
Abstract
Wilson’s disease (WD), an autosomal recessive disorder of copper metabolism, may develop complex foot and ankle deformity associated with gastrosoleus muscle complex spasticity. In this case report, we present a female WD patient with bilateral equinocavovarus foot deformity in which the right foot deformity was progressed with severe contracture of posteromedial hindfoot structures and manifested as a rigid deformed foot. One-stage correction surgery including modified Lambrinudi arthrodesis, posterior tibialis tendon transfer to the lateral column of the foot, plantar fascia release (Steindler release), and Achilles tendon lengthening procedures was performed. Shortening the treatment period and decreasing possible complications due to multiple procedures are the main benefits of this technique. Although the limitation is that only a single patient was enrolled, this study provides a practical and reasonable surgical procedure with a satisfactory outcome.
Introduction
Wilson’s disease (WD) is an autosomal recessive disorder of copper metabolism. 1,2 With a global incidence of 1:30,000, it results from malfunction of a copper-transporting ATPase caused by ATP7B gene mutations on the long arm of chromosome 13. 2,3 Toxic copper accumulates in body tissues, mainly the liver and central nervous system. Chronic liver injury and cirrhosis, neurologic impairment, and corneal Kayser–Fleischer rings are the classical clinical manifestations of WD, 4 and neurologic features including tremors, dystonia, parkinsonism, drooling, and dysarthria typically begin in the second or third decades of life. 5,6 Some patients may have severe and painful dystonia that can develop into limb contractures over time. 2
Magnetic resonance imaging (MRI) is known as a useful image examination to WD. The characteristic brain MRI includes midbrain “Panda sign” which is represented as preservation of substantia nigra and red nucleus surrounded by high T2 signal change in the tegmentum. 7,8 Electrophysiological study was also demonstrated as an effective diagnostic tool for discrimination of the disease severity and also the specific part of neurological involvement such as extrapyramidal tract or even pyramidal damage. 9 The neurologic manifestation of the WD has a wide variety of clinical presentation. The most common foot and ankle deformity resulting from neurologic impairment is intrinsic muscle weakness and rigidity. 10 Neurogenic cavovarus foot is the imbalance of the longstanding muscles. Charcot–Marie–Tooth disease, post-poliomyelitis syndrome, and cerebral palsy are the most illustrated diseases. 11 Coexisted with an equinus deformity as equinocavovarus deformity is relatively rare and is correlated to the spasticity in the gastrosoleus muscle complex. 12,13 This complex deformity manifests as a combination of ankle equinus, midfoot cavovarus, and adduction of the forefoot. Painful discomfort and decreased stability in the stance phase of gait due to weight-bearing only on the lateral column can affect walking ability and activities of daily living. 12,13 Equinus deformity was occasionally reported in the WD, especially with a rigidity or dystonia at the ankle joint, and sometimes associated with drop foot due to peripheral neuropathy. 14,15 Nevertheless, equinocavovarus was not found in the literature review.
The therapeutic strategy for equinocavovarus deformity is based on the severity of the deformity. Passive reducible deformity can be treated less invasively, such as with oral and intrathecal medications, intensive rehabilitation with the use of a brace, botulinum toxin injections, and selective neurotomy. Failed conservative treatment and rigid deformities can be managed with a combination of selective surgery including tendon transfer, talectomy, calcaneal osteotomy, dynamic corrective osteotomy using a hinged distraction apparatus (Ilizarov external ring fixator), and triple arthrodesis. 13,16 –18
Herein, we present a case of equinocavovarus deformity in a patient with WD who was treated with one-stage correction surgery including modified Lambrinudi arthrodesis, posterior tibialis tendon transfer to the lateral column, plantar fascia release (Steindler release), and Achilles tendon lengthening procedures.
Case presentation
The use of human data was reviewed and approved by the Institutional Review Board of the hospital (09-CR-015). Written informed consent was provided by the patient. A 24-year-old female presented to our outpatient department with the chief complaint of right foot deformity with pain. Her medical history was significant for WD which had been diagnosed when she was 19 years old based on clinical features, biochemical parameters, ATP7B genetic test, and brain MRI survey (Figure 1), with the symptoms of clumsiness of her right limbs and intermittent hand tremors. The T2-weighted axial MR image showed generalized cerebral atrophy, as well as bilateral symmetric laminar hyperintensity in basal ganglion with central dark signal intensity which is due to heavy metal deposition (Panda sign; Figure 2). 13 Besides from basal ganglion degeneration, there is also evidence of bilateral pyramidal tracts (corticospinal tracts) involvement as abnormal hyperintense signal in posterior limb of internal capsule (Figure 2). Initial treatment includes the prescription of penicillamine (1000 mg/day) for 3 months and then shifted to trientine (900 mg/day). Despite treatment, weakness in all four limbs and dystonia gradually progressed, with rigidity and the subsequent development of dysphagia, nonambulatory status, and dysarthria (15, 28, and 30 months after disease onset, respectively). In addition, a severe foot deformity prevented weight-bearing and restricted her to a wheelchair. She had been almost housebound.

