
Abstract
Purpose:
Successful arthroscopic femoroplasty in patients with cam lesions have been reported in Western countries in the last two decades. However, the outcomes after arthroscopic femoroplasty in Asia have thus far only been reported in patients with borderline dysplasia and in the military population. This retrospective study was designed to evaluate the short-term clinical outcomes and radiologic outcomes after hip arthroscopy in patients with cam-type femoroacetabular impingement (FAI) at a minimum postoperative follow-up of 2 years.
Methods:
From January 2013 to December 2016, 204 hip arthroscopy procedures were performed. Of these cases, 62 patients (73 hips) underwent hip arthroscopy for cam-type FAI.
Results:
Of the 73 hips, 65 (89.0%) achieved gratified reduction or elimination of preoperative pain. The clinical outcomes showed improvement in scores from before surgery to the last follow-up: 67.1 ± 15.0 to 90.2 ± 6.3 for the modified Harris hip score (p < 0.001), 4.7 ± 2.5 to 7.1 ± 1.4 for the University of California Los Angeles score (p < 0.001), and 7.4 ± 1.9 to 1.8 ± 1.5 for the visual analog scale score (p < 0.001). In radiologic assessments, significant improvement was observed in the alpha angle from a mean 60.9° to 49.5° (p < 0.001) and in the head–neck offset from a mean of 3.3 mm to 6.3 mm (p < 0.001). Of the 73 hips, 65 (89.0%) achieved satisfactory reduction or elimination of preoperative pain. In subgroup analysis for the sufficiency of femoroplasty (alpha angle < 55°), the clinical outcomes were not different between the two groups.
Conclusion:
Arthroscopic femoroplasty resulted in an 89% satisfaction at the 2-year follow-up. Therefore, hip arthroscopic femoroplasty might be an excellent alternative to open surgery and offers a greater probability of good to excellent results.
Introduction
Arthroscopic hip surgeries have been widely used for the treatment of hip disorders including labral tears and femoroacetabular impingement (FAI), which have traditionally been managed conservatively. 1 –7 Cam-type FAI, which is characterized as a subtle bony bump at the anterolateral femoral head–neck junction, leads to abnormal contact between the femoral head–neck junction and the acetabular rim, thus causing acetabular chondral delamination and variable degrees of labral pathology. 8 Cam-type FAI is usually diagnosed radiographically with asphericity of the femoral head that can be measured using the alpha angle, as described by Notzli et al. 9
Successful arthroscopic femoroplasty in patients with cam lesions have been reported in Western countries in the last two decades. However, the outcomes after arthroscopic femoroplasty in Asia have thus far only been reported in patients with borderline dysplasia 10,11 and in the military population. 12 Other studies in Asian countries focused on the prevalence of cam and FAI among Asian patients. Compared with the prevalence of 14–66% in Western patients with FAI including cam and pincer lesions, 13,14 the prevalence in Asian patients seems relatively lower (range, 0.5–51.5%). 15 –17 In addition, the different lifestyles of Asian populations, such as sitting in the tailor or cross-legged position, may cause a difference in outcomes compared with Western populations.
Therefore, this retrospective study was designed to evaluate the outcomes after arthroscopic femoroplasty in Asian patients with cam lesions. This study aimed to evaluate the short-term clinical outcomes, including visual analog scale (VAS) for pain, University of California Los Angeles (UCLA) activity scale, and modified Harris hip score (mHHS), and radiologic outcomes after hip arthroscopy in patients with cam-type FAI at a minimum postoperative follow-up of 2 years. In addition, we performed subgroup analysis of clinical outcomes and the sufficiency of femoroplasty (postoperative alpha angle, ≤55°) 18,19 of cam lesions during the follow-up period. The hypothesis of this study was that arthroscopic femoroplasty of cam lesions would improve the symptoms, function, and satisfaction level in these patients.
Methods
Patients
The design and protocol of this study were approved by the institutional review board at the hospital of the corresponding author. The requirement for informed consent was waived.
From January 2013 to December 2016, a total of 204 hip arthroscopic surgeries were performed. Of these cases, 62 patients (73 hips) underwent hip arthroscopy for cam-type FAI. The inclusion criteria were radiographic and intraoperative findings consistent with cam-type FAI and a minimum follow-up of 2 years. The exclusion criteria were traumatic labral tears without evidence of FAI, pincer-only FAI, revision surgery, previous hip conditions such as acetabular dysplasia, Legg–Calvé–Perthes disease, avascular necrosis, and prior surgical intervention (Figure 1).

