
Abstract
Purpose:
This study aimed to evaluate the feasibility and effect of triamcinolone acetonide (TA) injection for lateral malleolar (LM) bursitis.
Methods:
We retrospectively reviewed data of 49 consecutive patients (49 ankles) who received TA injection between March 2016 and March 2019. All cases received 1 ml (40 mg) of TA injection after aspiration of fluid in the LM bursal sac. Subsequently, the ankle was compressed with an elastic cohesive bandage for 2 weeks. Treatment responses were assessed according to the degree of fluctuation, shrinkage of the bursal sac, and soft tissue swelling. We used the Medical Outcomes Study Short Form Health Survey (SF-36) and complications at 2 and 4 weeks and at 3 and 6 months after TA injection.
Results:
Forty-four patients (89.8%) experienced complete resolution, four (8.2%) had partial resolution, and one (2.0%) had no resolution after the first or second TA injection. The physical component scores of SF-36 improved from 72.8 ± 6.0 to 82.3 ± 6.5 at the last follow-up (p < 0.001). Associated complications included skin atrophy in three patients (6.1%) and transient hyperglycemia in four (8.2%).
Conclusion:
TA injection is an effective and safe procedure for LM bursitis. It should be considered as a primary treatment method.
Introduction
Bursa is a closed sac that is lined by synovial membrane, contains synovial fluid, and is located between surfaces where there is friction and movement. 1 The function of a bursa is to reduce friction by creating a space between two tightly apposed surfaces. 2 The malleoli do not usually have bursae, but lateral malleolar (LM) bursitis develops as a result of repeated irritation, trauma, excessive compression, or shear forces between lateral malleolus and shoes. 3 LM bursa is an adventitious bursa, 4 which is common in athletes who wear hard shoes that cover their ankles, such as skaters, or in Asians who usually sit on the floor with their legs crossed. 3,5,6 In the past, it occurred in coal miners who commonly sat in a cross-legged manner in the restricted height environment of coal seams and was called coal miner’s ankle. 7 Histological changes in the adventitious bursa are characterized by mucoid and myxomatous degeneration of connective tissue. 4,8 Different stages of development have been described, including early bursa formation characterized by an increased number of blood vessels and inflammatory cells without cavities and late stages characterized by small cavities that progress to large cystic cavities. 4,8 The main symptoms include irritation, discomfort, cosmetic problems, and pain. 9
First-line treatment of LM bursitis includes conservative treatment such as lifestyle changes with avoidance of the sitting position, aspiration, or a compression bandage is preferred, but the patient’s satisfaction is not high because of the high recurrence rate. 3,5 In addition, if bursitis does not improve after first-line treatment, it can then become enlarged or inflamed, negatively affecting the patient’s ability to wear shoes and hindering the patient’s lifestyle and performance in sports. 6,9 Operative excision of LM bursa could be considered if conservative treatment failed, recurrent bursitis, or infected bursitis. 3,5 However, operative management can cause painful scarring, superficial peroneal nerve injury, cosmetic problem, and recurrence. 3,9
LM bursitis is an appropriate target for periarticular corticosteroid injection. 10 Although periarticular corticosteroid injection for LM bursitis has been referred to as a first-line treatment method in several studies, 5,6,9 only few studies have reported outcomes of corticosteroid injection and there is no consensus on the preferred choice and optimal dose of corticosteroid. Triamcinolone acetonide (TA) is a long-acting corticosteroid and is most commonly used for intralesional and small intraarticular injections. 11,12 This study aimed to evaluate the feasibility and effect of TA injection for LM bursitis.
Methods
Between March 2016 and March 2019, 87 consecutive patients were diagnosed with LM bursitis of the ankle based on clinical symptoms, physical examination, and radiological evaluation. We evaluated all patients by simple anteroposterior and lateral radiographs of both ankle and performed ultrasonography over the lateral malleolus. The following diagnostic criteria of LM bursitis were applied: soft tissue swelling and fluctuation over the lateral malleolus; no infection signs such as heating sensation, tenderness, and open wounds; no fracture or foreign body visible in the simple radiographs; and visible bursal sac with fluid collection in the ultrasonography. Of these, 10 patients with previous corticosteroid injection within the preceding 3 months and 28 patients with infected bursitis requiring operative treatment were excluded. A total of 49 patients (49 ankles) received 1 ml (40 mg) of TA (Kenalog; Bristol-Meyers Squibb, Princeton, New Jersey, USA) injection. Patients’ medical records were used to obtain data on their age, gender, the side of the affected lateral malleolus, disease duration, number of TA injections, follow-up period, clinical outcomes, subjective satisfaction, recurrence, and complications. Except for 16 patients (32.7%) experiencing their first episode of LM bursitis, an average of 2 aspirations (range, 0–10) had been performed in 67.3% (33 of 49 patients), of which 18.2% (6 of 33 patients) experienced recurrence afterward. This retrospective study was approved by the institutional review board of our hospital.