ATP7B mutation analysis of our patient. A heterozygous mutation c.1708-1 G>C of the ATP7B gene with clinical association was found.
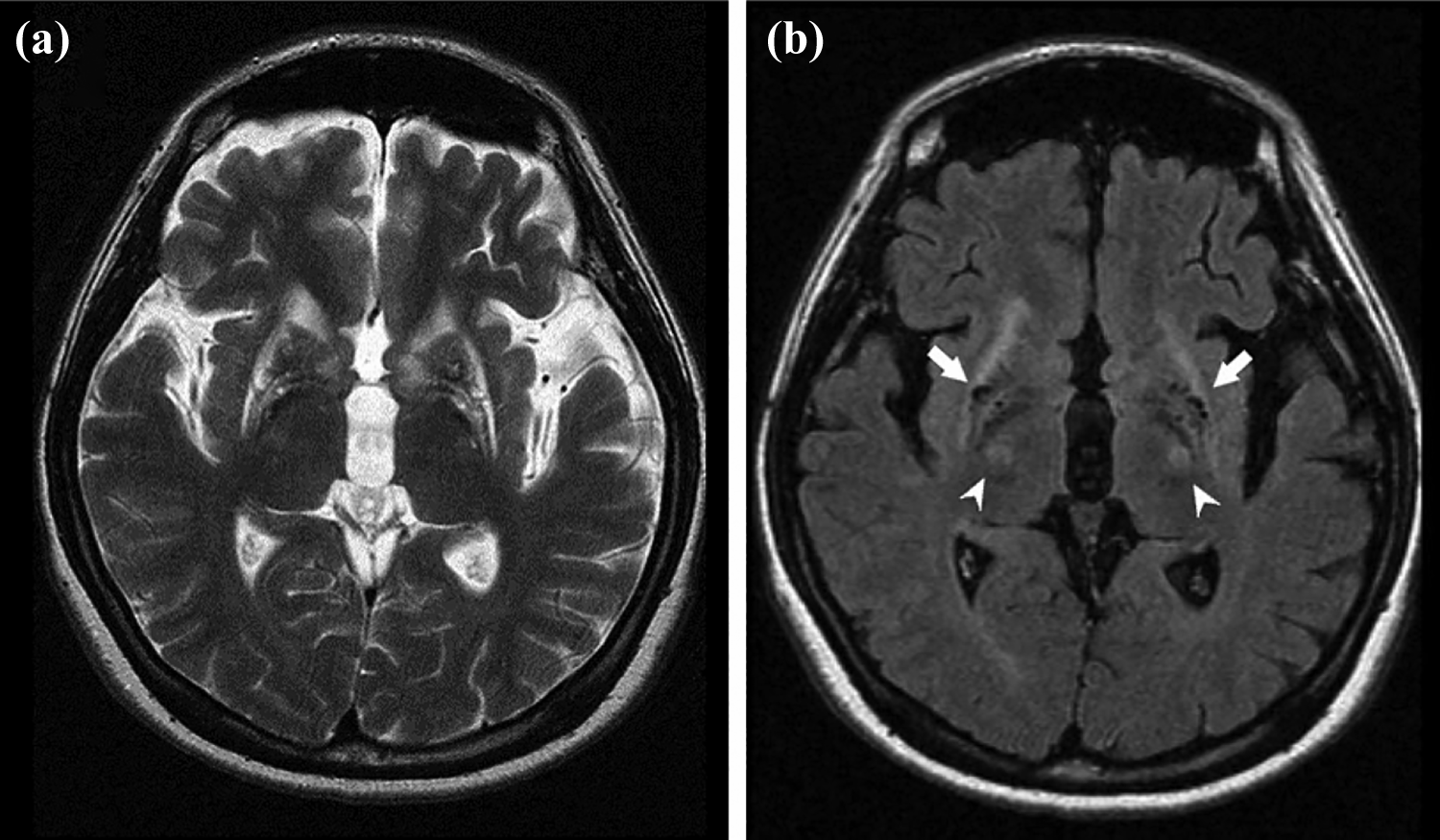
(a) Axial T2-weighted MR image shows bilateral symmetric laminar hyperintensity in basal ganglion, with central dark signal intensity which indicates increased heavy metal deposition. Generalized cerebral atrophy is also present. (b) Axial T2-FLAIR MR image shows involvement of bilateral pyramidal tracts (or corticospinal tracts) as abnormal hyperintense signal in posterior limb of internal capsule (arrowheads). The dark signal intensity in bilateral globus pallidus and putamen are due to heavy metal deposition (arrows). MR: magnetic resonance.
