharge, and 3, 6, and 12 months postoperatively. These results from these six measurements were also compared using one-way repeated measures analysis of variance.
Results:
The TUG test and ST were significantly improved at 3 months after surgery. However, both the TUG test and ST did not improve further from 3 months to 6 months postoperatively or from 6 months to 1 year postoperatively.
Conclusion:
TKA is useful for restoring lower limb function, as both ambulation and balance functions were significantly improved 3 months after surgery. However, no further improvement in ambulation or balance function was recognized beyond 3 months.
Introduction
Osteoarthritis (OA) of the knee joint is the most common indication for total knee arthroplasty (TKA). The incidence and prevalence of OA is likely to continue increasing owing to factors such as the aging population in developed countries. 1 Furthermore, OA is an important risk factor for falls. Falls are among the most common causes of injury and hospitalization in elderly individuals. 2 TKA aims to relieve pain, restore motor abilities, correct lower limb deformities, and improve quality of life. 3 However, patients undergoing TKA owing to knee OA often have residual functional deficits, such as ambulation and balance deficits, which increase the risk of falls. 4
There is a concept of musculoskeletal ambulation disability symptom complex (MADS) that indicates the elderly population with a high risk of falls and ambulation deficits caused by musculoskeletal disorders. The diagnosis of MADS is composed of two parts: (1) a musculoskeletal disorder must be diagnosed, which includes deteriorating ambulation and balance functions, and (2) the degree of independence in the activities of daily living must decrease to the point of requiring support or nursing care, or a functional decline in ambulatory function must be observed (Table 1). 5 The functional evaluation involves two simple performance tests; MADS is diagnosed if the 3-m Timed Up and Go (TUG) test time 6 is 11 s or more and/or the one-leg standing time (ST) with open eyes 7 is less than 15 s. 8
The diagnosis criteria of MADS.

MADS: musculoskeletal ambulation disability symptom complex; ST: standing time; TUG: Timed Up and Go.
Rehabilitation with a particular emphasis on physiotherapy and exercise is widely promoted after TKA. 9 Physiotherapy targets mobilization and achievement of functional goals relating to hospital discharge. Length of hospital stay after TKA varies widely from country to country, 10,11 and these differences may depend on each institute’s capacity to perform postoperative inpatient rehabilitation. Our institution allows patients to determine the length of their hospital stay and to receive rehabilitation every day, taking into consideration uncontrolled pain and unstable transfer.
Some papers have reported the effect of TKA on postoperative ambulation and balance functions. 12 However, there have been no detailed reports on how TKA affects perioperative and postoperative ambulation and balance functions or differences in ambulation and balance functions due to the length of the hospital stay. The present study aimed to quantitatively evaluate changes in ambulation and balance functions before and after TKA based on the evaluation criteria of MADS by performing the TUG test and the ST. It was hypothesized that ambulation and balance functions would improve after TKA and that a longer hospital stay with rehabilitation would improve ambulation and balance functions.
