
Abstract
Purpose:
Osteoid osteomas are benign and nonprogressive lesions. The clinical presentation of osteoid osteoma is typical with night pain responsive to nonsteroidal anti-inflammatory agents. The typical radiological appearance is lucent nidus and adjacent reactive sclerosis. The most traditional management of osteoid osteoma is surgical removal which is associated with significant morbidity. This article aims to demonstrate our single-center experience of 55 patients with osteoid osteoma treated with percutaneous radiofrequency ablation (RFA).
Methods:
Fifty-five symptomatic patients who were seen at our orthopedics outpatient clinics, diagnosed with osteoid osteoma, and referred to interventional radiology department between May 2015 and April 2019 were enrolled. The nidus size, pain numeric rating scale score, and intramedullary edema diameter before and after RFA were compared. Clinical and technical success, intervention-related complications, and need for subsequent ablation were recorded.
Results:
Of the 55 patients, including 12 pediatric cases, 6 had atypical locations such as metatarsal, vertebra, and scapula, while 1 case had osteoid osteoma with multiple nidus. The mean age was 18.5 ± 9.6 years. Preintervention maximum nidus diameter, pain score, and edema diameter were significantly lower in postintervention measurements (p < 0.001). Technical success rate was 98.1%, and clinical success was 96.36%. Severe complication occurred in one patient with soft tissue burn and osteomyelitis.
Conclusion:
This is one of the largest series of osteoid osteoma treated with RFA done in a single center with atypical cases. In conclusion, RFA is safe and effective in both pediatric and adult patients with rare complications even in challenging cases with atypical locations.
Introduction
Osteoid osteomas are benign tumors of the bone that are easily distinguished from other lesions with radiological evaluation and clinical presentation. They are small and nonprogressive lesions and account for 5% of all bone tumors and 11% of benign bone tumors. 1 Most of the patients are young adults who are less than 20 years of age. 2 It is rare in patients whose age is less than 4 or more than 40. There is male predominance with a male-to-female ratio of 2:1.5. It usually involves the appendicular skeleton. Flat bones that have intramembranous formation and skull are rarely involved. 3 Most of the cases occur in the femur or tibia, with the most involved site of the femur being the neck region.
The clinical presentation of osteoid osteoma is typical with night pain responsive to nonsteroidal anti-inflammatory agents. The pain is dull and has intermittent character in most cases. 4 The typical radiological appearance is lucent nidus smaller than 1.5 cm in size and adjacent sclerotic bone reaction and edema. Less frequently patients may be seen at the clinics with complaints of growth disturbance, deformity, scoliosis, limited joint motion or swelling, erythema, and, if the osteoid osteoma is located subcutaneously, tenderness. 5
The traditional management of osteoid osteoma is removing the translucent nidus completely. However, surgery mandates hospitalization and may alter and weaken the structure of the bone which may require fixation. 6 In addition to that, patients would need more off days from school or work in case of surgery. Due to those disadvantages minimally invasive techniques emerged and developed in recent years such as radiofrequency ablation (RFA), laser photocoagulation, or percutaneous resection. 7,8 During the procedures, the most used imaging method is computed tomography (CT) which is cheap, widely available, and easy to use.
In this article, we aim to demonstrate our single-center experience of 55 patients with osteoid osteoma treated with percutaneous RFA. Our series is relatively large with atypical cases involving the scapula, metatarsal, vertebral facet, and tumor with double nidus. We also reported a dramatic complication which occurred in one patient. We evaluated the efficacy and safety of the procedure regarding ablation of the tumor and remission of the symptoms.