There were 32 men and 17 women, with a mean age of 61.6 (range 41.0–81.0) years. There were 24 patients with right ankle and 25 with left ankle bursitis. The mean duration of the disease was 10 (range 0.5–32) weeks (Table 1). In the outpatient clinic, each patient was placed in the semi-lateral position with the affected side up. TA solution was prepared in a 5-ml syringe, with 40 mg of TA in 1 ml composition. The bursal sac was punctured posteroanteriorly using an 18-gauge needle with a 10-ml syringe, and the bursal sac fluid was aspirated as much as possible: approximately 5.2 (range 4.0–9.8) ml (Figure 1(b)). Then, 1 ml (40 mg) of TA was injected into the bursal sac using a different syringe with the same needle used for aspiration (Figure 1(c)). After TA injection, we applied a compressive dressing using cohesive elastic bandage for at least 2 weeks (Figure 1(d)). TA injections were not performed more than two times.
Demographic characteristics and clinical outcome of the patients.

OA: osteoarthritis; DM: diabetes mellitus; CKD: chronic kidney disease; LC: liver cirrhosis; CR: complete response; PR: partial response; NR: no response; SF-36: Medical Outcomes Study Short Form Health Survey; PCS: Physical Component Score; MCS: Mental Component Score; SD: standard deviation; M: male; F: female; R: right; L: left; Rt. ankle: right angle; Lt. ankle: left ankle; HT: hypertension; CHF: congestive heart failure.

(a) Initial photography of the swollen left ankle LM bursitis. (b) The bursal sac was punctured posteroanteriorly using an 18-gauge needle with a 10-ml syringe. (c) One milliliter (40 mg) of TA was injected into the bursal sac using a different syringe with the same needle used for aspiration. (d) After injection, we applied a compressive dressing using cohesive elastic bandage for at least 2 weeks. LM: lateral malleolar.
The average follow-up period was 6.8 (range 6–10) months. Patients were examined at 2 and 4 weeks and at 3 and 6 months after TA injection. The resolution of LM bursitis was assessed using response evaluation criteria, 9 which were modified from the guidelines of the response to treatment in a solid tumor. 13 Clinical evaluation was performed by one of the authors who did not perform the injection. The response evaluation criteria include the degree of fluctuation, shrinkage of the bursal sac, and soft tissue swelling (Table 2). 9 To measure subjective satisfaction of patients, a physical and mental status questionnaire was conducted at first visit and at the final follow-up. We used the Medical Outcomes Study Short Form Health Survey (SF-36), 14 which is a health status questionnaire for the assessment of the functional status and quality of life. In addition, we observed for skin atrophy, transient hyperglycemia, skin depigmentation, infection, facial flushing, and scarring during the follow-up period. 12
Response evaluation criteria for malleolar bursitis of the ankle.

Data were analyzed using SPSS software, version 20.0 (SPSS Inc., Chicago, Illinois, USA). Categorical variables are presented as numbers and percentages and continuous variables as mean and standard deviations for normally distributed data or as median and interquartile range for non-normally distributed data. Wilcoxon signed rank test was used to analyze pre- and postinjection SF-36 outcomes. Statistical significance was defined at the 5% (p < 0.05) level.