Flowchart of the study. FAI: femoroacetabular impingement.
The indications for surgery were hip pain, mainly inguinal pain with associated mechanical symptoms and intractable pain after nonsurgical treatment for at least 3 months. On physical examination, all patients had a painful range of motion and a positive impingement test (i.e. pain was induced with passive sequential flexion, adduction, and internal rotation). Preoperative imaging included plain radiographs (pelvic anterior–posterior, modified Dunn, and frog-leg views) and computed tomography arthrography or magnetic resonance arthrography to detect bony impingement and labral tear. The final diagnosis of a cam lesion was confirmed using fluoroscopic imaging at the onset of the operative procedure to determine asphericity of the femoral head. In the subgroup analysis according to the diagnostic criteria of cam (alpha angle > 55°), the complete and incomplete resection groups were defined and compared according to clinical outcomes and satisfaction at a minimum 2-year follow-up.
Surgical procedure
Hip arthroscopy was performed with the patient in the supine position on a standard fracture table. Traction was applied with slight extension and adduction of the hip joint, with enough force to open the joint by approximately 1 cm. Two or three portals were placed on the anterolateral, anterior, and/or posterolateral portals. Transverse interportal capsulotomy without a T-incision was performed from 12 o’clock to 2 o’clock, approximately 5–8 mm from the labrum by using an arthroscopic scalpel (approximately 4 cm in length). Fluoroscopic imaging was used to identify the positioning of instruments and to help define the extent of each cam lesion with internal and external rotation. Acetabuloplasty and repair of the torn labrum were performed simultaneously, and femoroplasty (Figure 2) was performed after labral repair.
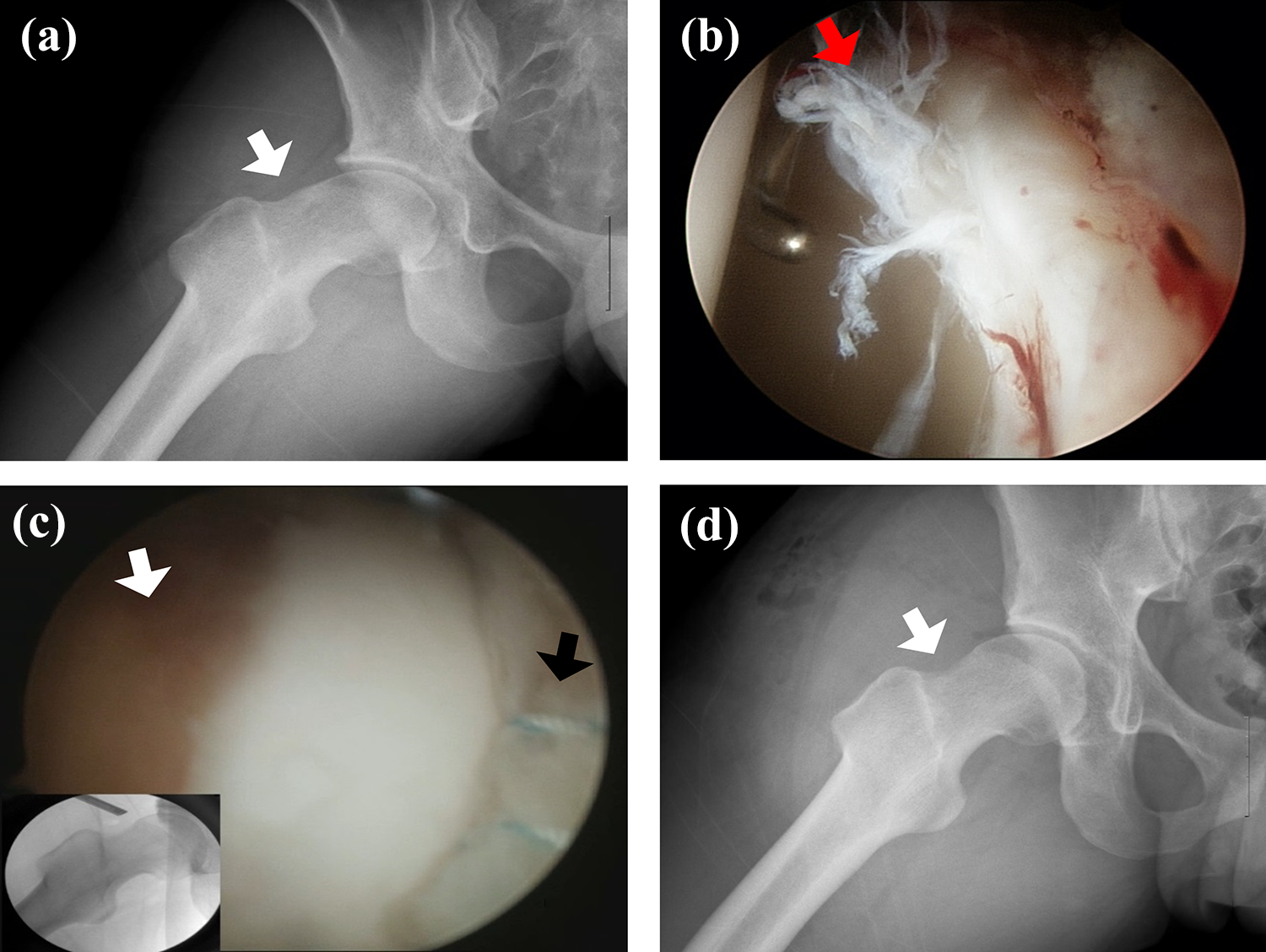
Cam lesion and labral tear in a 20-year-old man. (a) The cam lesion (white arrow) was seen on the preoperative modified Dunn view. (b) The labral tear lesion was seen through the arthroscopy (red arrow). (c) Arthroscopic labral repair (black arrow) and femoroplasty (white arrow) were done under C-arm image intensifier guidance. (d) Postoperative plain film in modified Dunn view showing proper correction (white arrow) of the cam lesion.
A final assessment of residual cam was performed after releasing the traction device, and the femoral head was visualized throughout the full range of flexion and rotation. Capsular repair was not performed in any of the patients. The operation was completed with joint lavage and local anesthetic injection. All operations were performed by a single senior surgeon.
Clinical outcomes