Although she had bilateral equinocavovarus foot deformity, the right foot deformity was aggravated with severe contracture of posteromedial hindfoot structures and manifested as a rigid deformed foot. The influence of neurologic deficits on her left foot was relatively minor and manifested as a flexible deformity which could be reduced passively. Initially, conservative treatment was prescribed due to the patient’s concern over complications of surgical correction. For her right foot contracture deformity, H. Botox injections in the right tibialis posterior muscle (20 U) and right gastrocnemius (30 U) were given, but no obvious improvements were seen. The physical therapy and serial bracing rectification failed owing to the high intensity of limb spasticity. Consequently, a surgical intervention was proposed to correct the right foot deformity.
Clinical condition
The initial evaluation of the affected extremity revealed a severe equinus deformity of the right ankle with internal rotational contracture of the foot. A left foot flexible deformity was also noted, and the malformation was rotated inward and downward (Figure 3(a) to (e)). The right limbs involvement was more severe than the left side in accordance with the severity of the equinocavovarus deformity.

(a and b) Clinical picture showing forefoot varus and inversion of the right foot. Appreciation of (c) equinus and cavus and (d and e) forefoot varus.
The muscle power was 4 over the proximal muscles of the right upper limb and 3 at the distal right lower limb. Single tendon function of the right foot was also assessed to evaluate the feasibility of the preoperative surgical option of a soft tissue procedure. Tightened heel cord and contracture of the posterior tibialis tendon were the major forces leading to the foot deformity. The peroneal brevis tendon and anterior tibialis tendon were paralyzed. The peroneal longus tendon, which is the antagonist of the anterior tibialis tendon, was still intact and preserves the ability for foot plantarflexion. To restore function of ankle dorsiflexion and subtalar eversion, transferring the posterior tibialis tendon to the lateral column of the foot was the most reasonable option. Achilles tendon lengthening and plantar fascia release were also paramount during surgery to assist the reconfiguration of a plantigrade foot.
The preoperative roentgenographic study showed a 129° right tibiocalcaneal angle (Figure 3) on lateral foot radiographs, indicating equinus. The calcaneal pitch angle was 39° and the lateral talus-first metatarsal angle was 64° (Figure 4), indicating pes cavus. A foot anterior-posterior (AP) radiograph showed that the talonavicular coverage angle was 38° and the AP talus-first metatarsal angle was 53° (Figure 5), indicating forefoot varus.

Foot lateral radiography (patient could not bear weight). (a) Tibiocalcaneal angle: 129°, (b) calcaneal pitch angle: 39°, and (c) lateral talus-first metatarsal angle: 64°.

Foot AP radiography. (a)Talonavicular coverage angle: 38° and (b) AP talus-first metatarsal angle: 53°. AP: anterior-posterior.
A careful preoperative investigation was performed, and computed tomography angiography of her lower extremities showed the normal appearance of bilateral lower limb arteries without vascular impedance.
Procedure
Surgery for her right deformed foot included modified Lambrinudi arthrodesis, posterior tibialis tendon transfer to the lateral column, Steindler plantar fascia release, and Achilles tendon lengthening. Her leg was disinfected with beta-iodine and carefully draped. After exsanguination, the minimally invasive Steindler procedure (plantar fascia release) and triple-cut Achilles tendon lengthening were performed. The operative field was then changed to the lateral hindfoot. One skin incision from the tip of the fibula to the fourth metatarsal base was made. The calcaneocuboid joint was opened, and closing wedge osteotomy was performed with a width of 8 mm. The talonavicular joint and subtalar joint were subsequently exposed. The inferior 1/4 portion of the naviculum and the inferior 1/3 part of the talus were osteotomized and removed, and the upper 1/5 part of the calcaneus was resected. Another skin incision was made on the medial aspect of the foot, and the talonavicular joint and subtalar joint were exposed to allow for denuding of the articular cartilage. Closing wedge correction with lateral base derotation was accomplished with the foot kept in a neutral position. Two X-locking plates and two 6.5-mm headless compression screws were fixed on the calcaneocuboid joint, the talonavicular joint, and the subtalar joint. The posterior tibialis tendon was transferred to the remaining anterolateral talar head and fixed with one Twinfix 3.5-mm suture anchor. The wounds were closed in layers. A short leg splint was used for external support.