Materials and methods
Of the 296 patients who underwent primary TKA between March 2013 and July 2016 who were screened for this study, 141 were enrolled. The reasons for exclusion included unilateral OA (n = 38), a lack of follow-up data from all evaluation periods (n = 28), rheumatoid arthritis (n = 25), arthritis due to infection (n = 5), secondary knee OA (n = 37), and ipsilateral adjacent joint disease (n = 22). Four patients were lost to follow-up during the 12-month study period. This retrospective study therefore included 137 patients (116 females and 21 males) with bilateral knee OA. The patients were followed up for 1 year and did not received another TKA on the contralateral side during this period. The patients’ mean age, length of hospital stay for rehabilitation, body mass index (BMI), range of motion, hip-knee-ankle (HKA) angle, contralateral knee status, and comorbidities are listed in Table 2. The HKA angle is measured lower limb alignment on a full-length lower limb radiograph, defined as the angle between the mechanical axes of the femur and the tibia (positive value in varus). 13 Of the patients, 128 had varus knees and 9 had valgus knees. Contralateral knee status was classified in accordance with the Kellgren and Lawrence (KL) classification or was postoperative TKA. The comorbidities were under well controlled. The hospital ethics committee approved the study protocol, and the patients provided informed consent for participation. Patients were encouraged to perform preoperative self-rehabilitation for facilitating their postoperative rehabilitation. This program included isometric exercises and stretching of the quadriceps, hamstring, and gluteal, muscles; squatting, and straight leg rising exercises. All operations were performed by a single surgeon (HM). TKAs were performed with a medial parapatellar arthrotomy approach. Inpatient rehabilitative treatment was started on the day after surgery, and the rehabilitation was performed every day. The postoperative rehabilitation protocol included passive range of motion exercises; quadriceps, hamstring, and gluteal isometric exercises; gait and transfer training and straight leg rising exercises up to 2 weeks after surgery. The subsequent protocol included active range of motion exercises, stationary cycling, progressed quadriceps hamstring and gluteal isometric exercises, stepping exercises, and gait training to wean off of assistive devices. These protocols were performed by physiotherapists with a minimum of 10 years’ experiences. Duration of hospital stay depended on the social background such as patient age and activity level. The patients remained in the hospital until they were ready to leave—that was until they reached activity levels with which they could live independently at home without preparation of a care house. Regular home self-rehabilitation after discharge was performed in addition to regular hospital visits. No adverse events such as infection and aseptic loosening occurred, and no revision surgery was needed in any of the cases during the follow-up period.
Demographic and clinical data.a
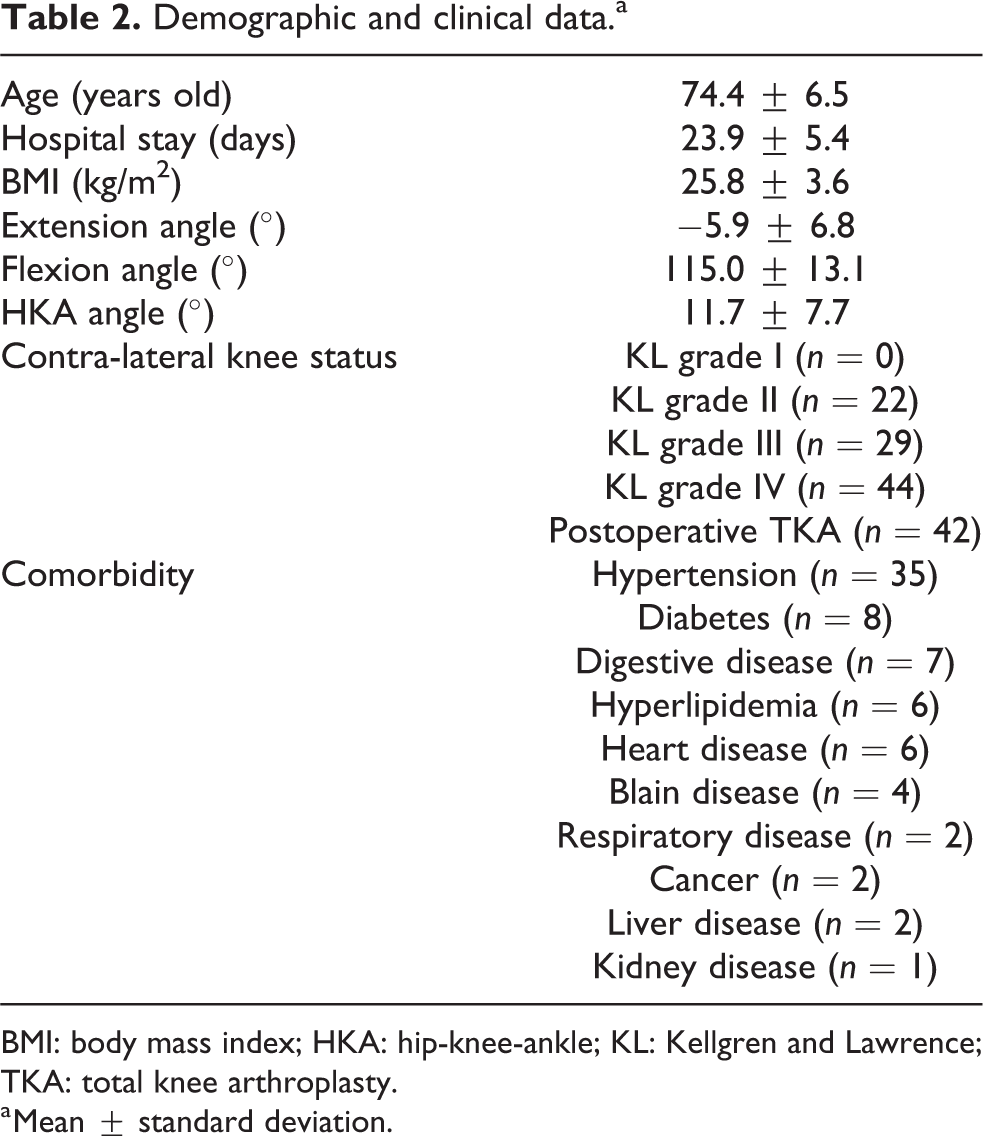
BMI: body mass index; HKA: hip-knee-ankle; KL: Kellgren and Lawrence; TKA: total knee arthroplasty.
