
Abstract
Purpose:
Computerized tomography (CT) imaging is increasingly being used to evaluate patients with ankle trauma. However, conventional CT (C CT) has a significantly higher radiation dose (RD) than plain radiography. This study aimed to evaluate the diagnostic accuracy and reliability of ultra-low-dose CT (ULDCT) protocol for ankle fractures.
Methods:
Ninety-eight consecutive patients who had ankle CT for suspected ankle fracture were included in our prospective study. C CT and ULDCT protocols were simultaneously performed on these 98 patients. Two observers independently evaluated ULDCT and C CT images. The effective RD of the ULDCT and C CT groups was calculated.
Results:
The interobserver agreement was 1 (perfect). ULDCT and C CT group images showed no significant difference in image quality. The effective RD of the ULDCT was significantly lower than the C CT (p < 0.001).
Conclusions:
By evaluating the results of this study, ULDCT proved to be a reliable diagnostic imaging method for fractures of the ankle. The satisfactory diagnostic image quality of the ULDCT protocol provides promising results.
Level of Evidence:
Level II/lesser quality RCT or prospective comparative study
Introduction
Ankle injuries are common injuries that account for more than 20% of injury patients admitting to emergency departments. 1 Ankle fractures which make up to 10.2% of all fractures have an increasing incidence of which is currently reported as 168.7 per 100,000 people per year. 2 Accurate diagnosis of ankle fractures in ankle injuries is crucial to prevent complications, such as osteoarthritis, persistent pain, and malunions, as even minimal residual displacement in ankle fracture results in an increased rate of complications and poor outcomes. 3 -5
Ankle injuries are typically examined radiographically after a physical examination if there is a concern for fracture. Plain radiographs have certain disadvantages like pain during positioning and providing insufficient data for diagnosis of subtle fractures, syndesmotic injuries, impaction of the medial tibial plafond, fractures of the posterior malleolus, and ankle fractures in adolescents and may provide insufficient data for the diagnosis. 6,7 Computerized tomography (CT) scanning in ankle injury provides an evaluation of the anatomic structures in more detail, especially in fractures with intra-articular expansion and with syndesmotic injuries. Thus, CT improves preoperative planning and intra- and postoperative reduction evaluation. 6,8 CT scanning is the golden standard option in all of the articular fractures other than ankle fractures. However, CT imaging is increasingly being used for the diagnosis of ankle fractures as well. 6,9,10
Conventional CT (C CT) has a significantly higher radiation dose (RD) than plain radiography. 11 Increasing RD is related to increased risk for radiation-induced cancer. 12 Ultra-low-dose CT (ULDCT) is the term which defines the massive reduction in RD with the use of novel reconstruction techniques without sacrificing the diagnostic image quality. 13 There are a limited number of studies, which evaluate the efficacy of ULDCT protocols in fractures of the extremities. 14,15
This study aimed to evaluate the diagnostic accuracy and reliability of ULDCT protocol for ankle fractures. With this aim, we have compared the diagnostic quality of C CT views and ULDCT images of patients with ankle fractures.
Material and methods
Patients
Between January and December 2019, a total of 142 consecutive patients were scheduled for ankle CT for suspected ankle fracture after trauma in our prospective study. Patients scheduled for ankle CT who were <18 years of age or pregnant were excluded from enrollment. A further three patients were excluded due to movement artifact during imaging. A total of 98 patients with suspected ankle fractures were included in the final analysis. Both the ankle CT protocols, including standard dose (120 kVp and 100 mAs) and ultralow dose (80 kVp and 5 mAs), were simultaneously performed on these 98 patients. CT images obtained from the standard dose were assigned to the C CT group (group 1) and CT images obtained from the ultralow dose were also assigned to the ULDCT group (group 2). All patients signed informed consent. The local institutional review board approved the study protocol. Informed consent was obtained from all individual participants included in the study. Patients signed informed consents on the conduction of diagnostic procedures and medical interventions. Ethical approval was obtained from the clinical ethical board of Ataturk University and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
CT acquisition protocols
All ankle joint CT examinations were performed on a 320-row detector CT (Aquilion ONE Vision; Toshiba Medical Systems Corporation, Otawara, Japan) in single volume mode with an acquisition in a single volume covering the ankle joint region. The ankle joint CT protocols for C CT and ULDCT groups were performed concurrently.
