
Abstract
Purpose:
To evaluate the acetabular cup and graft survival in patients who underwent total hip arthroplasty (THA) with the diagnosis of dysplastic hip osteoarthritis and received a femoral head autograft due to acetabular coverage deficiency.
Methods:
Between January 2005 and December 2016, 83 hip prostheses of 80 patients who underwent THA using femoral head autografts and were followed up for at least 2 years were retrospectively evaluated. Seventy-four hips of the remaining 71 patients (57 female (80%)) were included. Mean patient age at surgery was 51 ± 16 (range 18–76) years. The mean follow-up duration was 76 ± 25 (range 25–161) months. Acetabular inclination and graft thickness, contact length, percentage of coverage, and graft resorption were examined on postoperative and final follow-up radiographs. The presence of a radiolucent area around the acetabular and femoral components indicating loosening was also evaluated.
Results:
The mean postoperative acetabular component inclination was 44 ± 5.1° (range 30–48°) with mean graft coverage of 34 ± 4.8% (range 24–46%). In all patients, autograft union with the pelvis was seen and the lateral overflow was remodeled. Fifteen patients (20%) underwent revision surgery due to aseptic acetabular component loosening in four, nontraumatic recurrent dislocations in eight, periprosthetic infection in one, acetabular component protrusion in one, and traumatic hip dislocation in one.
Conclusion:
In patients with osteoarthritis secondary to developmental hip dysplasia, the use of femoral head autografts to eliminate acetabular coverage deficiency during THA achieves acceptable midterm postoperative radiological outcomes. Increased acetabular bone stock may be beneficial in possible future revision surgeries.
Introduction
In cases of hip osteoarthritis with developmental hip dysplasia, total hip arthroplasty (THA) poses technical difficulties due to dysplastic changes in the acetabulum and femur. 1 In patients with acetabular bone stock deficiency due to developmental hip dysplasia, placing the acetabular component in its true location during total hip replacement and achieving adequate bone coverage is difficult. 2 A femoral head autograft is commonly used in clinical practice to provide superolateral coverage of the acetabulum. Gerber and Harris found radiographic loosening in the seventh postoperative year in 21% of their patients treated with femoral head autografts. 3 Hampton and Harris later published that uncemented acetabular cups performed very well. They reported a 92% survival rate in an average of 16-year follow-up. 4 Over the last few decades, with advances in bone graft techniques, favorable results have been reported and the technique has become more important. However, few studies have evaluated the outcomes of THA in patients with dysplastic hip osteoarthritis using femoral head autografts combined with cemented or noncemented implants (Table 1). 5 –10 Therefore, this study aimed to radiologically evaluate the acetabular cup and graft survival during short- and medium-term follow-up of patients with dysplastic coxarthrosis who underwent THA and received a femoral head autograft due to acetabulum coverage deficiency.