a Mean ± standard deviation.
Evaluation of ambulation and balance functions and the timing of measurements
The TUG test was used to evaluate the patients’ ambulation ability in order to diagnose MADS. The TUG test was performed preoperatively, 2 weeks postoperatively, at discharge, and 3, 6, and 12 months postoperatively. This test measures the time taken to rise from a chair, walk straight for 3 m, turn around, walk back, and sit down on a chair. The time is measured from the seated position with a stopwatch starting on the command “ready go” and is stopped when the participant sits down. The average time of three trials was calculated, and the time was recorded to the nearest 0.1 s.
The ST was also used to evaluate balance ability in order to diagnose MADS. The ST on the operative side was also performed preoperatively, 2 weeks postoperatively, at discharge, and 3, 6, and 12 months postoperatively. The test measures the duration that the participants can stand on one leg with eyes open, hands placed on the hips, and the other foot raised at least 5 cm. The average longest time of three trials was selected, and the time was recorded to the nearest 0.1 s.
The TUG test and ST were individually performed face-to-face with patients with barefoot by physical therapists on a horizontal floor in the physiotherapy room without any noise. The importance of these tests to the patients was documented, and the fidelity for these tests was maintained.
Diagnosis of MADS
MADS is diagnosed if the 3 m TUG test time is 11 s or more and/or the one-leg ST with open eyes is less than 15 s. The percentage of patients with MADS was calculated at each measurement point. We calculated the percentage of reduced ambulation ability (TUG ≥ 11 s) and balance ability (ST < 11 s) at each measurement point.
Statistical analysis
The values in demographic and clinical data were expressed as the mean ± standard deviation, and the values of TUG test time and ST were expressed as the mean ± standard error. The results were analyzed statistically using the Statview statistical software package (ver. 5.0; Abacus Concepts, Inc., Berkeley, California, USA). The TUG test and ST results were compared among the six time periods using one-way repeated measures analysis of variance. We separated the patients into three groups by the length of hospital stay: 3 weeks or less (early discharge group (EDG)), 3–4 weeks (standard discharge group (SDG)), and over 4 weeks (late discharge group (LDG)). The TUG test time and ST among the three groups were evaluated using a one-way analysis of variance. The 137 patients included in the present study were divided into groups as follows: KL grade I (0 patient), KL grade II (22 patients), KL grade III (29 patients), KL grade IV (44 patients), and postoperative TKA groups (42 patients). The TUG test time and ST according to the contralateral knee status were also evaluated using one-way analysis of variance. The relationships between the TUG test time and ST were evaluated using simple regression analysis at each of the six time points. A value of p < 0.05 was set statistically significant. A statistical power analysis was performed prior to the study, which was expected to require a power of 0.8, based on a prespecified significance level of α < 0.05 and assuming a medium effect size (0.25) using G*Power 3. 14 The estimated sample size was 93 patients.