In group 1, the CT acquisition protocol was performed with the following parameters: 0.5-s gantry rotation time, 0.5 × 160 mm2 detector rows using a z-flying focal spot, 32-cm field of view (FOV), and 100-mAs tube current at 120 kVp tube voltage. In group 2, the CT acquisition protocol also performed with the following parameters: 0.5-s gantry rotation time, 0.5 × 160 mm2 detector rows using a z-flying focal spot, 32-cm FOV, and 5-mAs tube current at 80-kVp tube voltage. Patient position was supine with a slight reclination of the ankle joint to obtain a parallel alignment of the upper jaw to the gantry. The 1-mm axial, 1-mm coronal, as well as 1-mm sagittal images were reconstructed from the raw data set, using both bone and soft tissue kernels.
Image evaluation
All ULDCT and C CT images were transferred to a workstation (SyngoVia VB10B, Siemens Healthcare, Forchheim, Germany). ULDCT and C CT images of the same patients separated and named as different image sets. To eliminate the bias in evaluation of the images, views are presented to the observers in mixed image sets. Consequently, ULDCT and C CT images are selected from different patients (ULDCT images of the first patient, C CT images of the second patient, ULDCT images of the third patient, etc), and they are categorized as data set 1. The remaining ULDCT and C CT images (C CT images of the first patient, ULDCT images of the second patient, C CT images of the third patient, etc) are categorized as data set 2. One radiologist with 5 years of experience in musculoskeletal imaging and one orthopedic surgeon with 5 years of experience, respectively, were blinded to all clinical data and image type evaluated images on the workstation.
Two observers independently evaluated images for fracture diagnosis and image quality of the data. A five-point scale (1: not diagnostic, 2: limited diagnostic image quality with image noise and artifacts, 3: sufficient image quality, 4: good image quality, and 5: excellent image quality) score system used for image quality. 16 There was 2-weeks interval at least between the evaluation of data set 1 and data set 2 images to avoid observer bias. The fracture existence and diagnostic image quality score noted for each image set. The C CT images were used for gold standard imaging modality for detecting fractures and evaluating image quality. The presence or absence of fracture was decided by consensus by analyzing the C CT.
Estimation of effective radiation exposure
The effective RD of groups 1 and 2 was calculated due to utilization of a method proposed by the measurement, reporting, and management of RD in CT, which uses the dose–length product (DLP) and a conversion coefficient for the adult ankle (k = 0.0002 mSv/[mGy cm]). DLP values were derived from the patient protocol. 17
Statistical analysis
Statistical analyses were performed using SPSS 22.0 (SPSS Inc., Chicago, Illinois, USA). The χ 2 test was used to compare the categorical variables between groups 1 and 2. The sensitivity, specificity, and accuracy of ULDCT were calculated for two observers. We calculated interobserver agreements for all observers. An interobserver reliability analysis using the kappa statistic was performed to determine consistency among observers. The degree of agreement based on kappa values was as follows: <0, none; 0–0.20, slight; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, substantial; and 0.81–1.00, almost perfect. The p values <0.05 were considered to be statistically significant.
Results
There were a total of 98 patients in groups 1 and 2 (54 (55.1%) males and 44 (44.9%) females).
The effective RD which was calculated for the group 1 scans was 41.37 ± 1.85 µSv. The effective RD which was calculated for the group 2 scans was 0.47 ± 0.02 µSv. The effective RD of group 2 was significantly lower than group 1 (p < 0.001).
Two observers detected all fractures on ULDCT. The interobserver agreement was 1 (perfect) (Table 1).
The sensitivity, specificity, and accuracy of ULDCT based on observers.

CI: confidence interval.
Twenty-six patients had a fracture. We have detected distal tibial fractures in 11 of 26 (42.3%) patients, the distal fibular fractures in 7 of 26 (26.9%) patients, and talar fractures in 8 of 26 (30.8%) patients in our study (Figures 1 and 2).

(a) Ultralow dose and (b) standard coronal reformatted computed tomography images of 41 years old woman show two bone fragments (arrows) in the tibiotalar joint.