Materials and methods
We prospectively enrolled 55 symptomatic patients who were seen at our tertiary center’s orthopedics outpatient clinics and diagnosed with osteoid osteoma and were referred to interventional radiology department between May 2015 and April 2019. Before the start of the study, we obtained the local ethical board approval in accordance with the principles of the Declaration of Helsinki. The diagnosis was established with the clinical history of night pain which was severe and disturbing and required treatment with nonsteroidal anti-inflammatory drugs (NSAIDs) almost every day for pain relief together with typical findings on imaging with CT or magnetic resonance imaging (MRI), demonstrating a definitive nidus <1.5 cm in size with adjacent bone sclerosis. RFA decision was made by a multidisciplinary team including a radiologist and an orthopedic specialist. Contraindications for the procedure were being close to vital structures such as peripheral nerves, spinal cord or vessels (<1 cm), pregnancy, active cellulitis, sepsis, and coagulopathy. Physical examination was made for each individual to see whether the skin was intact and there was any sign of infection at the site of entry before the procedure. The lesions with a nidus larger than 1 cm in size were treated with multiple applications. Informed consent was obtained for everyone before the treatment, and information was given about the pros and cons of the alternative treatment options. The success of the ablation was evaluated clinically and technically. Clinical success was defined as remission of the pain after a single RFA within 1 month of therapy. Technical success was defined as the ability to localize the nidus and to insert the probe of the radiofrequency (RF) device into the nidus under CT guidance with ablation performed for the recommended time frame.
Numeric rating scale (NRS) was used to quantify pain and performed before and 4 weeks after the intervention for each patient. The diameter of the nidus and the adjacent edema was also recorded before and after the procedure. The follow-up interval until the last visit and presence of recurrent disease or subsequent therapies needed were also recorded.
All RFAs were performed by a single experienced interventional radiologist. Antibiotic was started for all patients for prophylaxis. CT was used to see the exact location of the lesion, follow the needle tract, and confirm the final position of the RF probe. A cannulated bone marrow biopsy needle (11 g for adults and 15 g for children) was drilled into the center of the nidus using a hand drill (Arrow on Control, Teleflex, Morrisville, North Carolina, USA). RFA probe (17 G, 17-15V05-30X) which is cooled with cold isotonic solution up to the tip was inserted into the nidus of the osteoid osteoma through the biopsy needle. The tines were opened and confirmed to be within the lesion with check CT sections. During ablation, RF waves from RF generator (Viva Generator, STARmed Co., South Korea) were used. The nidus was ablated with an RF probe (at 90°C for 6 min). After 6 min (in some cases longer or shorter depending upon the size of the lesion), the tines were withdrawn into the probe, and then, the RF probe was removed. The patient was discharged within the same day if there was no intervention-related complication. The prophylactic antibiotics were ordered to be taken 7 more days after ablation.
Statistics
Statistical analyses were performed using SPSS version 25 (SPSS Inc., Chicago, Illinois, USA). Saphira Wilkins test was used to check whether the variable had normal distribution. Descriptive analysis was presented as mean ± SD or median (min–max) where appropriate. The nonparametric Kolmogorov–Smirnov test was used to compare samples with the reference probability distribution, whereas the homogeneity of the variances was assessed using Levene’s test. Nonparametric Friedman test was used to compare initial and last measured volumes and longest axis of the nodules before and after intervention. The value of p < 0.005 was accepted as statistically significant.