Results
Changes in ambulation (TUG) and balance (ST) functions
The mean TUG test times were 12.6 ± 0.4, 16.9 ± 0.6, 13.0 ± 0.3, 11.1 ± 0.3, 10.4 ± 0.3, and 10.2 ± 0.3 s when measured preoperatively, 2 weeks postoperatively, at discharge, 3, 6, and 12 months postoperatively, respectively. The mean TUG test time was significantly higher 2 weeks after TKA than it had been preoperatively; however, the mean time was significantly lower at discharge than 2 weeks after TKA. There was no significant difference between the mean TUG test time when measured preoperatively and at discharge. The mean TUG test times at 3 months, 6 months, and 1 year after TKA were significantly improved when compared to the preoperative time. However, there was no significant improvement from 3 months to 6 months postoperatively or from 6 months to 1 year postoperatively (Figure 1(a)).

Sequential changes in (a) ambulation function (the 3 m Timed Up and Go test time), (b) balance function (the one-leg standing time with open eyes), and (c) the percentage of MADS. MADS: musculoskeletal ambulation disability symptom complex; TUG: Timed Up and Go; ST: standing time.
The mean STs on the operative side were 17.6 ± 2.1, 15.3 ± 1.8, 20.9 ± 2.4, 27.9 ± 2.9, 28.5 ± 2.7, and 25.9 ± 2.6 s when measured preoperatively, 2 weeks postoperatively, at discharge, and 3, 6, and 12 months postoperatively, respectively. There was no significant difference in the mean ST when measured preoperatively, 2 weeks postoperatively, and at discharge. The mean ST at 3 months after TKA was significantly improved compared to the preoperative ST, similar to the TUG test time. However, there was no significant improvement from 3 months to 6 months postoperatively or from 6 months to 1 year postoperatively (Figure 1(b)).
A significant correlation between the TUG test time and ST was observed at each of the six time points (preoperatively; p < 0.01, R = −0.26, 2 weeks postoperatively; p < 0.01, R = −0.30, at discharge; p < 0.01, R = −0.35, 3 months postoperatively; p < 0.01, R = −0.38, 6 months postoperatively; p < 0.01, R = −0.47, and 12 months postoperatively; p < 0.01, R = −0.45, respectively).
Changes in the percentage of MADS
The percentages of patients with MADS were 79.6%, 91.2%, 80.3%, 64.2%, 59.9%, and 61.3% when the patients were evaluated preoperatively, 2 weeks postoperatively, at discharge, and 3, 6, and 12 months postoperatively, respectively. The percentages of reduced ambulation ability (TUG ≥ 11 s) and balance ability (ST < 15 s) were 59.6% and 65.7%, 83.9% and 68.8%, 67.2% and 59.9%, 37.2% and 56.2%, 34.3% and 52.6%, and 30.7% and 56.9% when the patients were evaluated preoperatively, 2 weeks postoperatively, at discharge, and 3, 6, and 12 months postoperatively, respectively (Figure 1(c)).
TUG test time and ST according to length of hospital stay
The 137 patients included in the current study were separated into the EDG (49 patients; mean age: 73.7 years (range: 49–88 years); mean postoperative hospital stay: 19.2 days (range: 16–21 days)), SDG (63 patients; mean age: 74.9 years (range: 49–86 years); mean postoperative hospital stay: 24.0 days (range: 22–28 days)), and LDG (25 patients; mean age: 74.6 years (range: 64–88 years); mean postoperative hospital stay: 33.1 days (range: 29–45 days)). BMI, range of motion, and HKA angle are also listed in Table 3. No significant differences were observed among the three groups for mean age, BMI, range of motion, and HKA angle. The mean TUG test times and STs on the operative side are listed in Table 4. The mean TUG test times in the EDG and SDG were significantly lower than those in the LDG at all measurement points. The mean TUG test time in the EDG was significantly lower than that in the SDG 2 weeks after TKA. The mean STs in the early and SDGs were significantly longer than those in the LDG preoperatively. There was no significant difference in the mean ST between the early and SDGs (Table 5).
Demographic and clinical data of EDG, SDG, and LDG.a

EDG: early discharge group; SDG: standard discharge group; LDG: late discharge group; BMI: body mass index; HKA: hip-knee-ankle.
a Mean ± standard deviation.
b p < 0.05 Statistically significant.
The mean 3-m timed up and go test times and one-leg standing times on the operative side among EDG, SDG, and LDG.a

EDG: early discharge group; SDG: standard discharge group; LDG: late discharge group; TUG: Timed Up and Go; ST: standing time; PO: postoperatively.
a Mean ± standard deviation (seconds).