Clinical and radiographic follow-up evaluations were performed at 6 weeks; 3, 6, and 12 months; and every 6 months thereafter. Patients who were unable to attend the follow-up evaluations were contacted via telephone to evaluate their recent status. Two nurses and two doctors identified and visited the nonresponders. Patient satisfaction was evaluated through an interview at the last follow-up. Clinical evaluations were performed using the VAS score, UCLA score, and HHS modified by Byrd and Jones, 20 and the satisfaction level was assessed using a self-administered survey. The patients’ satisfaction after arthroscopic surgery was assessed and scored from 0 to 10 points. In subgroup analysis for patient-reported satisfaction, we defined satisfaction as a score of ≥5 points and dissatisfaction as a score of <5 points.
Radiologic outcomes
All radiographs were independently reviewed by two orthopedic surgeons for the measurements of the alpha angle 9 and head–neck offset ratio, 21 and the preoperative and postoperative values were compared. The measurements were then cross-checked against each other for the final Tönnis grade, alpha angle, and head–neck offset. The Tönnis grades 22 at the preoperative period and at the latest follow-up were obtained on anteroposterior radiographs of the pelvis. The alpha angle (abnormal value, >55°) 18,19 was measured between a line from the center of the femoral head through the middle of the femoral neck and a line through a point where the contour of the femoral head–neck junction exceeds the radius of the femoral head on an axial view. According to the reference range of the alpha angle (≤55°), a sufficient alpha angle was defined as ≤55° and an insufficient alpha angle was defined as >55°.
Rehabilitation protocol
All patients followed a standardized rehabilitation program after the operation. Immediately after surgery, passive and active range of motion was permitted. Patients were allowed toe-touch weight bearing on the affected side for 2 weeks, during which range of motion was encouraged but extremes of external rotation were avoided. In general, the patients typically required 2–3 weeks of crutch assistance.
Statistical analyses
The difference between preoperative and postoperative outcome measures were analyzed using paired t-tests for the pain VAS score, UCLA score, and mHHS for clinical outcomes and alpha angle and head–neck offset for radiologic outcomes. The numeric outcome measures were analyzed using the t-test or Mann–Whitney U test, and categorical outcome measures were analyzed using the χ 2 test or Fisher exact test. All statistical hypothesis tests were two-sided, with p < 0.05 considered statistically significant. For statistical analyses, we used SPSS Statistics 22.0 for Windows (SPSS, Chicago, Illinois, USA).