Results
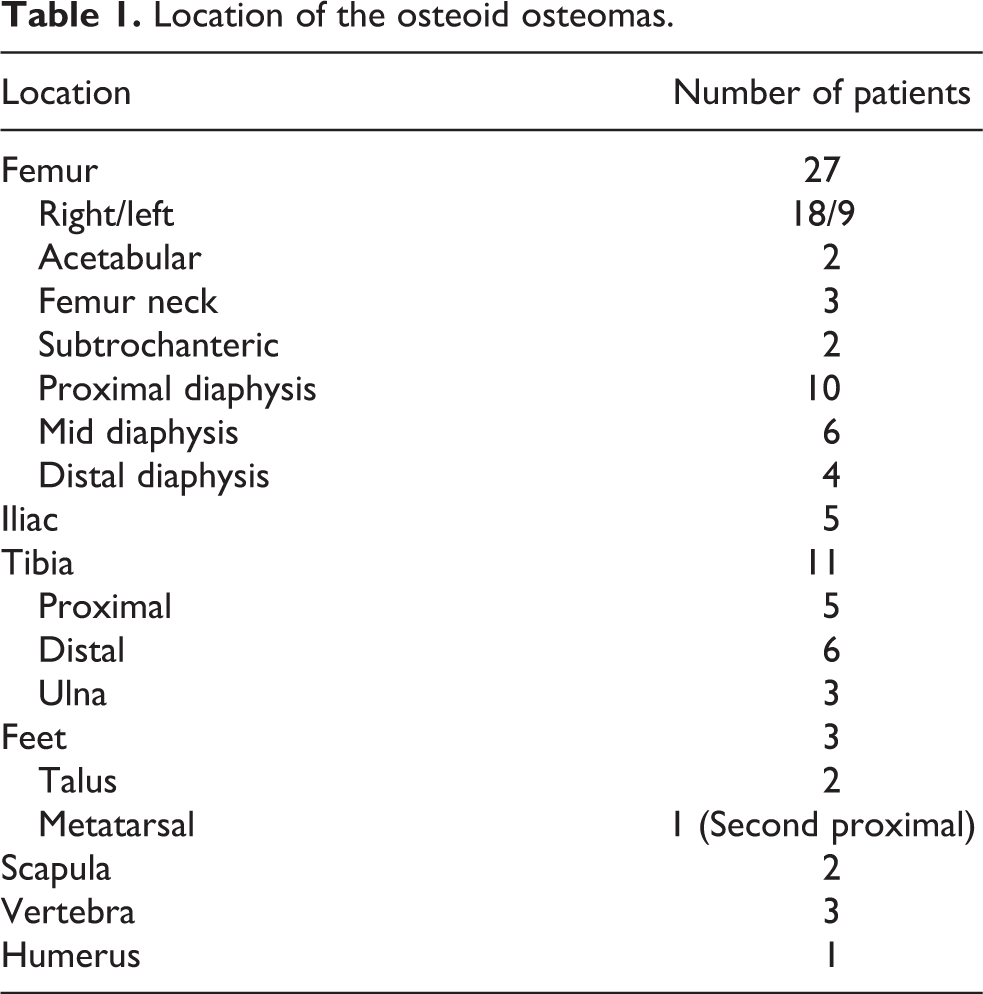
We enrolled 55 patients with osteoid osteomas. The locations of the osteoid osteomas are listed on Table 1. Of the 55 lesions, 27 were in the femur; 18 of them were on the right femur, whereas 9 were on the left. The most common location of the tumor on femur was the proximal diaphysis. The other involved locations in the femur were neck, acetabulum, and subtrochanteric regions. Eleven of the osteoid osteomas were located in the tibia, six of them were on the right, and the rest were on the left side. There were three ulnar lesions, three vertebral lesions, and one lesion in the humerus (Figure 1). One of the vertebral lesions was in the L3 facet (Figures 2 and 3). There were two scapular lesions (Figure 4) both on the right side. There were five osteoid osteomas in the iliac bones and three in the feet (two talus and one metatarsal) (Figure 5). One patient had an osteoid osteoma with double nidus (Figure 6). The mean age was 18.5 ± 9.6 years. The youngest patient was 5 years old, whereas the oldest was 50 years. Thirty-eight patients were male (69%) and 17 were female (31%). In all, 32.7% (18) had only CT, 40% (22) had only MRI, and 27.3% had both CT and MRI as the preintervention diagnostic imaging. None of them required biopsy. Pre- and postintervention NRS could not be obtained from six children who were younger than 10 years of age. Preprocedural mean nidus diameter was 3.59 ± 0.7 mm. Postintervention maximum nidus diameter was 2.1 ± 0.5 mm. The difference between pre- and postprocedure nidus size was statistically significant (p < 0.001) (Table 2). There was medullary edema in 54.5% of the patients. The median preinterventional maximum edema diameter was 18.5 mm (9–25), and the median postintervention maximum diameter was 6.5 mm. 2 –10 The difference was statistically significant (p < 0.001) (Table 2). Technical success rate was 98.1%. RF needle could not be replaced in the nidus in one patient since the family did not accept general anesthesia, and the patient was mobile during the whole procedure because of pain despite the maximum safe dose of sedatives. Clinical success was 96.36% since two patients required more than one session of RFA. Preintervention mean NRS score for pain was 8.4 ± 2.6, whereas postintervention mean NRS was 3.2 ± 1.18, and the difference was statistically significant. The median follow-up was 22 months (min–max; 8–56) (Table 2).