Results
Complete resolution was observed in 44 patients (89.8%); 42 patients (85.7%) responded at 2 weeks after the first TA injection, and 2 patients (4.1%) responded at 2 weeks after the second TA injection (Table 3). Six patients (12.2%) received second TA injections after 4 weeks due to insufficient shrinkage. Insufficient shrinkage was diagnosed in the presence of soft tissue swelling and fluctuation 4 weeks after first injection according to the response evaluation criteria. 9 A second injection was performed if soft tissue swelling and fluctuation remained. Partial resolution was observed in four patients (8.2%) after the second TA injection; however, all four patients were satisfied with the partial response and did not want to undergo operative excision. One patient experienced recurrence of LM bursitis 3 months after TA injection but showed complete resolution after an additional TA injection. There was one unresponsive patient (2.0%) despite a second TA injection; patient symptoms were resolved with operative excision without complications. The physical component scores of SF-36 improved from 72.8 ± 6.0 to 82.3 ± 6.5 (p < 0.001). The mental component scores of SF-36 did not change significantly (p = 0.363) (Table 4). The increase in the scores of SF-36 indicates that patients were satisfied with the outcomes, although the bursal sacs were not large enough to affect function. 9 Twenty-four patients (48.9%) had comorbidities, such as angina pectoris (three patients), ankle osteoarthritis (nine patients), breast cancer (one patient), cerebrovascular disease (one patient), chronic pancreatitis (two patients), chronic kidney disease (four patients), diabetes mellitus (nine patients), hypertension (four patients), and liver cirrhosis (two patients) (Table 1). However, the clinical outcomes may not be related to comorbidities.
Clinical outcomes of triamcinolone acetonide injection for LM bursitis.
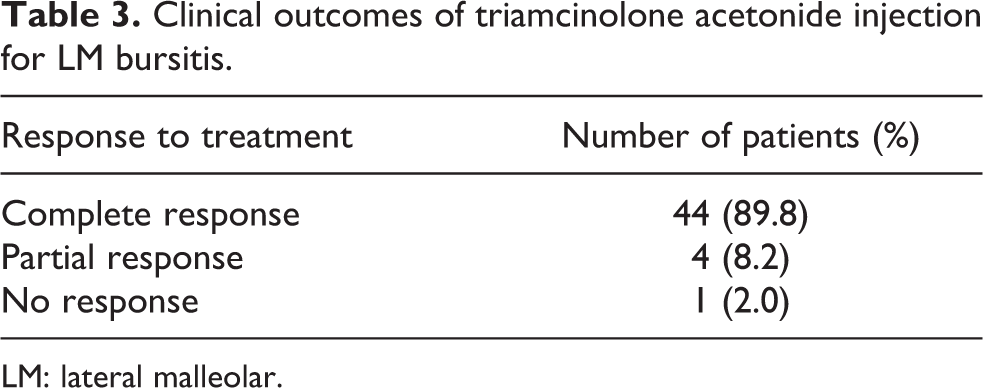
LM: lateral malleolar.
SF-36 scores before and after triamcinolone acetonide injection for LM bursitis.a

SF-36: Medical Outcomes Study Short Form Health Survey; PCS: Physical Component Score; MCS: Mental Component Score; LM: lateral malleolar.
a Values are represented as mean ± standard deviation.
Skin atrophy was observed in three patients (6.1%). Within 3 months, skin atrophy was resolved and became comparable to the contralateral side in all patients. Four patients (8.2%) with transient hyperglycemia attained normal blood glucose levels within 1 week of TA injection. No other complications occurred after TA injection, such as postinjection pain, skin depigmentation, infection, facial flushing, or scarring (Table 5).
Side effects of triamcinolone acetonide injection for LM bursitis.
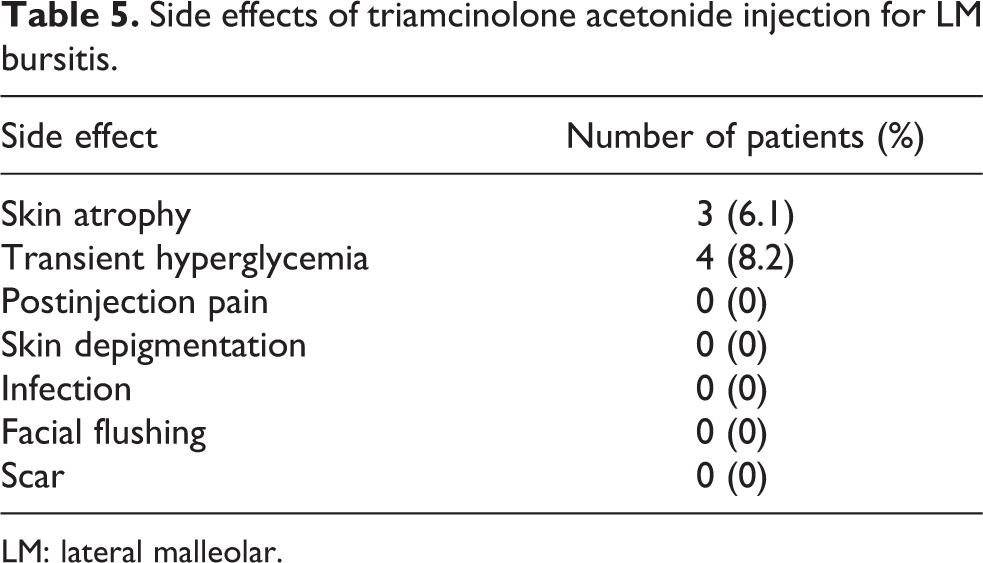
LM: lateral malleolar.