Comparison of publications related to total hip arthroplasty combined with femoral head autograft.
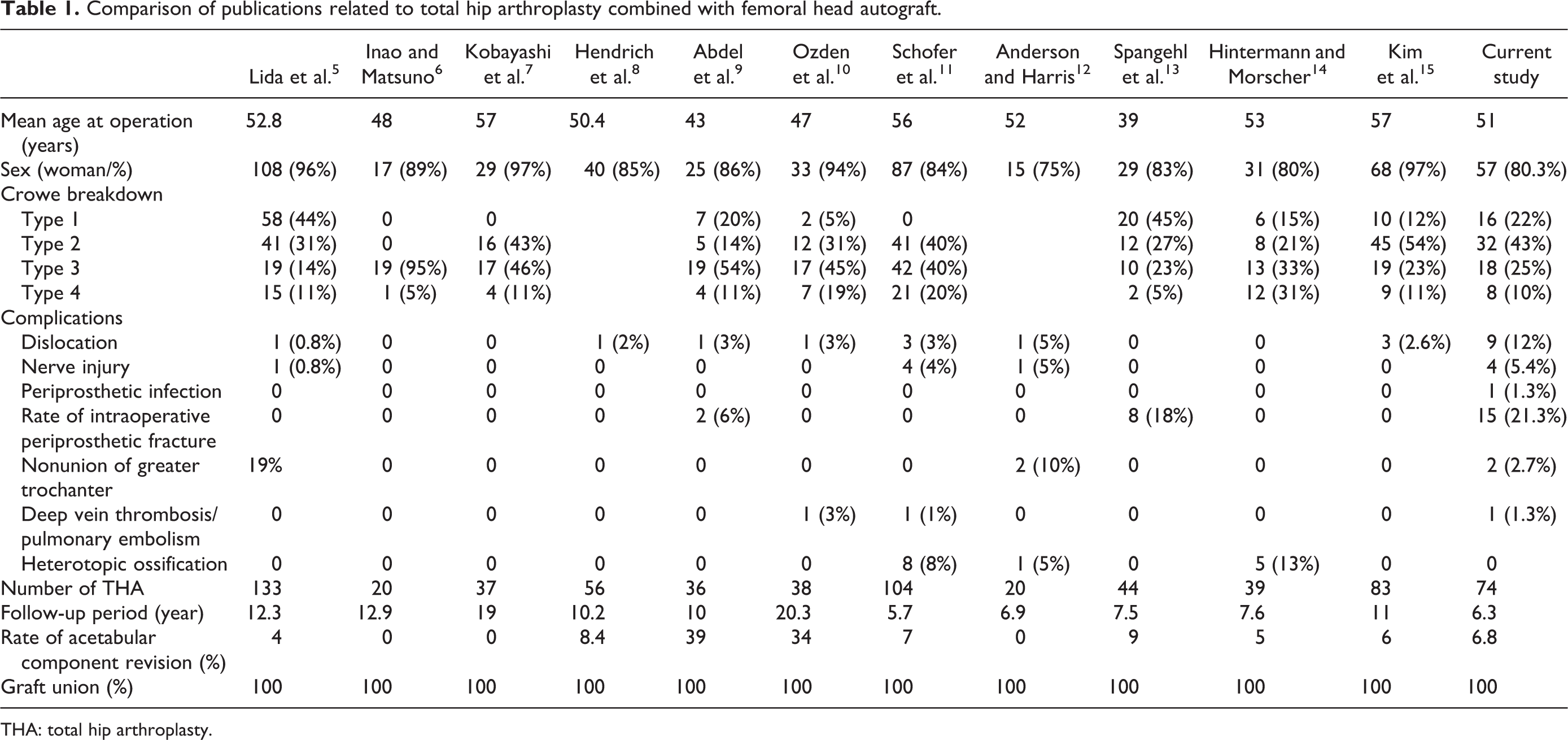
THA: total hip arthroplasty.
Materials and methods
This study was performed at a training and research hospital. After obtaining hospital ethics committee approval, 80 patients (83 hips), who underwent THA using a femoral head autograft between January 2005 and December 2016, were retrospectively evaluated. Nine patients were excluded: two with a history of trauma as an etiologic factor, two who died of non-THA reasons, and five who did not attend the follow-up sessions. A total of 74 hips of the remaining 71 patients were included in the study.
During the surgery, the acetabular component was ideally placed in the acetabulum, and THA was performed. In cases in which a 20% coverage deficiency was detected in the acetabulum, a femoral head autograft was applied. The degree of acetabular dysplasia was determined, as described by Crowe et al. 16 (Table 1). A cemented acetabular component was used in three of the 74 hips, whereas a noncemented acetabular component was used in the other 71 (Figure 1). A noncemented femoral component was used in all hips. For graft fixation, two screws were used in 53 hips, whereas three screws were used in the other 21 hips. The primary outcome that we measured was radiologic measurements. Complications and revision rates were evaluated as secondary outcome measures.

A 63-year-old female patient. Noncemented acetabular and femoral components were used in the left hip. (a) Preoperative, (b) early postoperative, and (c) latest (36 months) follow-up radiographs.
Radiological evaluation
Patients were called for clinical and radiological follow-up on the 15th postoperative day, 6th week, 3rd month, 6th month, 12th month, and annually thereafter. Standardized pelvic, hip anteroposterior (AP), and hip lateral radiographs were taken in the supine position to evaluate the femoral stem and acetabular component in outpatient controls. Follow-up radiographs were compared with the baseline immediate postoperative radiographs. In the early postoperative period, the inclination angle of the acetabular component and percentage of the graft coverage of the acetabular component was measured. The graft coverage percentage was determined as the ratio of the length of the portion of the component in contact with the graft to the total length of the acetabular component in contact with the graft and acetabular bone (Figure 2). 17,18

Reconstruction of the acetabulum with femoral head autograft x: Percentage of coverage of the graft on acetabular component: % (distance from b to c)/(distance from a to c), y
Graft resorption was evaluated by measurement of its mediolateral width and superior–inferior length on the early postoperative radiographs and pelvic and hip AP radiographs taken at the last follow-up. The stability of the acetabular component was assessed using the criteria described by DeLee and Charnley 17 and Callaghan et al. 19 for the radiographic evaluation of component loosening: changes in component position, migration, broken screws, and a complete radiolucent area of ≥2 mm at the bone–implant interface. The need for acetabular component revision was defined as clinical failure.