Location of the osteoid osteomas.

Osteoid osteoma on humerus (a) before and (b) during RFA. RFA: radiofrequency ablation.
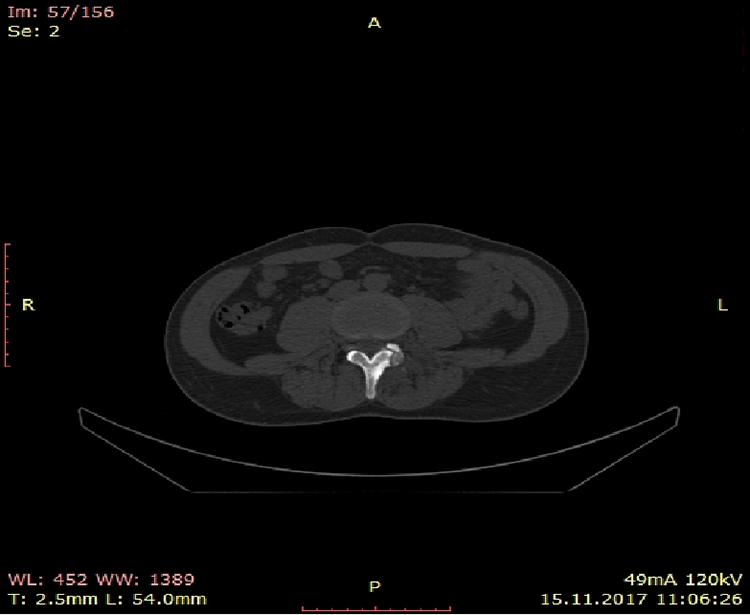
Osteoid osteoma on facet vertebrae.

Scintigraphy of osteoid osteoma on facet vertebrae.

Scapular osteoid osteoma (a) before and (b) during RFA. RFA: radiofrequency ablation.
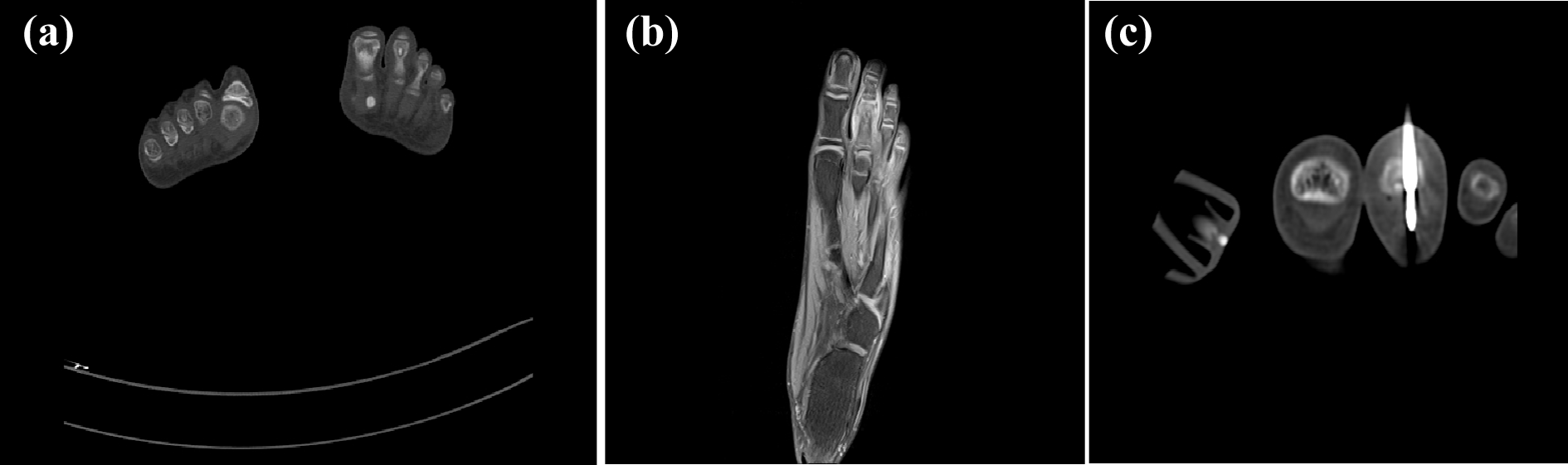
Osteoid osteoma on metatarsal before and during RFA. RFA: radiofrequency ablation.