The relationships of mean 3-m timed up and go test times and one-leg standing times on the operative side among EDG, SDG, and LDG.
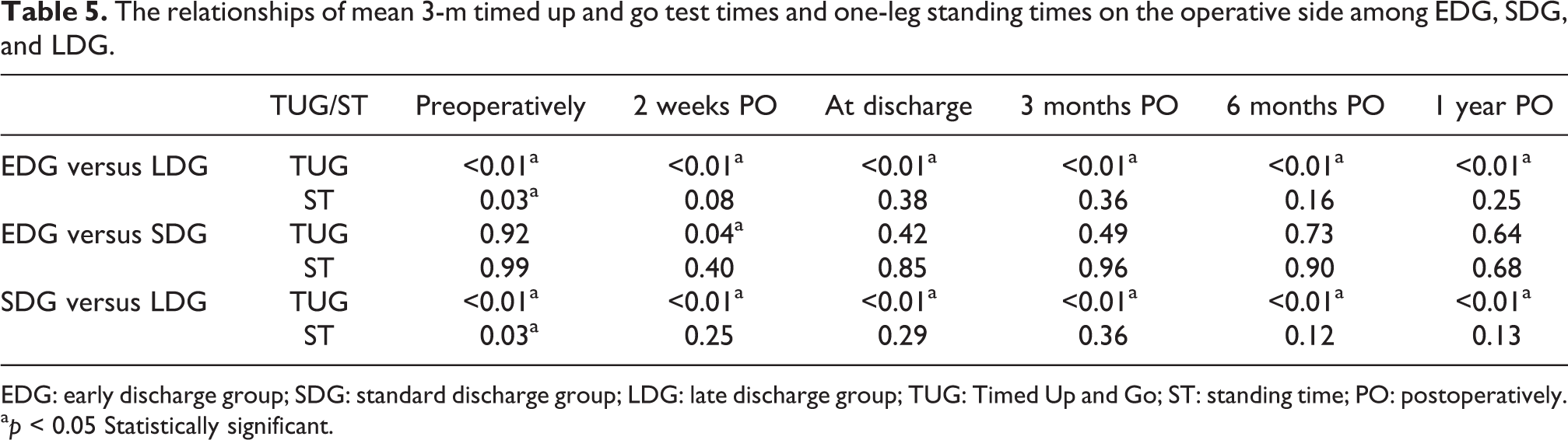
EDG: early discharge group; SDG: standard discharge group; LDG: late discharge group; TUG: Timed Up and Go; ST: standing time; PO: postoperatively.
a p < 0.05 Statistically significant.
TUG test time and ST according to contralateral knee status
The demographic data of each group are listed in Table 6. The mean TUG test time and STs on the operative side are also listed in Table 7. The mean TUG test times in the KL grade II and postoperative TKA groups were significantly lower than that in the KL grade IV group from discharge to 1 year after TKA. The mean TUG test time in the KL grade III group was also significantly lower than that in the KL grade IV group from 3 months to 1 year after TKA. No significant difference in the mean ST was found among the four groups (Table 8).