Results
There were 56 men (65 hips) and 6 women (8 hips) with a mean age of 31.4 ± 9.4 years at the time of index hip arthroscopy. Of the procedures, 37 were performed on the right side and 36 on the left side. The mean body mass index was 23.7 ± 3.1 kg/m2. Femoroplasty in 73 hips (100%) and labral repair in 53 hips (72.6%) were performed. The operation time was 116.3 ± 30.8 min (range, 50–190 min), and the length of hospitalization was 7.4 ± 5.1 days (Table 1).
Demographic characteristics.a

No.: number; SD: standard deviation; BMI: body mass index.
a Data are reported as n (%) or mean ± SD.
Although most clinical outcomes were improved at 1-year follow-up, they continuously improved over the study period. In the clinical outcomes, improvements in scores from before surgery to the last follow-up were observed, as follows: 67.1 ± 15.0 to 90.2 ± 6.3 for the mHHS (p < 0.001), 4.7 ± 2.5 to 7.1 ± 1.4 for the UCLA score (p < 0.001), and 7.4 ± 1.9 to 1.8 ± 1.5 for the VAS score (p < 0.001) (Table 2; Figure 3).
Clinical outcomes including the mHHS, UCLA score, and VAS score showed continuously significant improvement during the study period (p < 0.001).

mHHS: modified Harris hip score; UCLA: University of California Los Angeles activity score; VAS: visual analog scale for pain.

Flowchart of clinical outcomes. Pre-op.: preoperative period; mHHS: modified Harris hip score; UCLA: University of California Los Angeles activity score; VAS: visual analog scale.
In radiologic assessments, the mean alpha angle and head–neck offset in the preoperative period and at the latest follow-up were improved from 60.9° and 3.3 mm to 49.5° and 6.3 mm, respectively. However, the mean alpha angle in 21 hips was >50°. The preoperative Tönnis grades were evaluated in all patients, with the following results: 31 hips (44.5%) were grade 0; 39 hips (53.4%), grade 1; and 3 hips (4.1%), grade 2. Of these, 56 (76.7%) had no change in the Tönnis grade. The Tönnis grade changed from grade 0 to 1 in 9 patients, from grade 1 to 2 in 7 patients, and from grade 2 to 3 in 1 patient. These patients underwent conversion to total hip arthroplasty replacement at 1-year follow-up. Of the 73 hips, 65 (89.0%) achieved satisfactory reduction or elimination of preoperative pain.
In addition, of the 73 hips, 52 had an alpha angle of ≤55° (sufficient group) and 21 hips had an alpha angle of >55° (insufficient group) on postoperative radiographic assessments. In subgroup analysis, although patients with insufficient surgical correction (21 hips) were younger than patients with sufficient correction, the clinical outcomes were not different between the two groups (Table 3).
Comparisons of clinical outcomes between the sufficient group (alpha angle ≤ 55°) and the insufficient group (alpha angle > 55°).a
