
Abstract
Background:
Several factors affect proximal humeral fracture (PHF) morphology. In the presence of glenohumeral osteoarthritis (GOA), the joint kinematics is alternated which might influence fracture configuration. The purpose of this study was to identify fracture patterns in patients with advanced osteoarthritis to facilitate recognition and treatment.
Methods:
In this retrospective analysis, and computed tomography (CT) scans of all patients undergoing surgical treatment for a PHF during a 5-year period were analyzed. Fracture pattern according to the AO Foundation/Orthopaedic Trauma Association (AO-OTA) classification and the presence of GOA were evaluated. In addition, critical shoulder angle (CSA), glenoid configuration, and glenoid inclination (GI) were measured.
Results:
Of the 713 patients, 574 met the inclusion criteria. A total of 166 patients showed radiological signs of GOA (28.9%). Advanced GOA (stage 2 or 3) was identified in 23 patients (4.0%). In this group, the mean age was 77 ± 10 years, mean CSA was 28.8 ± 4.2°, and the mean GI was 19.0 ± 7.8°. All fractures were extra-articular metaphyseal fractures (5 A2, 11 A3, 7 B1.1). Patients with advanced GOA had more than threefold risk (risk ratio 3.2; confidence interval 95% 2.80–3.74; p < 0.0001) for sustaining a metaphyseal fracture. In patients with GOA grade 1 compared to patients with no radiographic signs of GOA, this could not be observed.
Conclusion:
Patients experiencing PHF with radiological signs of advanced GOA have a higher risk of sustaining a metaphyseal fracture compared to individuals with the absence of or mild GOA. To date, no classification system for PHFs takes preexisting osteoarthritis into account, although it might indicate a different treatment and therefore the recognition is crucial.
Introduction
With an aging population, the incidence of degenerative shoulder pathologies such as cuff tear arthropathy (CTA) and glenohumeral osteoarthritis (GOA) is continuously increasing. Numerous studies have demonstrated the prevalence of rotator cuff tears to be as high as 30%, 1,2 whereas the prevalence of GOA has been estimated to be as high as 26%. 3 Overall, proximal humeral fractures (PHFs) account for 5% of all fractures and are more common in the elderly population. 4 In a normal fall, the arm is typically held in flexion, abduction, and internal rotation as a reflex to absorb the impact. 5 In this position, the humeral head is pressed against the glenoid, which normally presents a stronger bony structure, and thus the proximal humerus finally breaks. 6,7 To understand the fracture morphology, several factors have to be taken into account. Due to the characteristic arm position at the time of the accident and the anatomical retroversion of the humeral head, it is pressed dorsally and caudally of the glenoid. In addition, there are several inserting tendons causing further dislocation forces. 5 With reduced bone substance the bone may already break under less force and a subcapital PHF is more likely to occur. 5 The combination of different acting forces at the time of the accident, inhomogeneous bone quality, and the vectors of the attaching muscles results in a high fracture variability. In the presence of GOA, the glenohumeral contact pressure is alternated 8 which might also affect the fracture pattern. To date, a different fracture morphology in the case of GOA has not been described yet, although it might influence the treatment method and postoperative outcome. Therefore, the purpose of this study was to analyze the PHF morphology in patients with advanced osteoarthritis to facilitate recognition and treatment.
Materials and methods
Following institutional board approval, all consecutive patients with a PHF treated surgically in our institution during the 5-year period from 2014 to 2019 were included in this study and were retrospectively analyzed. Inclusion criteria were the presence of an acute proximal humeral fracture (<6 weeks), the availability of preoperative radiographs, and a preoperative computed tomography (CT) scan. Exclusion criteria were bone and joint infection as well as pathological fractures. Data collected were patient demographics, fracture classification according to the revised AO Foundation/Orthopaedic Trauma Association (AO-OTA) classification, 9,10 and severity of GOA if present. Classification of the GOA was realized according to Samilson and Prieto. 11 Osteophytes, subchondral bone sclerosis, pseudocystic areas, and altered shape of bone ends were assessed. Narrowing of the joint space was not considered as a factor because an intra-articular hematoma might lead to joint distension resulting in a widened joint space. Therefore, within our eyesight range, the interpretation of joint space narrowing in a fracture situation is unreliable. Preoperative radiographs and computed tomography (CT) scans were used for radiographic analysis. The measurements on preoperative conventional radiographs included critical shoulder angle (CSA) 12,13 and glenoid inclination (GI) 14 as shown in Figure 1(a) and (b). Bone quality was quantified with the deltoid tuberosity index (DTI) (Figure 1(c)). 15

Preoperative measurements on plain radiographs: (a) CSA, (b) GI angle according to Habermeyer, and (c) DTI. CSA: critical shoulder angle; GI: glenoid inclination; DTI: deltoid tuberosity index.
