
Abstract
Purpose:
Patients with von Willebrand’s disease (VWD) have either a qualitative or quantitative deficiency in a key clotting protein called von Willebrand’s factor. Type Ⅰ disease is the most common variant, but its clinical implications in total hip arthroplasty (THA) are unclear. Our purpose is to describe the perioperative impact of VWD in THA.
Methods:
We retrospectively reviewed a total of 17 primary THAs in 14 patients with type Ⅰ VWD performed between 2008 and 2019. Almost all cases (88%) received tranexamic acid, and most (59%) received DDAVP. All patients had a direct anterior approach (DAA) THA.
Results:
None of these cases required a blood transfusion. Mean estimated blood loss was 229 mL, and the mean hemoglobin dropped from 13.9 g/dL to 10.2 g/dL. There were no major bleeding complications. After a mean follow-up of 4 years, the mean hip disability and osteoarthritis outcome score, junior (HOOS, JR) was 79, and there were no reoperations or revisions for any cause.
Conclusion:
Patients with type Ⅰ VWD do not experience severe bleeding with routine chemoprophylaxis combined with DAA THA.
Introduction
Von Willebrand’s disease (VWD) is an inherited disorder that increases the risk of bleeding after surgery. First recognized in 1926, it is characterized by a quantitative or qualitative deficiency of von Willebrand factor (VWF). 1 VWF is a key clotting protein that binds to platelets in damaged endothelium to commence initiation of platelet plug formation. This is among the first steps in clot formation. In circulation, VWF is bound to factor Ⅷ. 2
In understanding the perioperative risk, VWD is often linked with hemophilia under the class of coagulopathies. Both diagnoses involve factor Ⅷ. However, their pathophysiology, clinical implications, and management are different. Hemophilia A is a potentially severe disease characterized by factor Ⅷ deficiency of varying degrees. The degree of bleeding complications correlates with the severity of levels. Major provoked bleeding and even spontaneous bleeding are common problems from an early age. There are over 50 orthopedic studies of hemophilic arthropathy, and appropriate perioperative management is well understood. In contrast, type Ⅰ VWD, while far more common than hemophilia, is comparatively less severe. This entity is caused by a reduction in functional VWF. To the best of our knowledge, there are no studies on the clinical significance of VWD type Ⅰ in total hip arthroplasty (THA).
A large database study of VWD, as well as hemophilia, in total knee arthroplasty (TKA) reported an increase in complications, revisions, and transfusions in the VWD cohort compared to controls. 3 Yet the prevalence and management of surgical risks of THA in this population remain unclear. In this retrospective case series, we explored the clinical course, complications, and outcomes of patients with type Ⅰ VWD who underwent direct anterior approach (DAA) THA.
Materials and methods
We retrospectively reviewed a total of 17 primary THAs in 14 patients with VWD performed between 2008 and 2019. All patients reported a history of type Ⅰ VWD. Patients with type Ⅱ or type Ⅲ VWD were excluded. Patients with associated blood dyscrasias such as thalassemia or iron deficiency anemia were also excluded. Surgery was performed by a single surgeon at a single institution with a minimum of 1-year follow-up. In all patients, a DAA THA with intraoperative fluoroscopy was performed. Charts were reviewed for indications, medical history, and hospital course. The primary outcome measures were bleeding complications, estimated blood loss (EBL), and postoperative transfusion of packed red blood cells (PRBC), specific VWF concentrate, or cryoprecipitate. Secondarily, hospital records were reviewed for other complications, reoperations, and rehospitalizations. Outcomes measured were patient-reported hip disability and osteoarthritis outcome scores, junior (HOOS, JR), revision, and death. 4 EBL and number of patients requiring transfusion were compared to a gender and age-matched control group of 17 patients without type Ⅰ VWD who underwent DAA THA by the same surgeon. The study was approved by the institutional review board.
For patients who were prescribed DDAVP or cryoprecipitate, the infusion was given preoperatively before the patient was brought to the operating room. The choice of general or neuraxial anesthesia was deferred to the anesthesiologist. Patients who received tranexamic acid (TXA) were given 1 g IV at the beginning of surgery.
Surgical technique
The patient was placed on the Hana table in the standard fashion. A standard DAA THA was performed as described by Matta et al. 5 For hemostasis, all visible vessels were suture ligated. Cell saver was made available. Intraoperative fluoroscopy was used to confirm implant sizing, orientation, and position. Postoperatively, the patient was allowed to proceed with weight bearing as tolerated (WBAT) and no other precautions. Given the potential hematologic complexity of these patients, the choice and duration of deep vein thrombosis (DVT) prophylaxis were deferred to the hematologist and hospitalist.