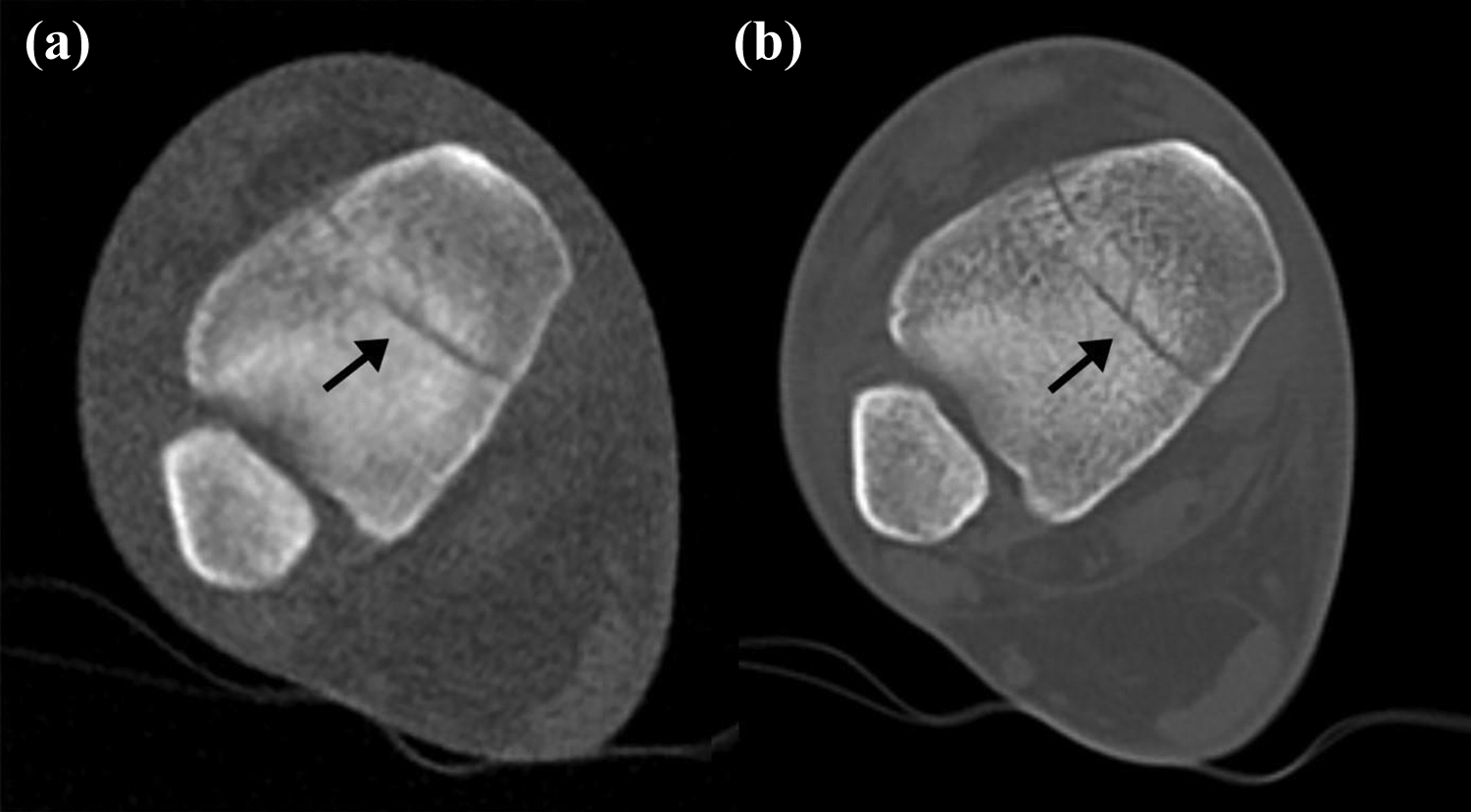
(a) Axial ultralow dose and (b) standard CT images of 45 years old man show fracture lines (arrows) in the tibia. CT: computed tomography.
We obtained an overall interobserver agreement of 0.84 (almost perfect agreement based on kappa values) in evaluating all the bony components of the ankle joint for observers 1 and 2. For observer 1, the lowest mean image quality score was 3.43 in evaluating the distal end of the fibula fracture in group 2. For observer 2, the lowest mean image quality score was 3.79 in evaluating the distal end of the fibula fracture in group 2. The overall mean image quality score was 3.69 for observer 1 and 4.63 for observer 2 in group 2; the overall mean image quality score was 4.39 for observer 1 and 4.97 for observer 2 in group 1. C CT and group 2 CT images showed no significant statistical difference in image quality. The image quality scores are summarized in Table 2.
The mean image quality scores and kappa values of study and control group for each observer.