Appearance of osteoid osteoma with double nidus in femur before and during ablation.
Pre- and postablation values and comparisons of nidus diameter, NRS, and edema.
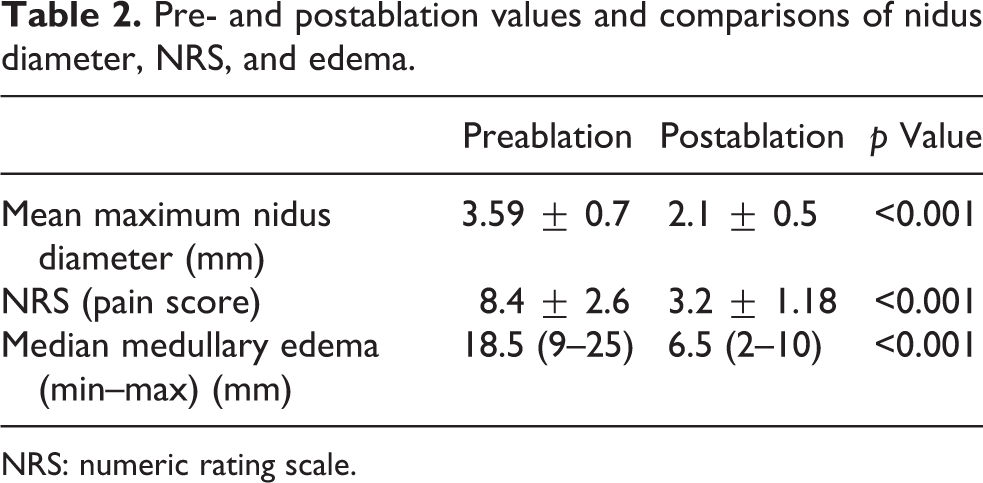
NRS: numeric rating scale.
In an adult female patient with a lesion on tibia, there had been skin and soft tissue burns throughout all needle tract (Figure 7). That was the only serious and severe complication of all. That happened because the trocar was overheated due to a technical problem. The patient was hospitalized and received intravenous antibiotics due to osteomyelitis. The wound then was closed with a flap. None of the patients developed temporary or permanent neurological deficits, and there was no intervention-related mortality in our study. RFA was well tolerated with mild complications such as transient pain after operation or anesthesia-related complications.

Severe burn and soft tissue defect due to RFA of the osteoid osteoma in tibia. RFA: radiofrequency ablation.
Discussion
Osteoid osteomas are well described and known benign tumors characterized with a translucent nidus. The primary imaging technique is CT which can easily detect the nidus and dense sclerotic reaction. 9 CT is better than MRI for tumor localization, whereas MRI has the advantage of better demonstration of osteoid osteomas in cancellous bones and showing adjacent intramedullary edema. 10 In our cohort, most of the patients had CT as the primary diagnostic test and only 40% had MRI. Positron-emission tomography (PET)/CT using F-18 and fluoro-deoxy-glucose may have a role in the diagnosis and posttreatment response evaluation. 11 The nidus exhibits avid glucose metabolism, whereas surrounding sclerosis does not. None of the patients had PET examination in our study group but five had bone scintigraphy.