Surgical technique
The operations were performed by two experienced arthroplasty surgeons. A posterolateral incision was used in all patients. Because the walls of the acetabulum were weak and the medial stock was small, controlled reaming was performed. The acetabular superolateral defect was evaluated after the insertion of a trial acetabular cup. In cases in which a femoral head autograft was to be used, the acetabular host region and femoral head autograft were prepared.
A reamer and curette were used to show the bleeding of the sclerotic area in the superolateral wall, and viable tissue was reached. The resected femoral head and neck were divided into two pieces considering the defect size. Chondral surfaces of the femoral head and host region were removed. In the host acetabulum site and autograft surface, chondral and cortical tissues were removed. To promote graft union, the iliac bone was prepared with multiple drillings to obtain a bleeding bone bed. The autograft was then inserted and fixed with two or three screws.
A Pinnacle® Acetabular Cup System (DePuy Synthes Joint Reconstruction, Warsaw, Indiana, USA) in 23 (31%) patients, a Trilogy® Acetabular Hip System (Zimmer Inc., Warsaw, Indiana, USA) in 14 (19%) patients, a Harris-Galante-II® (Zimmer, Inc.) in 12 (16%) patients, and a Reflection® cup (Smith & Nephew, Memphis, Tennessee, USA) in 22 (30%) patients were used. Longevity® Highly Crosslinked Polyethylene liner (Trilogy Longevity; Zimmer, Inc.) in three (4%) patients (cemented acetabular components) were used. The cemented cup was preferred due to obtaining adequate stability. Highly cross-linked polyethylene liners were used in patients older than 65 years old. Delta ceramic liners were used in patients younger than 65 years old. Uncemented tapered wedge femoral stems were used in all patients. The M/L taper stem® (Zimmer Inc.) in 40 (54%) patients, the TRI-LOCK® stem (DePuy Synthes Joint Reconstruction) in 23 (31%) patients, and the Anthology® stem (Smith & Nephew, London, UK) in 22 (30%) patients were used.
Postoperative follow-up
Isometric quadriceps exercises were started on the first postoperative day, followed by active straight leg lifting and hip and knee exercises on the second postoperative day. Patients who did not have intensive pain and had a normal arterial blood pressure were encouraged to sit on the side of the bed as soon as possible. After the drains were removed within 24–48 h postoperatively, all patients were mobilized with the help of a physiotherapist without weight bearing on the operative side. Weight-bearing was restricted until 6–8 weeks postoperative. Next, partial weight-bearing was permitted and gradually increased. Full weight-bearing was allowed in the 10th postoperative week.
Statistical analysis
All analyses were descriptive. Patient characteristics are summarized as mean, standard deviation, percentage, lowest, and highest. All data sets were parametric in distribution.
Results
The mean patient age was 51 ± 16 years (range 18–76 years). Fourteen patients (20%) were men and 57 (80%) were women. The mean follow-up duration was 76 ± 25 months (range 25–161 months). Patient demographics are summarized in Table 2.
Patients’ demographics data.
In the early postoperative radiographic controls, the acetabular component angle (inclination) ranged from 30° to 48° with a mean value of 44 ± 5.1°. The mean acetabular cup diameter was 49 ± 13 mm (range 40–60 mm).
During follow-up, the early postoperative and final radiographs were compared to determine the displacement of the acetabular component in the horizontal and vertical directions. Acetabular cup migration was observed in a total of nine patients (12%): both vertically and horizontally in four (5.4%) and only vertically in five (6.7%). The mean vertical migration value was 3.7 ± 1.2 (range 1–8 mm), and the mean horizontal migration value was 1.5 ± 0.3 mm (range 1–2 mm).
When the acetabular component was evaluated according to the radiological zones defined by DeLee and Charnley, radiolucent areas were seen in a total of five hips (6.8%). Radiolucency of ≥2 mm was detected in all zones in four hips (5.4%) and only in zones 2 and 3 in one (1.4%).