Statistical analysis
Mann–Whitney U test was chosen to determine statistical significance in EBL at the time of surgery in patients with type Ⅰ VWD versus patients without type Ⅰ VWD. The nature of the hypothesis testing was two tailed. Statistical significance was determined at a p value of less than 0.05 between groups. Data were analyzed using IBM SSPS statistics software, version 25.0.0.
Results
Of the 17 THA cases in patients with type Ⅰ VWD, 10 were left hips and 7 were right hips. Patients included 12 women and 2 men; 3 of the patients underwent staged bilateral DAA THA. The average age of patients at the time of index surgery was 61 years (range 40–79 years). The mean follow-up was 4 years (range 1–12 years).
Six of the patients presented with a clear bleeding history of epistaxis, menorrhagia, or excessive bleeding after surgery. The other eight had been diagnosed by laboratory findings. A hematologist was consulted in 10 cases prior to surgery. Cryoprecipitate was given preoperatively in one case and VWF concentrate (Humate-P) was given preoperatively in one case based on the recommendations of the hematologists. DDAVP was infused in 10 cases. TXA was given to all patients, except one (two hips) who underwent surgery in 2008 and 2010 before the routine use of TXA in orthopedics. This patient did receive DDAVP.
At the time of surgery, the average EBL was 229 mL (range 50–700 mL). The mean preoperative hemoglobin was 13.9 g/dL. The mean postoperative hemoglobin was 10.2 g/dL. There were no known bleeding complications. Cell saver was utilized in all cases, but a sufficient amount of blood for reinfusion was not available except in one case. This patient received 135 mL of cell saver blood intraoperatively. Cementless acetabular cups and femoral stems were used in all cases. There were no intraoperative complications. A summary of the results is provided in Table 1.
Results of 17 primary THAs in patients with type Ⅰ VWD.

THA: total hip arthroplasty; VWD: von Willebrand’s disease; TXA: tranexamic acid; EBL: estimated blood loss; VWF: von Willebrand factor.
Of the 14 DAA THAs performed in the comparative cohort of patients without type Ⅰ VWD, there were 10 left hips and 7 right hips. Patients included 15 women and 2 men. The average age of patients at the time of index surgery was 61 years (range 48–78 years). The average EBL at the time of surgery was 264 mL (range 100–500 mL). There was no significant difference in EBL (p = 0.5) or age (p = 0.9) between the two groups. A summary of the results can be seen in Table 2.
Comparison of EBL at the time of surgery and need for transfusion in age- and gender-matched groups undergoing DAA-THA with type Ⅰ VWD versus patients with without type Ⅰ VWD.

EBL: estimated blood loss; DAA: direct anterior approach; THA: total hip arthroplasty; VWD: von Willebrand’s disease.
No patient in either of the groups required an allogeneic transfusion postoperatively. In the group of patients with type Ⅰ VWD, the average length of stay was 2.7 days (range 1–7 days). The patient who required hospitalization for 7 days developed hyponatremia and pulmonary edema. This patient was diagnosed with syndrome of inappropriate antidiuretic hormone secretion (SIADH), a known side effect of DDAVP, and was managed medically until discharge. Another patient with leg swelling had a negative ultrasound 2 days after surgery. All patients were discharged to home.
At follow-up, the mean HOOS, JR score in patients with type Ⅰ VWD was 79 (range 39–100). The patient with a score of 39 had ankylosing spondylitis and was thus unable to differentiate hip pain from his overall disability. A preoperative HOOS, JR score was not available for comparison. One patient sustained a dislocation after a fall 3 months following surgery. The patient was closed reduced and has had no further dislocations after 2 years. There were no cases of revision or reoperation for any cause by the time of follow-up.
Discussion
VWD affects 1% of the US population and is the most common inherited bleeding disorder worldwide. 6 However, there is a paucity of data pertaining to its impact on orthopedic surgical outcomes. Its heterogeneity with respect to presentation and provoked bleeding severity, particularly in those with mild disease, may allow some cases to be unrecognized. This may predispose to excessive perioperative bleeding. For patients facing THA, it is essential to identify patients based on personal and family history. It is also important to characterize the VWD subtype. Although each subtype relates to an abnormality of VWF, the clinical implications are substantially different. There are three major subtypes. 7 Type Ⅰ is the mildest and most common and is inherited in autosomal dominant fashion. Type Ⅰ VWD accounts for 60–80% of VWD cases. It is characterized by a reduced circulating VWF level. Type Ⅱ accounts for 15–30% of cases and is characterized by a variety of qualitative defects of VWF and is subdivided into types 2A, 2B, 2M, and 2N depending on the presence of and behavior of larger VWF multimers. Symptoms are usually mild to moderate. Type Ⅲ is found in 5–10% of patients and is by far the most severe variant and is caused by marked reductions or absence of circulating VWF and bleeding is often quite severe with complications including spontaneous joint and muscle bleeding. 8 All patients in this study presented with type Ⅰ disease.