Demographic and clinical data of patients classified by contralateral knee status.a
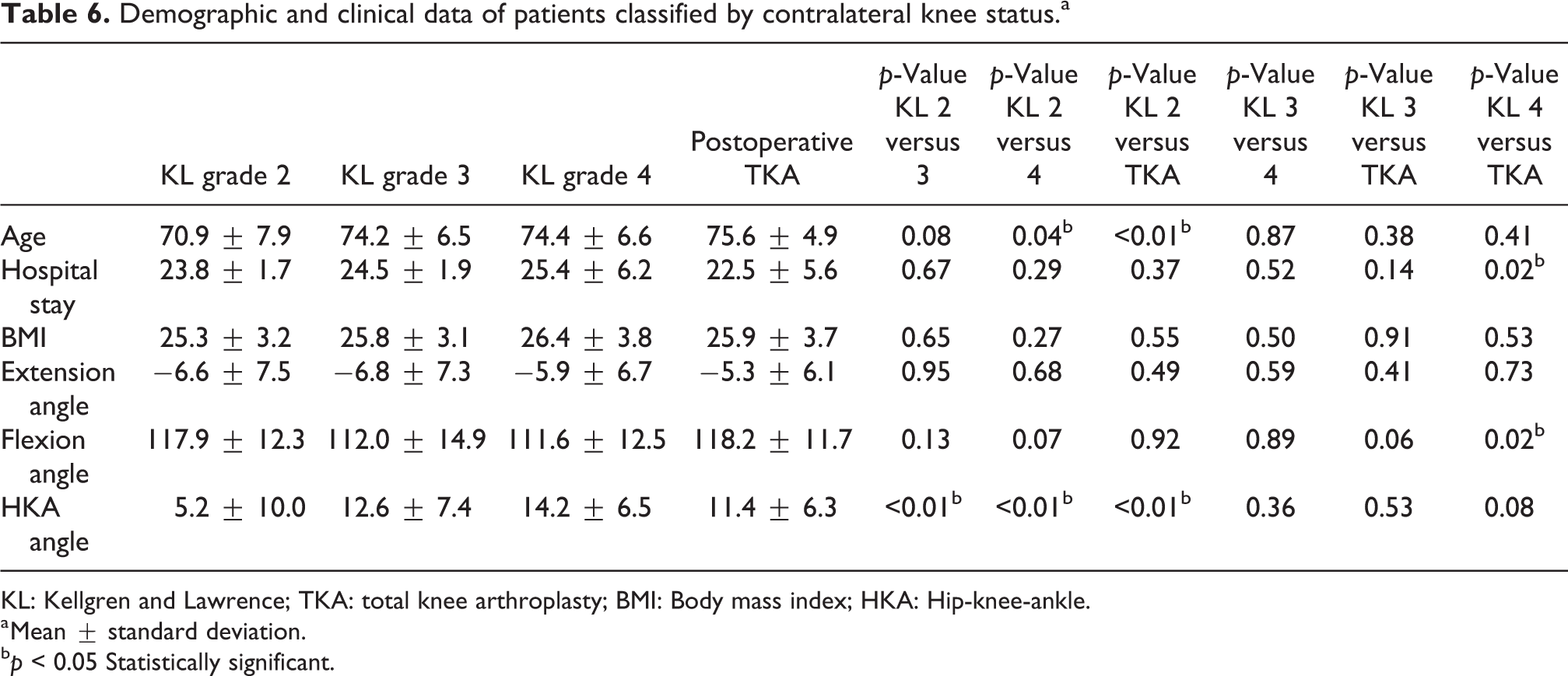
KL: Kellgren and Lawrence; TKA: total knee arthroplasty; BMI: Body mass index; HKA: Hip-knee-ankle.
a Mean ± standard deviation.
b p < 0.05 Statistically significant.
The mean 3-m timed up and go test times and one-leg standing times on the operative side among the patients classified by contralateral knee status.a

TUG: Timed Up and Go; ST: standing time; PO: postoperatively; KL: Kellgren and Lawrence; TKA: total knee arthroplasty.
a Mean ± standard deviation (seconds).
The relationships of mean 3-m timed up and go test times and one-leg standing times on the operative side among the patients classified by contralateral knee status; p values were listed.