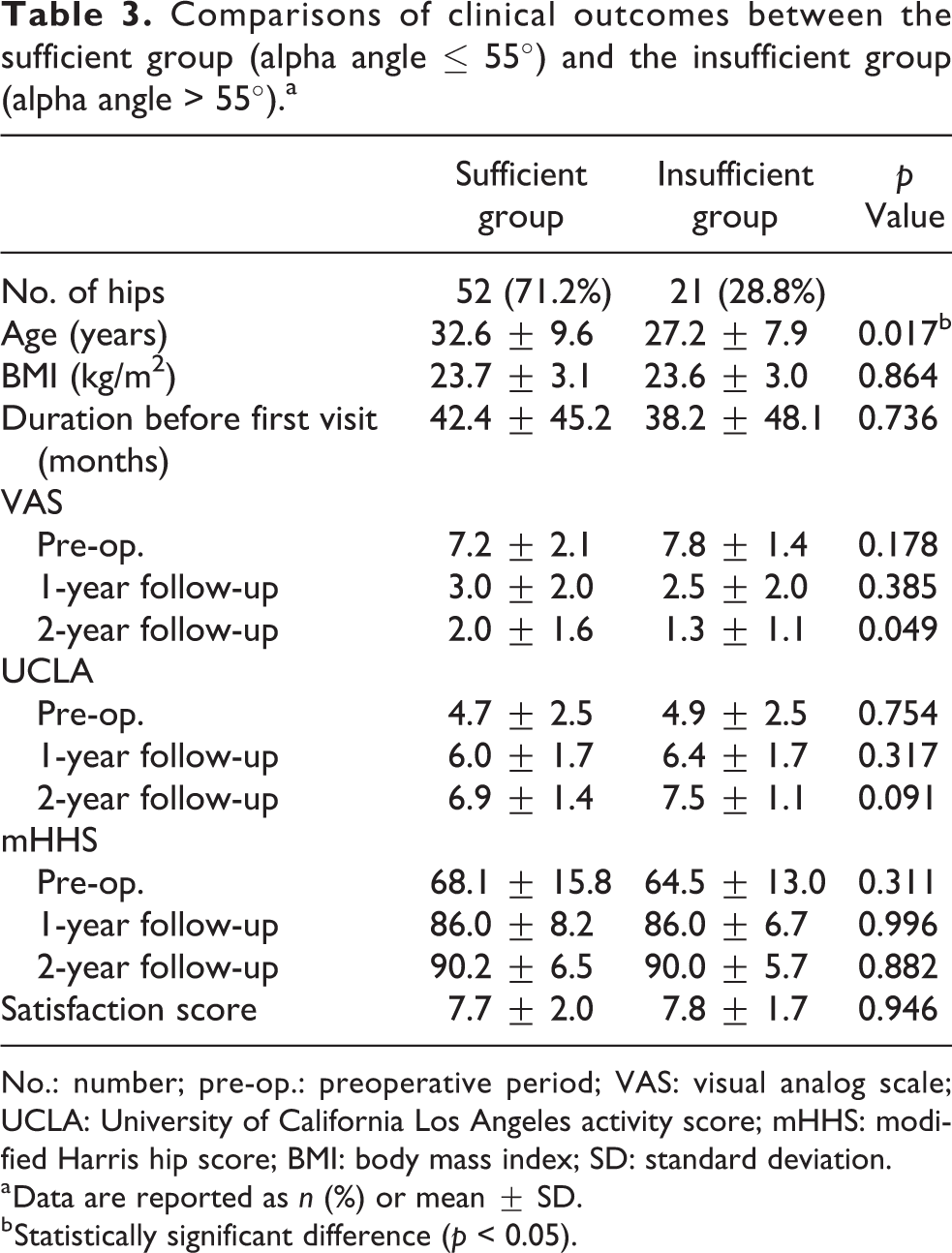
No.: number; pre-op.: preoperative period; VAS: visual analog scale; UCLA: University of California Los Angeles activity score; mHHS: modified Harris hip score; BMI: body mass index; SD: standard deviation.
a Data are reported as n (%) or mean ± SD.
b Statistically significant difference (p < 0.05).
Three patients complained of transient pudendal nerve palsy but recovered within 6 weeks. No relevant complications, such as infection, heterotopic ossification, thromboembolic episodes, or permanent nerve injury, occurred at the latest follow-up.
Discussion
The principal findings of this study were that arthroscopic treatment of cam-type FAI in 73 hips improved clinical outcomes and 52 hips had sufficiently normalized femoral bump (≤55°) at a minimum postoperative follow-up of 2 years. At the latest follow-up, 89% of the patients with cam-type FAI reported being satisfied with the procedure. Comparing the 52 hips in the sufficient femoroplasty group with the 21 hips in the insufficient femoroplasty group, the patients’ satisfaction and clinical outcomes, including VAS score, UCLA score, and mHHS, were not different at the latest follow-up.
Studies on outcomes after arthroscopic treatment in patients with FAI have reported satisfaction rates of 68% to 100% in the last two decades. 23 Khan et al. 24 reported clinical outcomes after reviewing 104 studies related to hip arthroscopy for FAI. They reported that the pooled weighted mean mHHS values after arthroscopic surgery for FAI showed improvements in the mid-term period from 60.5 points (range, 56.6–83.6 points) to 80.5 points (range, 72.1–98.0 points) out of the possible 100 points. 24 Minkara et al. 25 performed a meta-analysis including 1911 patients from 31 studies and reported the outcomes after the arthroscopic management of FAI. They reported that 87.7% of the patients were able to return to sport after surgery and that all patient-reported outcomes improved postoperatively, with the highest increase observed in the Hip Outcome Score-sports scale and the alpha angle decreased by an average of 23.6°. 25 According to previous studies, arthroscopic intervention in patients with FAI could improve clinical outcomes and allow recovery of physical activity in the short-term and mid-term follow-up periods. These findings corresponded with the results of this study. In this study, the mean mHHS after arthroscopic surgery for cam lesions showed an improvement from 67.1 points to 90.2 points at a minimum 2-year follow-up. In addition, the patient-reported satisfaction rate was 89% at the latest follow-up and was related not to radiologically sufficient correction of the alpha angle and offset but to clinical outcomes including the VAS score, mHHS, and UCLA score.