All of our patients presented to us with a prior history of VWD. Six patients (43%) described a clinically significant bleeding history citing epistaxis, menorrhagia, and excessive bleeding after surgical procedures or dental extraction. There were no cases of hemophilic arthropathy, as is commonly seen in hemophilia and the more severe coagulopathies. The remainder of our patients received a diagnosis in the absence of a specific bleeding history. As the type Ⅰ variant is an autosomal dominant condition, these patients sought and received a diagnosis after a warning from a family member who had been diagnosed with a bleeding diathesis. As previously noted, given the heterogeneity of type Ⅰ patients, we suspect some may have exhibited subclinical symptoms and were identified with routine screening. Hence, the actual number of our patients with subclinical type Ⅰ VWD disease may have been much higher.
In preparing for THA in our practice historically, the need for preoperative consultation by hematology or additional lab studies was deferred to the internist’s judgment. Most cases (59%) were evaluated by hematology preoperatively, and in these cases recommendations for presurgical DDAVP, cryoprecipitate, or VWF concentrate were made in all but one case. Eight patients (10 cases) received DDAVP, one patient received cryoprecipitate, and one patient received VWF concentrate. No patients were prescribed platelets. Our current protocol is to require all patients with a positive bleeding history or known type Ⅰ VWD to obtain a preoperative hematology consultation. A flowchart describing how a patient with type Ⅰ VWD is identified and prepared for THA in our practice is outlined in Table 3.
Flowchart to prepare patients with type Ⅰ VWD for THA.
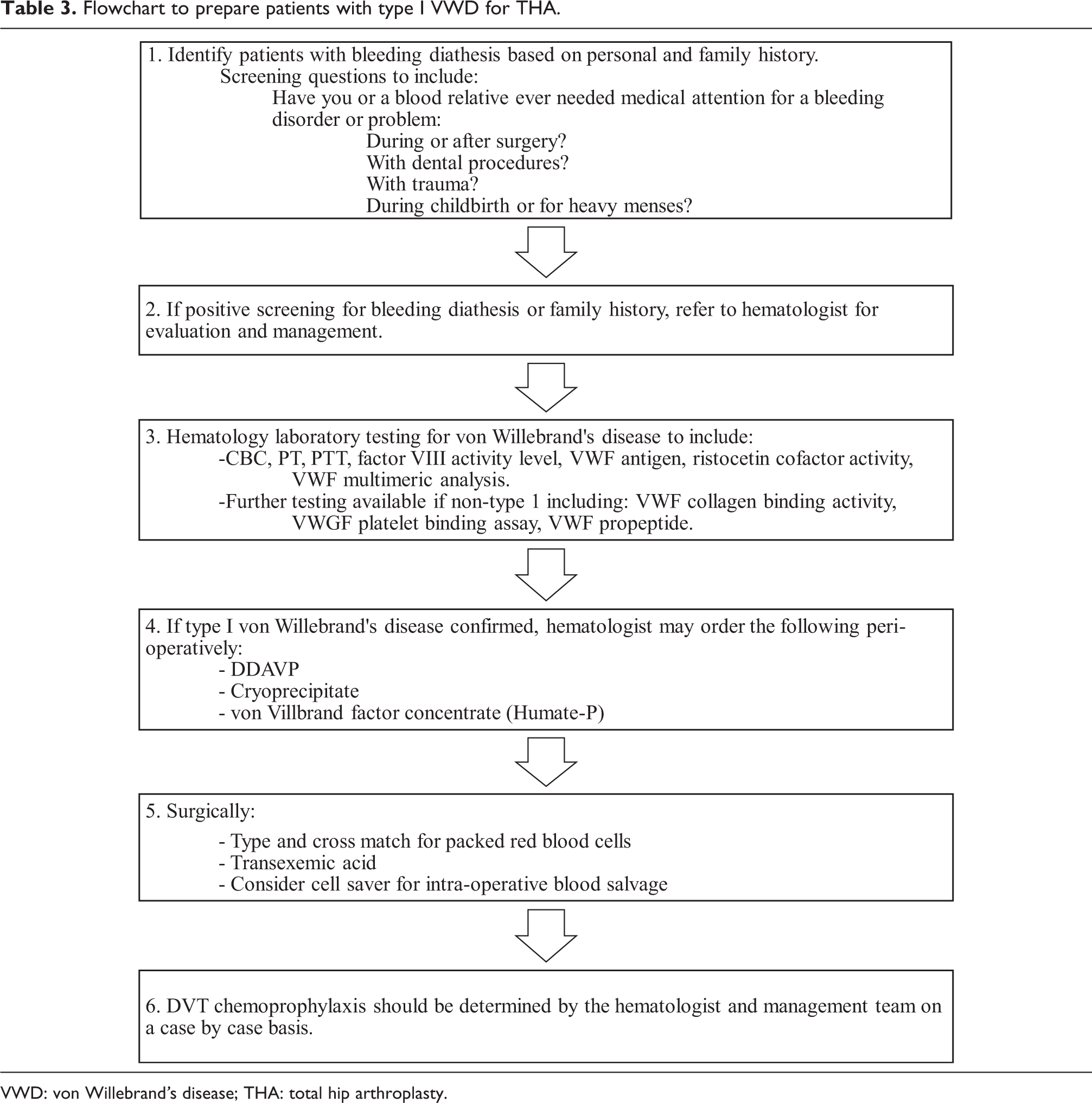

VWD: von Willebrand’s disease; THA: total hip arthroplasty.