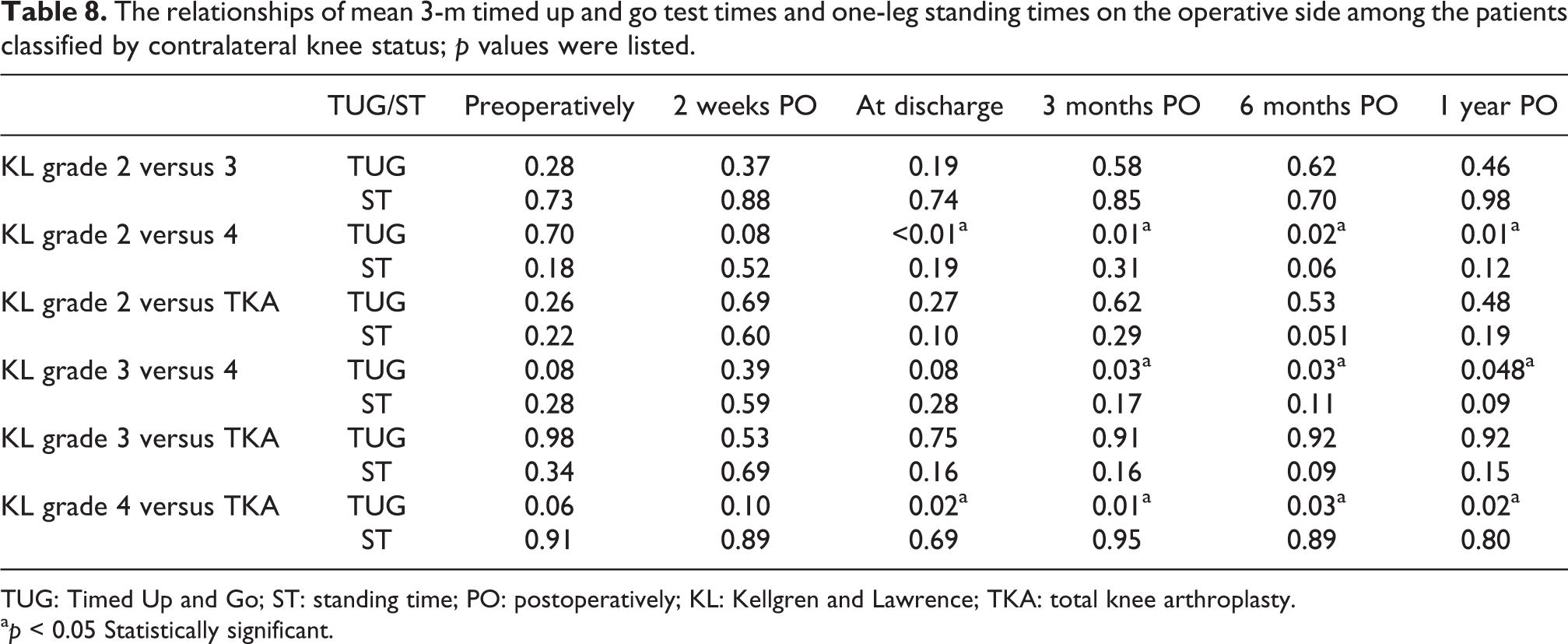
TUG: Timed Up and Go; ST: standing time; PO: postoperatively; KL: Kellgren and Lawrence; TKA: total knee arthroplasty.
a p < 0.05 Statistically significant.
Discussion
We hypothesized that ambulation and balance functions would improve after TKA and that a longer hospital stay with rehabilitation would improve ambulation and balance functions. The most important finding in this study was that ambulation and balance functions were significantly improved at 3 months after TKA, thus supporting our hypothesis. However, ambulation and balance functions did not improve from 3 months to 6 months postoperatively or from 6 months to 1 year postoperatively, thus contradicting our hypothesis. Furthermore, a longer hospital stay did not improve ambulation and balance functions, thus contradicting our hypothesis. These results suggest that patients with poor preoperative ambulation and balance functions might have a longer hospital stay and that a longer hospital stay with rehabilitation might not affect ambulation and balance functions after discharge.
MADS is defined as a condition where elderly individuals have a high risk of falls and have ambulatory disabilities caused by musculoskeletal disorders. 5 MADS is also diagnosed if the 3-m TUG test time is 11 s or more and/or the one-leg ST with open eyes is less than 15 s. The TUG test is a modified, timed version of the “Get-Up and Go” test first reported by Mathias et al. 15 It is a simple and inexpensive method to assess basic mobility with daily movements. 16 The TUG test includes sit-to-stand and stand-to-sit chair transitions, turning, straight-ahead gait, balance control, and the ability to perform tasks in sequence. 12 The ST is also a widely used clinical tool to evaluate postural steadiness in the standing position for elderly people. Previous reports suggest that ST is associated with age, self-assessment of their health status, BMI, mortality, and the risk of falls. 17 The ST involves standing on one foot, placing the hands on the hips, and raising the other foot more than 5 cm, while keeping the eyes open. 18 The TUG test and ST are simple to score, requiring minimal training and no expertise in mobility analysis. In the current study, approximately 80% of the patients preoperatively had MADS, and this number decreased to about 65% at 3 months postoperatively. Our results indicate that only about 15% of patients no longer had MADS at 3 months after surgery. The percentage of reduced ambulatory ability (TUG ≥ 11 s) improved from 59.6% preoperatively to 37.2% at 3 months postoperatively and 30.7% at 1 year postoperatively, indicating that the percentage improved at 3 months after TKA. However, the percentage of reduced balance function (ST < 15 s) improved from 65.7% preoperatively to 56.2% at 3 months postoperatively but did not improve from 3 months postoperatively to 1 year postoperatively (56.9%).