The percentage of the graft covering the acetabular component was 34 ± 4.1% (range 24–46%). The coverage percentage of the acetabular component was 44–83% (mean 66%). The mean length of the contact area between the graft and host bone was 34 ± 5.3 mm (range 13–52 mm). The mean graft thickness was 29 ± 4.6 mm (range 10–52 mm) (Figures 3 and 4).

The diagram shows graft coverage and length of the contact area between the graft and host bone.
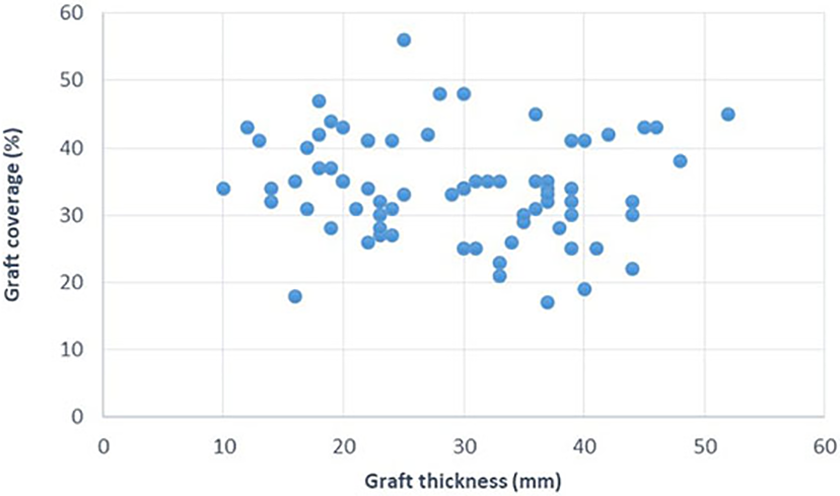
The diagram shows relationship graft coverage with graft thickness.
In the evaluation of the radiolucent areas around the femoral component, only one hip showed a 2-mm migration of the femoral component, which was not clinically significant when evaluated together with the remaining radiological parameters and patient’s clinical state.
Complications
As given in Table 1, 16 perioperative and 20 postoperative complications developed.
Fracture
The periprosthetic acetabular fracture occurred in one patient (1.3%) during surgery. The periprosthetic femoral fracture occurred in 15 patients (20%). The M/L taper stem (Zimmer Inc.) was used in seven patients, a TRI-LOCK stem (DePuy Synthes Joint Reconstruction) in five patients, and an Anthology stem (Smith & Nephew) in three patients. Vancouver type-A periprosthetic femoral fracture was developed in 5 patients (33%), while Vancouver type B fracture was developed in 10 patients (67%). Open reduction and internal fixation were performed in all patients intraoperatively. Locking compression plates were performed in 4 patients (23%) and Dall-Miles cables (Stryker, New Jersey, USA) were performed in 11 patients (77%). Fracture union was observed in all patients.
Infection
Three of the postoperative complications were related to infections. Discharge at the wound site occurred in two patients in the early postoperative period; these patients were treated within 2 weeks without any radical intervention other than superficial debridement and intravenous antibiotic treatment. One patient underwent two-stage revision hip arthroplasty with the diagnosis of periprosthetic infection.
Dislocation
Early postoperative dislocation occurred in nine patients (12%), in whom closed reduction was performed. Acetabular component loosening (two patients), malposition of the acetabular or femoral component (three patients), impingement (three patients), and abductor arm insufficiency (one patient) were found to be responsible for dislocations.
Nerve palsy and pulmonary thromboembolism
Intraoperatively, sciatic nerve palsy developed in four patients. Three of these patients achieved complete recovery of the sciatic nerve, whereas the other showed no improvement with the use of an ankle–foot orthosis at the 2-year follow-up; thus, a tendon transfer was planned. Exploration was not performed in any of the patients. One patient developed pulmonary thromboembolism, for which medical treatment was performed.
Revision
Revision surgery was required in 15 of the 74 hips for the following reasons: nontraumatic hip dislocation in eight patients (three patients with Crowe type 2 dysplasia, one patient with Crowe type 3 dysplasia, and four patients with Crowe type 4 dysplasia), aseptic loosening of the acetabular component in four patients (three cementless and one cemented cups), late traumatic hip prosthesis luxation in one patient, and periprosthetic infection in one patient. Also, protrusion and rotation of the acetabular cup due to no ingrowth were developed in one patient. The time to revision surgery ranged from 7 days to 136 months.