Discussion
Bursitis is a common disease entity which could occur in any area of the body. The bursal lining is a poorly vascularized synovial membrane that has a low coefficient of friction; 15 it reduces friction, allowing the skin move smoothly over the bone during joint motion. 6,15 Bursae can be classified into anatomical and adventitious bursae. 5 An anatomical bursa is usually not present at birth; rather, it develops in response to normal friction between tendons and adjacent structures. An adventitious bursa is usually subcutaneous and develops after birth as a protective response to repeated trauma or constant friction. 6
LM bursa is an adventitious bursa which develops as a result of chronic pressure on the LM area. This chronic pressure is usually generated by the cross-legged sitting position common in specific regions or by general weakness-induced external rotation of the hip. 16 Repeated microtrauma or inflammation induces the proliferation of synovial cells, and subsequently, the bursal sac fills with fibrous exudates. 17 Because the symptoms are not severe unless an infection is present, conservative treatment, such as lifestyle modification, aspiration, compression, and corticosteroid injection, is the first-line treatment. However, conservative treatment showed a high recurrence rate of 43.7% (7 of 16 patients) with lifestyle modification 5 and of 35% (21 of 60 patients) with simple aspiration and compression. 3
TA injection has many advantages over other conservative and operative treatments. First, TA injection is a simple and fast procedure. Patients only need to undergo aspiration, injection, and 2 weeks of compression. Second, TA injection does not need hospitalization, or analgesics for injection site pain. Third, TA injection is not expensive and has fewer complications with lower recurrence rate. Additionally, TA injection does not need multiple injections. Given these advantages, TA injection seems to be suitable for the first-line treatment of primary LM bursitis.
In our study, 33 of 49 patients (67.3%) had recurrent LM bursitis with history of an average of two aspirations (range 1–10) in other hospitals (Table 1). Although patients with recurrent LM bursitis are often referred for operative excision, the procedure has many complications such as hyperesthesia, wound healing, and recurrence. 3,5,18 Therefore, OK-432 sclerotherapy 9 and 50% ethyl alcohol injection 19 have been introduced for recurrent LM bursitis. Park et al. 9 reported excellent results: 95% (19 of 20 patients) experienced complete resolution with OK-432 sclerotherapy. However, due to the nature of OK-432, which induces strong local inflammation by production of cytokines, 20 complications such as low-grade fever (30%), local redness and swelling (45%), and pain (45%) occurred. Hong et al. 19 reported the outcome of 50% ethyl alcohol injection for chronic intractable malleolar bursitis. Although 54% (13 of 24 patients) had complete resolution and 46% (11 of 24 patients) achieved partial resolution, the mean number of alcohol injection was 3.8 with a maximum of 17 injections. Additionally, 16.6% (4 of 24 patients) showed injection site warmth and pain for an average of 2.1 months. In our study, 44 of 49 patients (89.8%) showed complete resolution at 6 months after TA injection with minimal complications. Of these, 29 of 33 patients (87.9%) with recurrent LM bursitis showed complete resolution. These results were superior when compared with usual conservative treatment.