Rehabilitation with an emphasis on physiotherapy and exercise is widely promoted after TKA. 9 During the hospital stay, physiotherapy targets mobilization and achievement of functional goals relating to hospital discharge. The length of hospital stay after TKA was recently reported to range widely from 3.8 days to 35.1 days by each country. 10,11 Therefore, in countries with a short hospital stay, outpatient, community, or home-based physiotherapy and exercise-based interventions are important after hospital discharge. 9 In the current study, patients were discharged at their request, with inpatient rehabilitation continuing daily until discharge. As a result, the mean TUG test time and ST at 3 months after TKA were significantly improved compared to the preoperative TUG test time and ST. However, there was no significant improvement from 3 months to 6 months postoperatively or from 6 months to 1 year postoperatively for either the TUG test time or the ST. Unnanuntana et al. reported that the mean baseline TUG test time was 23.9 s, which subsequently decreased to 19.7, 17.1, and 15.6 s at 3, 6, and 12 months after surgery, respectively. 19 In this study, the mean TUG test times were 12.6, 11.1, 10.4, and 10.2 s when measured preoperatively and at 3, 6, and 12 months postoperatively, respectively. As a result, there was no significant improvement from 3 months to 6 months postoperatively, or from 6 months to 1 year postoperatively. However, even the TUG test time at 12 months postoperatively met the criteria for diagnosis of MADS by TUG in the report of Unnanuntana et al. The difference between these two results could have been because the baseline TUG times differed considerably. Considering the results and that no regular rehabilitation after discharge was performed in this study, we suggested that continued rehabilitation after discharge might be necessary to restore lower limb function beyond 3 months after TKA.
According to contralateral knee status, the patients were divided into the KL grade I (0 patient), KL grade II (22 patients), KL grade III (29 patients), KL grade IV (44 patients), and postoperative TKA groups (42 patients). Although no significant differences in the mean ST were found among four groups, the mean TUG test times in the KL grade II and III groups and postoperative TKA group were significantly lower than that in the KL grade IV group from 3 months to 1 year after TKA, which suggests that contralateral knee status particularly influenced ambulation function of the patients. The patients were followed up for 1 year and did not receive another TKA on the contralateral side during this period. For patients whose contralateral side was KL grade IV, permitting TKA on the contralateral side early after the TKA on the other side may be desirable.
This study has some limitations. First, the data were obtained for posterior-stabilized and cruciate-retaining TKA; therefore, the results for each type of TKA may differ. Second, we did not evaluate patients by OA stage on the operative side. Third, the TUG test and ST were only performed until 1 year after TKA. Longer term investigation of the changes in the TUG test and ST is necessary. Fourth, we did not consider the influence of range of motion and activity on preoperative or ambulation and balance abilities. Fifth, there was not a suitable age-matched reference group. Furthermore, we did not determine whether the TUS test and ST could predict the risk of falls and the success of TKA. We also did not investigate the relationships among the TUG test, ST, and other patient reported outcome measures. These assessments should be included in future studies.
Conclusion
We investigated functional changes in the lower limb before and after TKA for only bilateral knee OA by evaluating the ambulation and balance functions based on the TUG test and ST, respectively. TKA is a useful treatment for restoring lower limb function, as both ambulation and balance functions were significantly improved at 3 months after TKA. However, an improvement in ambulation and balance functions was not recognized beyond 3 months after TKA. Furthermore, a longer hospital stay with rehabilitation not always affected ambulation and balance functions, and preoperative ambulation and balance abilities may also predict the length of hospital stay after surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.