Prior reports of arthroplasty in patients with bleeding disorders comment on the increased technical difficulty of surgery. 3,9 In a study of TKA, Solimeno et al. reported increased contractures and arthrofibrosis from recurrent intra-articular bleeds in hemophilia patients. 9 In contrast, our subgroup of patients did not have preexisting hip contractures or difficulties with exposure. To minimize bleeding, most patients (59%) received preoperative DDAVP, one patient received cryoprecipitate, and one received VWF concentrate as a precaution. All patients after 2010 received the antifibrinolytic agent TXA, and current guidelines support the use of TXA in patients with VWD. 10 With these protocols, there were no cases of major or uncontrolled bleeding, and the mean EBL was 229 mL.
The risk of transfusion would intuitively seem higher in patients with bleeding disorders. Up to 58% of patients with hemophilia are reported to need transfusion in TKA. 9 In the analysis by Cancienne et al., TKA patients with VWD had a transfusion rate of 32.8%. 3 Surprisingly, with the exception of one patient receiving 135 mL of cell saver blood intraoperatively, no patient in our series required a postoperative transfusion with PRBC, cryoprecipitate, or VWF concentrate. It should be noted that unlike those with hemophilia, all patients in this series presented with either mild or no anemia preoperatively.
Since 2014, the need for transfusions in THA overall in our practice has dropped substantially with the addition of TXA and with the removal of hemoglobin-based transfusion triggers below 10 g/dL. While six of the cases had a postoperative hemoglobin level less than 10 g/dL, these patients were managed with fluid and colloids to maintain orthostatic pressures. Blood transfusions would only have been given in a symptomatic and hemodynamically unstable patient unresponsive to fluid resuscitation.
After surgery, patients with VWD are reported to have more medical complications at 3 months. 3 In our series, there was only one postoperative complication in a patient who developed acute pulmonary edema and hyponatremia consistent with SIADH, as mentioned previously.
Prior studies also report an increased risk of implant failure and early revisions in patients with coagulopathy. 3 Figgie et al. proposed that aseptic loosening may arise from microbleeds at the bone–cement interface in cemented constructs. 11 In contrast, this same risk of failure may not apply to cementless ingrowth constructs used in this series and more widely used in THA overall. We reported no revisions or reoperations for failure at the follow-up.
Our most varied protocols arose in the management of VTE prophylaxis. As we deferred the choice of chemoprophylaxis to the attending hematologist or internist, it seemed there was no discernible pattern of medication. Patients who were on anticoagulation for a preexisting condition unrelated to VWD were restarted on that medication. Seven patients were given standard oral antiplatelet therapy, two received enoxaparin and two were treated with mechanical compression only. Regardless of the treatment protocol, we found no cases of pulmonary embolism or proximal DVT at the time of follow-up. In the absence of published guidelines to standardize thromboprophylaxis for these patients, treatment should be individualized by the hematologist based on the degree of VWF deficiency and clinical history. Further study of DVT prophylaxis in patients with type Ⅰ VWD is warranted.
The limitation of this study is that it is a single surgeon’s small retrospective series. Larger number of patients and longer follow-up may reveal a complication profile similar to that of other series. Although a minimum 2-year follow-up is more common, we chose a minimum 1-year follow-up to establish a greater pool for analysis, especially in perioperative complications. Finally, a preoperative HOOS, JR score was not available for comparison.
Conclusion
Unlike other severe coagulopathies, we found in our limited experience that type Ⅰ VWD is not associated with severe bleeding or an increased need for transfusions. Many patients present with a diagnosis in the absence of a personal bleeding history. Preventative management with hematology consultation, preoperative DDAVP infusion, and TXA may mitigate the risk of excessive blood loss. A DAA THA for these patients may also be of help in reducing bleeding and complications.
Footnotes
Data availability
Data is avaliable upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.