Intra-articular osteoid osteomas including femoral neck can be particularly difficult to diagnose with routine radiography because of the relative absence of sclerotic reactions and absence of periosteal reaction. 1 The differential diagnosis of osteoid osteomas includes Brodie abscess, stress fracture, chondroblastoma, and osteoblastoma. 9 In addition to that, the bone density may be decreased because of disuse of the extremity due to pain which can lead to misdiagnosis of osteomalacia. However, in osteomalacia, demineralization is diffuse, trabecula is coarsened, there may be fractures defined as “looser zone,” and there are biochemical findings such as low calcium, increased parathyroid hormone, and low vitamin D levels. 12 Routine biopsy is not performed by most centers before the procedure due to the high specificity of imaging techniques. Even if an osteoblastoma is misdiagnosed as an osteoid osteoma, there is no inconvenience to treat such a lesion with RFA. The only exception can be Brodie’s abscess which requires antibiotic treatment. Another issue is the substantial percentage of nondiagnostic biopsy findings in osteoid osteomas regardless of the sampling technique of the nidus. 12
The treatment options for osteoid osteomas include observation, surgery, or minimally invasive techniques such as RFA. They can be treated conservatively by observation only because the pain is reduced with NSAIDS and the lesion may resolve with time. 13 Surgery was used to be performed frequently in the past that included removal of the nidus and allografting. 14 It is difficult to localize the lesion during operation and surgery is associated with significant morbidity afterward, especially in challenging locations such as the acetabulum or glenoid. 15 Since it was first reported to be successful by Torriani and Rosenthal, RFA has been used widely in the treatment of osteoid osteomas. 10 RFA is performed using a generator as the source of the current and it is directly delivered into the lesion by the probe. The tip of the probe is not insulated. The yielded energy and heat may damage the surrounding tissue which may cause coagulation necrosis. This happened in one of our patients causing months of hospital stay. Fortunately, this complication is rare, and the overall safety of the procedure is excellent.
The clinical and technical success rates in our cohort were 96.3% and 98%, respectively, which are compatible with the literature reporting success rate approaching 100%. 16 Only two patients needed an extra session of RF and ablated completely at the second sequence. In the literature, the recurrence rate varies between 7% and 16%, but during the median follow-up of 18 months none of our patients experienced recurrence. 17 The NRS score for pain significantly reduced after RFA. We performed the ablation under CT guidance, but it can also be made with fluoroscopy or MRI. Compared to MRI, CT-guided RFA has advantages including the highly resolved visualization of bone structures and rapid frame rate, allowing treatment under real-time fluoroscopy. 18
The cost of osteoid osteoma RFA in our country is €484 including sedation if the patient is discharged at the day of procedure. The cost is relatively lower compared to other European countries with the lowest cost reported as €655.5 excluding anesthesia, infrastructure, and equipment. 13 There is no cost-effectiveness analysis comparing surgery and RF in our country, but the expense is estimated to be higher in case of surgery due to operation charge, prolonged hospital stays or possible intensive care unit need, and higher recurrence rates and associated subsequent treatments. 3
One advantage of our cohort was having atypical cases such as scapula, metatarsal, and vertebral facet involvement. The metatarsal involvement on toe is rare with few published cases. 19 To the best of our knowledge, there is no reported case of facet vertebrae involvement. Vertebral osteoid osteomas can be a clinical challenge since it is hard to diagnose and treat without compromising function. 20 In our three cases with vertebrae involvement, the ablation was successful without any complication. Scapular osteoid osteoma is also very rare and usually dismissed in the differential diagnosis of shoulder pain. They can be confused with rotator cuff pathologies which occur in older patients. 21 There was a patient with double nidus in our cohort which is also rare with approximately 20 cases in the literature. 22 Another advantage of our study was its prospective design and demonstrating efficacy and safety in both adult and pediatric patients. In our study, 12 of the patients were younger than 18 years old and the rest were young adults.
In conclusion, RFA is safe and effective in both pediatric and adult patients with rare complications even in challenging cases with atypical locations.
Footnotes
Authors’ note
The study was carried out in Ankara City Hospital, Ankara, Turkey.
Acknowledgments
All of us have made a substantial contribution to the information submitted and have read the final manuscript. We have no direct or indirect commercial, financial incentive associated with publishing this article. Each of us acknowledges that he or she participated sufficiently in the work to take public responsibility for its content. We thank the staff of interventional radiology department for assisting us during the ablation procedures and helping us recording all needed data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.