With the CT scans, fracture classification and evaluation of the glenoid morphology according to Walch 16 was performed. Measurements and classifications were performed by two examiners (JS and MJ).
Statistical analysis
Statistical analysis was performed with IBM SPSS for Windows version 22 (SPSS inc., Chicago, Illinois, USA). Results were considered statistically significant for the values of p < 0.05. Categorical variables were reported as frequencies with the corresponding percentages, whereas continuous variables were reported as mean value and standard deviation (SD).
Results
A total of 713 proximal humeral fractures were treated in our institution during the 5-year period (713 patients; 463 females; 424 fractures involved the right side). Of these, 574 fulfilled the inclusion criteria. The mean age was 69 years (range 23–97 years, SD 14.5 years). The overall distribution of the different fracture types according to the AO-OTA classification is shown in Figure 2.

The overall distribution of the different fracture types according to the AO-OTA classification. AO-OTA: AO Foundation/Orthopaedic Trauma Association.
In total, 166 patients showed radiological signs of GOA (28.9%). Advanced GOA (stage 2 or 3 according to Samilson and Prieto 11 ) was identified in 23 patients (4.0%; 13 grade 2, 10 grade 3). Baseline characteristics, fracture and glenoid classification, and the evaluated radiological parameters of the patients with advanced GOA (grade 2 and grade 3) are listed in Table 1.
Baseline characteristics, fracture and glenoid classification, and the evaluated radiological parameters of the patients with severe glenohumeral osteoarthritis (grade 2 and grade 3).

SD: standard deviation; GOA: glenohumeral osteoarthritis; AO-OTA: AO Foundation/Orthopaedic Trauma Association; CSA: critical shoulder angle; GI: glenoid inclination; DTI: deltoid tuberosity index.
In this group, the mean CSA was 28.8 ± 4.2° and the mean GI was 19.0 ± 7.8°. According to Habermeyer, there were nine cases of vertical glenoid morphology type 1, eight cases of type 2, and six cases of type 3. The mean DTI was 1.39 ± 0.31. All fractures were extra-articular metaphyseal fractures (5 A2, 11 A3, 7 B1.1). Regarding the glenoid morphology, there were 10 A2, 6 B1, and 7 B2 glenoids.
In the presence of GOA, the risk of sustaining a metaphyseal humeral fracture increased with the grade of GOA in comparison to its absence. In patients with GOA grade 2 and grade 3, the risk of sustaining a metaphyseal fracture was more than threefold (risk ratio 3.2; confidence interval (CI) 95% 2.80–3.74; p < 0.0001) compared to patients without radiological signs of GOA. On the contrary, there was no significant difference in the fracture morphology observed in patients with GOA grade 1 (risk ratio: 1.2; CI 95% 0.89–1.51; p = 0.28) in comparison to patients without GOA. The percentage of metaphyseal fractures increases with the presence and severity of GOA as it is demonstrated in Figure 3. In Figure 4, exemplary preoperative radiographs with the typical metaphyseal fracture morphology are shown.