Thus far, two papers on the outcomes after arthroscopic surgery in Asian patients with FAI have been published. One case–control study performed arthroscopic surgery in 47 athletes and 27 nonathletes with FAI and reported improved mHHS (95.4 and 88.2, respectively) at a minimum follow-up of 2 years. Yoo et al. 12 performed a comparison study between 28 military personnel and 28 civilians, and reported improvement of the mHHS (89.9 and 91, respectively), UCLA score (9.4 and 8.4, respectively), and VAS score (2.6 and 2.2, respectively) at a minimum follow-up of 2 years. Although a direct comparison between previous Asian studies and the present study might be difficult because of the different study designs, patient characteristics, and surgical indications, arthroscopic surgery after FAI in Asian patients is a promising method that offers better outcomes at a minimum follow-up of 2 years. The present study focused on patients with cam-type FAI. This study group is relatively rare in Asian populations. According to an epidemiologic study on the prevalence of FAI, the prevalence of FAI-related morphologic features in Asian countries is lower than that in Western countries. 15,26,27 Despite of low incidence of cam-type FAI, different physical activity like sitting cross-legged, kneeling, squatting may be more inconvenient than Western countries. Nevertheless these differences, hip arthroscopy with femoroplasty for FAI is recommendable surgical procedures in Asian patients because functional outcome and satisfaction after arthroscopic femoroplasty are remarkable.
Incomplete femoroplasty in cam lesions of FAI is the main cause of revision surgery and is related to poor clinical outcomes. Urquhart et al. 28 performed a systematic review of 14 comparable studies and reported that precise surgical restoration of the alpha angle in cam-type FAI required a minimum angle of <55°, which influenced the improvements of patient outcomes. However, our findings did not correspond with those of other studies. In a subgroup analysis of this study comparing the clinical outcomes between the sufficient group (≤55°) and the insufficient group (>55°), the clinical outcomes were not different at a minimum follow-up of 2 years. This might be related to the severity according to the clinical score and alpha angle at the index operation. In addition, the follow-up duration was too short to draw conclusions about the effect of incomplete resection of cam lesions. Therefore, studies with a long-term follow-up are needed to confirm the effect of incomplete resection of cam lesions of FAI.
This study has several limitations. First, there was no control group, the sample size was small, and this was a retrospective single-center study. However, a priori power analysis was completed to calculate the number of patients necessary in each group to realize a minimum of 80% power using a 1:1 matching ratio. Based on an expected mean difference in the mHHS of 10 points, the power analysis determined that 63 patients would be required for each group. 29 Therefore, this study might be proven the value of arthroscopic procedures with femoroplasty for cam-type FAI. Second, the learning curve of hip arthroscopy for FAI is challenging, and the results are related to the level of surgeon experience. Equivalent outcomes may not be attainable for surgeons with less experience. Third, the mHHS used in this study was simply translated into the Korean language, because no Korean version of the mHHS has been validated yet. In the future, validation and cross-cultural adaptation of the Korean version of the mHHS will be necessary to assess the clinical outcomes after hip arthroscopy in Korean patients. Finally, the preoperative patient expectations were not evaluated. However, we evaluated the satisfaction rate at a minimum follow-up of 2 years and confirmed the obtained rate of 89%.
In conclusion, arthroscopic femoroplasty resulted in an 89% satisfaction rate at the 2-year follow-up. Therefore, hip arthroscopy with femoroplasty might be an excellent alternative to open surgery and offers a greater probability of good to excellent results.
Footnotes
Authors’ note
Yong-Chan Ha and Jae-Young Lim contributed equally to this work and should be considered co-first authors.
Acknowledgment
The authors in this study express our sincere appreciation for all the patients to join this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.