ULDCT: ultra-low-dose computed tomography; C CT: conventional computed tomography.
Discussion
Ankle fractures having an incidence of 179/100,000 account for 9% of all adult fractures. 1,18 Ottawa ankle rules defined the indications for the use of radiography in ankle trauma. 19 The standard ankle series is composed of an anteroposterior, mortise, and lateral radiographs. In cases of suspected syndesmotic or ligamentous injury and subtle fractures, external and internal oblique views and stress views of the ankle can be included as well. 20 An increased number of X-ray views results in increased radiation exposure (mean single X-ray dose of 0.53 ± 0.43 μSv). 15 ULDCT (mean ULDCT dose 0.47± 0.02 µSv) protocol can provide satisfactory diagnostic data with less doses of radiation than multiple X-ray views. 15,18
In a recent critical review, Rammelt and Boszczyk recommended the use of CT imaging in malleolar fractures with unstable syndesmosis, fractures of the posterior malleolus, supination adduction type fractures with medial plafond impaction, spiral fractures of the distal tibia, and transitional ankle fractures in adolescents. 6 Alagic et al. compared digital radiography with ULDCT imaging in 207 extremities. In this article, ULDCT detected 36 additional fractures, 3 of which had surgical treatment, where digital radiography failed. Moreover, ULDCT also provided comparable RD with digital radiography. 15
We have found that ULDCT scanning is a reliable and accurate diagnostic option in radiologic evaluation of ankle fractures. We have obtained high levels of agreement for interobserver reliability regarding diagnostic quality. Also, we have obtained similar image quality scores to C CT. A 98% decrease in the effective RD was provided with the use of ULD-CT protocol compared to C CT in this study.
Voizard et al. reported 48.5% of change of initial diagnosis of the emergency department after orthopedic evaluation with further radiologic imaging in pediatric ankle trauma patients. 21 Also, Eismann et al. reported a significant rate of modification of the diagnosis after CT evaluation in pediatric triplane ankle fractures. 7 As misdiagnosis resulting in mismanagement of the fractures of the ankle causes an increased rate of morbidities, the aforementioned studies conclude that the evaluation of the ankle trauma patients with conventional radiography can cause misdiagnoses and the use of CT in ankle trauma is invaluable. ULDCT protocol used in this study having similar image quality with conventional CT can decrease the rate of misdiagnosis without increased radiation exposure.
The diagnosis of subtle fractures of the ankle requires CT scanning as the alternative magnetic resonance imaging is not cost effective. 6,22 However, CT has the essential disadvantage of increased radiation exposure. 6 New strategies are being employed to decrease effective RD in CT processing. Articles on ULDCT applications in various disciplines have been published recently. 23 Studies evaluating the use of ULDCT protocol in limb trauma reported successful results. 13 -15,24 The outcomes of our study were consistent with the recent literature.
The linear no-threshold theory states that increasing doses of radiation is directly proportional to an increase in the radiation-related risk of cancer. 25 Current evidence suggests that being exposed to 10 mSv of radiation increases the risk of malignancy with 1:2000. The pediatric population is more susceptible to radiation-related malignancies. Meulepas et al. reported a 1.5 times increase in overall cancer incidence in pediatric patients after the first CT. 26 Especially, polytrauma patients undergoing repeated CT scans have increased exposure to radiation. The ULDCT protocol performed in this series of patients provided almost 98% of the decrease to effective RD without compromising diagnostic quality.
There are several low-dose CT studies on fractures diagnosis in the literature. 15 Reviewing the recent studies, we have noticed that the mean RD in our study was significantly lower than the previous studies. 13 -15
The strengths of this study are its prospective design and evaluation of the same patients with different CT protocols. The limitation of this study is the relatively small number of patients. There are also several shortcomings of ULDCT, such as cost and limited scanning width. Novel techniques should be developed and studies should be done to eliminate these disadvantages.
Conclusion
Evaluating the results of this study, ULDCT proved to be a reliable diagnostic imaging method for fractures of the ankle. The satisfactory diagnostic image quality of the ULDCT protocol provides promising results. We do hope that the ULDCT protocol having almost the same effective RD with plain radiography will be the standard of care in ankle fractures in the future.
Footnotes
Acknowledgment
We would like to thank Prof Dr MT for assistance with statistical analysis and John Adam Brown for reviewing the article as a native speaker of the English language.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.