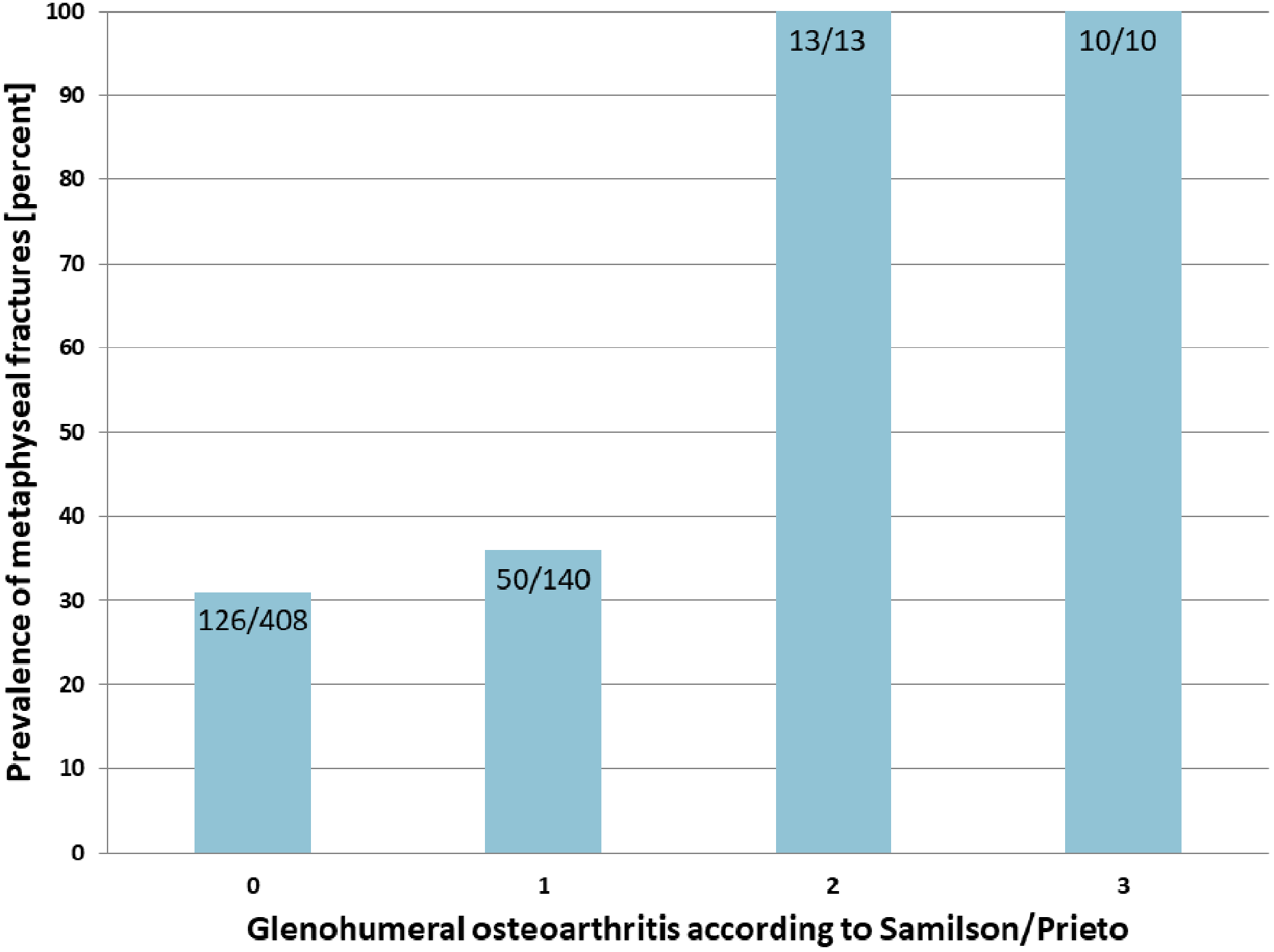
Percentage of metaphyseal fractures in patients without and with different grades of glenohumeral osteoarthritis.

Exemplary images of four cases. (a) 3D CT of a 64-year old female with GOA grade 2 and an AO 11A3 fracture. (b) AP radiograph of a 69-year old female with GOA grade 2 and an AO 11-A3 fracture. (c) AP radiograph of a 79-year old female with GOA grade 3 and an AO 11-A2 fracture. (d) AP radiograph of an 88-year-old female with GOA grade 3 and an AO 11-A3 fracture with a metaphyseal comminution zone and a DTI of 1.22. 3D: three dimensional; AP: anteroposterior; CT: computed tomography; DTI: deltoid tuberosity index; GOA: glenohumeral osteoarthritis.
Discussion
The presence of GOA in patients with a PHF might affect the choice of the treatment method and the outcome. To date, little attention has been paid to the influence of GOA on the fracture pattern in PHF and possible consequences for the treatment. Therefore, this study focused on identifying and reporting the association between the presence of GOA and the PHF morphology.