Judicious corticosteroid injection to periarticular structures may provide substantial pain relief and enhance the performance of activities of daily living. 10 For several reasons, LM bursitis is an appropriate target for periarticular corticosteroid injection. First, the bursal sac is mainly formed by the connective tissue. 1 TA inhibits growth, regeneration, and repair of cellular and intercellular components of the connective tissue. 21 It affects fibroblast proliferation and production capabilities and is responsible for their degeneration. Second, in histological sections of well-formed LM bursa, new blood vessels and inflammatory cells were evident in the connective tissue of the wall of the bursal sac. 1 TA suppresses inflammation by inhibiting leukocyte and monocyte migration and phagocytosis, 22 which subsequently relieves inflammatory symptoms of bursitis. Third, TA is a powerful vasoconstrictor, reducing the delivery of oxygen and nutrients to bursal sac. 22
Corticosteroid injections have many well-known complications. However, they are safe and comfortable when proper technique is used. 23 Systemic complications of injectable corticosteroids are rare. 24 Notably, the risk of septic arthritis is less than 0.03%. 25 The risk of hyperglycemia is very low and transient. 26 Other complications include skin atrophy, skin depigmentation, and facial flushing. 24 Skin atrophy is one of the most common side effects of corticosteroid injections and is more common with long-acting corticosteroid such as TA. 10 It is generally transient and may occur in areas with little subcutaneous fat such as the lateral aspect of the ankle. 27 The incidence of skin atrophy after periarticular corticosteroid injection has been reported from 1.0% to 2.4%. 10,28 In our study, skin atrophy was observed in three patients (6.1%), two of whom received second TA injections. The frequency of skin atrophy may depend on the method of administration, the administered compound, and dose. Although all the three patients recovered within 3 months, care must be taken before injection, especially before the second injection. The risk of skin atrophy is greater when inadvertent injection of the surrounding normal tissue occurs. Therefore, it is important to position the needle exactly inside the bursal sac. Changing the needle after loading the syringe to avoid corticosteroid coating of the outer needle surface, flushing the needle with anesthetic or saline after its injection, and diluting the corticosteroid with several volumes of other fluid may reduce skin atrophy. 10 Highly balanced esters of triamcinolone or methylprednisolone are the preferred agents for periarticular injections administered by physicians. 10 These branched esters of hydrocortisone were superior to hydrocortisone itself due to insolubility. 29 TA and methylprednisolone acetate (MA) have the same efficacy at the same dose. 30 However, the average duration of action for TA (14 days) is longer than that of MA (8 days) at the same dose. 10 Avci and Sayli 5 reported a high recurrence rate of 75% (3 of 4 patients) with 20 mg MA injection for premalleolar bursitis. Although there is no consensus on the appropriate dose of periarticular corticosteroid injection, 20 mg of MA has half the efficacy and a shorter duration (<8 days) compared to 40 mg of TA used in our study. Inadequate dose of MA and lack of compression after injection may result in a high recurrence rate.
The choice of different corticosteroids in a given practice is largely based on consideration that includes availability, cost, and versatility of the agent. 24 In many cases, it depends on where the physician was trained. 31 There is also a lack of consensus on frequency and dose for periarticular corticosteroid injection. 32 It could be partially explained by the rarity of studies comparing the efficacy of different corticosteroids. Although there are no clear evidence-based recommendations as to the appropriate number of injections, we did not perform more than two injections to prevent complications related to overdose. MA, triamcinolone hexatonide (TH), and TA in that order to be the most popular agents for intraarticular injection. 31 Several studies suggest that TH has greater efficacy than TA and MA in chronic inflammatory arthritis. 33 Because TA is the most frequently injected corticosteroid at our facility and TH is not imported into our country, we used TA for LM bursitis in our study. Randomized controlled trial for efficacy and dose-related complications depending on the type of long-acting corticosteroids are necessary to consider in a future study.
Our study had several limitations. First, this study has all the shortcomings of a retrospective study. Second, there was no control group for comparison with the TA injection group. Third, we included a relatively small number of patients and short follow-up periods. A prospective, randomized controlled trial with a larger number of patients will be needed in the future. Fourth, the clinical outcomes were not evaluated using functional scoring system. Since LM bursitis, which is not accompanied by an infection, is usually painless and has no significant effect on the patient’s function, it was difficult to use functional scoring system based on pain relief and function recovery. Therefore, the authors have tried to evaluate subject satisfaction of the patient using SF-36 scores instead of using functional scoring system.
In conclusion, TA injection is an effective and safe procedure for first-line treatment of patients with LM bursitis. According to our results, TA injection elicited complete or partial resolution in nearly all patients with LM bursitis, without severe complications. Before undergoing TA injection, patients should be warned of the possible complications, such as skin atrophy and transient hyperglycemia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research, authorship, and/or publication of this article: This study was supported by grants from Basic Science Research Program (NRF2018R1D1A1B07047666) through the National Research Foundation of Korea (NRF) grant funded by the Korean government.