Discussion
In this study, no radiological findings of graft nonunion or failure were observed at the final follow-up. Graft union was observed in all patients at 3–9 months postoperatively. If a part of the femoral head autograft protruded from the superolateral corner of the acetabular component, this unloading part was resorbed over time. Resorption of the lateral bone graft (graft remodeling) protruding over the unloaded part of the acetabular component was limited to the lateral edge of the graft alone, and no loosening of the component due to graft resorption was seen in the load-bearing area. During the revision surgery, the previously implanted autografts were confirmed viable and facilitated the placement of the new acetabular component. No additional graft or metal augment was needed in the revision cases.
In the literature, results related to the use of bone autografts vary, which has been attributed to differences in patient selection, degree of dysplasia, patient age and bone quality, grafting technique, graft coverage percentage, and choice of the component. 20 –22 The use of high hip center technique provides an attractive alternative for reconstruction of the deficient acetabulum. Excellent outcomes, as shown by a minimum 10-year follow up, were accomplished with the high hip center placed by different authors. 23,24 In elderly patients, probably a high hip center could be used. Although this technique is not used in this series, it should be kept in mind in elderly patients. Femoral head autografting for hip dysplasia could be preferred when dealing with young patients with secondary arthritis with dysplasia to restore bone stock.
Excellent survival at 15 years has been reported by Kim and Kadowaki 15 with 94% long-term survival of bulk femoral head autografts in cementless THA for Developmental dysplasia of hip (DDH). The result led them to speculate that the high rate of graft incorporation and survival could be attributed to three factors: initial stability of the graft and cup, impacted cancellous surfaces of the host and graft, and a porous surface of the largest possible cups. In our study, a high graft incorporation rate was obtained. Although the total survival was not very high, no patients underwent revision due to graft-related complications.
In a series of Mulroy and Harris, the aseptic loosening rate was 67% in patients who had ≥40% graft coverage (40–70%) of the cemented acetabular component and 21% in those who had <40% graft coverage (20–40%). At least 70% of the acetabular component should be covered by the host bone to ensure stability. 25 Kobayashi et al. 7 suggested that the graft’s coverage of the socket should not exceed 50%. Rodriguez et al. 26 emphasized that the graft coverage rate of the acetabular component should be <40% and noted that in their study, graft viability and integrity were maintained and the main reason for the loosening of the graft was the failure to properly fix the components. In our series, examining the relationship between aseptic loosening and autograft fixation and coverage size, the two patients whom we suspected of having aseptic loosening had a graft coverage of 40%; in one of them, percentage of the acetabular component covered by the autograft was 48%, two screws were used for graft fixation, and follow-up revealed a radiolucent area of ≥2 mm in zones 2 and 3 around the acetabular component as well as vertical and horizontal acetabular cup migration. In the last session, this patient presented with no symptoms; thus, revision surgery was not necessary, and outpatient follow-up was recommended. In the other patient, the percentage of the autograft coverage was 47% and the graft had been fixed using three screws. During follow-up, revision surgery was performed 51 months postoperatively due to symptomatic acetabular aseptic loosening. The average graft coverage percentage of the acetabular component was 34%.
Of the four patients who required revision surgery due to aseptic loosening, only one had graft coverage of >40% (47%). In 19 of the 74 hips, there was 40% graft coverage. The rate of graft coverage was >50% (56%) only in one patient, and the follow-up of this patient revealed graft union with no radiolucent area or aseptic loosening of the acetabular component. In our series, there was no significant difference in graft coverage in patients with and those without aseptic loosening. However, we did not have a sufficient number of patients with a graft coverage percentage >50% to accurately assess the relationship between graft coverage and aseptic loosening. Use of highly porous trabecular metal cups may be used in the reconstruction of mild to moderate acetabular bone defects, with a portion of the cup uncovered by native bone. These materials can promote osseointegration even with reduced host bone contact less than 60%. However, the size (mean acetabular cup diameter: 49 mm) of the socket is a limitation in this study. Also, we are not able to use trabecular metal augments in our country due to restrictions.