Compared to other studies, the demographics of the study population were comparable regarding age and gender with a mean age of nearly 70 years and a female-to-male ratio of around 2:1. 17 –19
For fracture classification, we applied the AO-OTA classification as it has been described to be more comprehensive for an exact description of the fracture pattern than the commonly used Neer 7 classification. 18 As we only analyzed those patients treated with surgery, the epidemiology of the fracture morphology differed from the literature with a far higher percentage of AO type C lesions of 55% in our cohort. According to an epidemiological study of 1027 PHF in an overall population of 700,000 individuals realized in the United Kingdom, most PHF were AO type A lesions (66%), followed by type B lesions (27%) and only 6% were AO type C fractures. 18
Considering the presence of GOA in patients with PHF, to date no data are available in the literature. In our cohort, 29% of the patients showed radiological signs of osteoarthritis, whereas an advanced stage with osteophytes greater than 3 mm could be observed in 4% of the study population. Interestingly, those numbers are consistent with those reported for the overall population. 3
Regarding the potential association of the grade of GOA with the fracture pattern, we could show a statistically significant increased risk with a more than threefold risk ratio for extra-articular, metaphyseal fractures in patients with GOA grade 2 or 3 according to Samilson/Prieto. 11 For the shoulder, this has not been described before. However, similar findings have been reported for patients with advanced osteoarthritis of the hip (grade 2 and 3 according to Kellgren/Lawrence 20 ) who sustained a proximal femoral fracture. According to Aguado-Maestro et al. 21 and Calderazzi et al., 22 in these patients, the ratio of extracapsular trochanteric fractures to intracapsular femoral neck fractures is augmented.
As expected, the 23 patients with advanced GOA of our cohort showed typical radiological features such as a small CSA, 12 a pathological glenoid inclination 14 and concentric or eccentric glenoid wear 16 as described before for patients with GOA. The bone quality measured with the DTI did not influence the metaphyseal fracture location, however, all patients with a DTI < 1.4 presented a metaphyseal comminution zone (Figure 4(d)). This could not be observed in patients with DTI > 1.4 (Figure 4(b)).
Currently, there is no literature available that provides an explanation for our findings regarding the altered fracture morphology in the case of advanced GOA. However, the osteoarthritic glenohumeral joint undergoes several anatomical adaptations such as posterior glenoid wear, 23,24 flattening of the humeral head as well as the glenoid surface, 23 and modification of the retroversion 25 resulting in an altered geometry affecting joint kinematics. In a finite element model of the shoulder comparing normal and osteoarthritic joints, Büchler et al. 8 found that alteration of the humeral head geometry may greatly increase the contact pressure and influence stress distribution in the glenohumeral joint. In addition, Matsen reported higher necessary muscle forces during the motion of the osteoarthritic shoulder. 24 Taking into account these presumptions, we hypothesize that an increased contact pressure in combination with less mobility could result in a different fracture pattern in the case of a PHF as shown in Figure 4. In our cohort, 100% of the patients with advanced GOA presented extra-articular metaphyseal fractures confirming our theory.
In the case of preexisting GOA, the shoulder function is compromised, 23,24 thus conservative or osteosynthetic treatment of a PHF might result in an impaired functional outcome; however, no data have been published yet in this regard. To date, no classification system for PHF takes a preexisting GOA into account, although the recognition of such pathology most likely influences the treatment. In this cohort, all 23 patients were treated either with hemiarthroplasty (2 patients younger than 60 years of age) or with primary reverse shoulder arthroplasty (21 patients). Exemplary images pre- and postoperative images are shown in Figure 5.

Pre- and postoperative images of two exemplary cases: (a to c) a 68-year-old man with GOA grade 3 and an AO 11-A3 fracture treated with primary reverse shoulder arthroplasty. (d to f) a 76-year-old man with GOA grade 2 and an AO 11-A2 fracture treated with primary reverse shoulder arthroplasty with an additional wire cerclage to allow refixation of the metaphyseal fragment with the tuberosities.
Limitations
This is a radiological retrospective case series analyzing the fracture morphology in patients with advanced GOA. The described pathognomonic fracture morphology is only an observation. To date, there is no scientific proof for this phenomenon. Further biomechanical studies are necessary to prove this hypothesis. In addition, the study cohort might not accurately represent the incidence of the underlying glenohumeral OA as the decision for surgery might have created a bias, in which more severe fracture patterns (AO-OTA type C) in already arthritic and poorly performing shoulders in multimorbid patients might have been elected for nonoperative treatment.
Conclusion
With increased degenerative changes of the glenohumeral joint, the fracture pattern shifts to metaphyseal comminution, as patients with advanced glenohumeral osteoarthritis with an acute proximal humeral fracture have a threefold risk of sustaining a metaphyseal fracture when compared to patients without osteoarthritis. To date, no classification system for proximal humeral fractures takes preexisting osteoarthritis into account, although it might indicate a different treatment and therefore the recognition is crucial.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.