In the literature, Abdel et al. 9 who performed arthroplasty using a femoral head graft reported a mean acetabular component diameter of 48 ± 5.2 mm (range 42–58 mm), and Maruyama et al., 21 in their 102-case study, observed that the acetabular component diameter was 40–50 mm; more than half of the patients had an acetabular component of 48 mm. In the present study, the mean acetabular cup diameter was 49 mm (range 40–60 mm), which is consistent with the literature. Due to the bigger contact surface with host and graft, the largest possible acetabular cup could be used. The mean graft thickness was 29 ± 4.6 mm (range 10–52 mm), and the mean graft–acetabulum contact length was 34 ± 6.1 mm (range 13–67 mm). Concerning these evaluations, the literature contained only one other study that of Schofer et al. 11 who reported that the mean contact length was 36 mm (range 12–110 mm) and that the graft thickness was 25 mm in most patients (range 10–50 mm). Measurement of these values may contribute to an investigation into the autograft union and stability; however, in our study, lateral graft overflow was clinically significant because, in two of our patients, the autograft impinged the greater trochanter of the femur, causing early recurrence of the hip dislocation. In both patients, the autograft was removed, reshaped, and fixed to the acetabulum. Redislocation was not seen in either of these patients after the revision surgery.
Anderson and Harris used cementless acetabular components and observed no loosening, migration, or pelvic osteolysis over the 8-year follow-up of 24 hips. Also, the authors emphasized that covering 80% of the cementless component with healthy bone tissue was sufficient to ensure stability. 12 In cementless porous-coated acetabular components, biological fixation occurs with the introduction of living bone tissue between porous surfaces, which decreases the stress on the graft and the possibility of mechanical failure of the graft. 27 –29 If a cemented acetabular component is to be used, the cement should not contact the junction between the autograft and recipient bone to prevent any effect on graft union. 30 In the present study, cementless acetabular components were used in most patients (n = 71), whereas cemented acetabular components were utilized only in three. We had a limited number of patients to evaluate the relationship between aseptic loosening and the use of cemented acetabular components. However, as mentioned in the literature, we consider that the use of a cemented component causes early aseptic loosening and, therefore, prefers to use cementless components in our daily practice. Similarly, bilateral cemented components were used in one of the earlier cases in our series. Complication developed in another case in which a cementless acetabular component was used. Thus, we continued to use cementless components in the remaining patients. Our results are consistent with those in the literature (Table 1).
Intraoperative femoral fracture rates in uncemented femoral stems have been reported between 1.5% and 27.8%. 31,32 Higher intraoperative femoral fracture rate has been associated with femoral stem design and intraoperative technique. Also, several risk factors, such as older age, the operative volume of the surgeon, female gender, revision surgery, minimally invasive approach, metabolic bone disease, technical errors, and using the press-fit cementless stem, were reported in the development of intraoperative femoral fracture. 33 In our study, the intraoperative femoral fracture rate was found at 20%. It is higher than previous studies performed with cementless stems (Table 1). When our fractures were further evaluated, all patients were female. Their age was significantly higher than in nonfractured patients. Tapered wedge femoral stem was used in most of or patients. Also, stem sizes were higher than nonfractured femurs. The above factors may explain our higher intraoperative fracture rate. Dislocation rates of the hip after reconstruction of the acetabulum with femoral head autografts have been reported between 0% and 10%. 3,11,13 Gerber and Harris reported a 10.6% incidence of dislocation in 47 hips. 3 Schofer et al. reported dislocation of the hip after reconstruction of the acetabulum with femoral head autografts that occurred in 3 of 118 hips (2.5%). 11 Spangehl et al. reported no dislocation after reconstruction of the acetabulum with femoral head autografts. 13 In this study, dislocation was occurred in nine patients (12%). It was slightly higher than previous reports. Technical errors observed in the dislocated hips may be related to the first 25 cases of the series. Also, the management of dysplastic hips requires a steep learning curve and needs to be addressed by specialized units only to decrease the revision and dislocation rates.
Limitations of our study include its retrospective nature, the absence of a comparison group, a relatively short follow-up duration, operations performed by more than one surgeon, graft union evaluated using only direct radiography, different degrees of hip dysplasia, and variation of the acetabular components used. Also, the use of nonmodular monoblock stems could be the cause for both intraoperative fractures and postoperative dislocation. In patients in whom combined anteversion is low, a modular stem like an SROM stem or a Wagner cone stem or a cemented stem could have been used to reduce the intraoperative fracture and dislocation rates.
Conclusion
In patients with osteoarthritis secondary to developmental hip dysplasia, the use of femoral head autografts to eliminate acetabular coverage deficiency during THA achieves acceptable midterm postoperative radiological outcomes. However, to fully evaluate the efficacy of this method, long-term outcomes of a larger number of cases should be investigated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.