Outcome
Bony union was investigated 3 months postoperatively according to radiographs. She then started rehabilitation, wearing orthotic shoes with custom made insoles and walking with a walker. At the most recent postoperative evaluation after 12 months of follow-up, no specific complications were noted. The radiographs revealed improved alignment of the joints, a right tibiocalcaneal angle of 34°, calcaneal pitch angle of 23°, and lateral talus-first metatarsal angle of 16° (Figure 6). The talonavicular coverage angle was around 0°, and the AP talus-first metatarsal angle was also 10° (Figure 7).
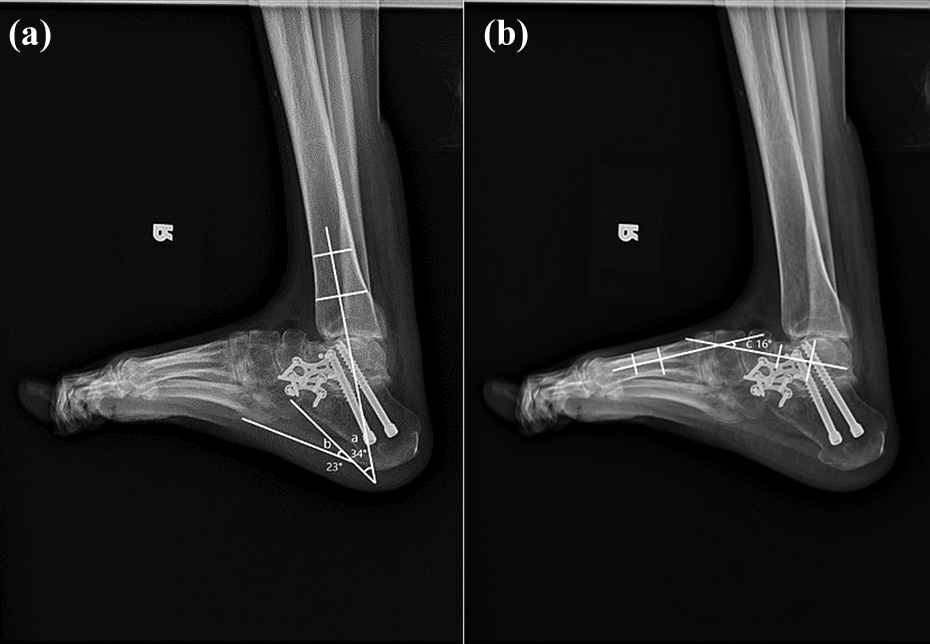
Foot lateral radiography. (a) Tibiocalcaneal angle: 34°, (b) calcaneal pitch angle: 23°, and (c) lateral talus-first metatarsal angle: 16°.
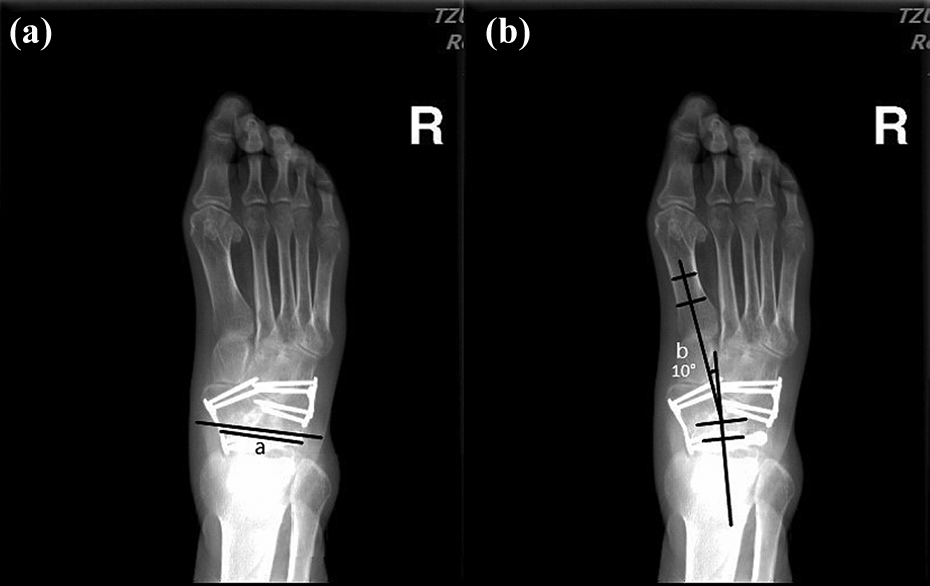
Foot AP radiography. (a) Talonavicular coverage angle: 0° and (b) AP talus-first metatarsal angle: 10°. AP: anterior-posterior.
Overall, she had improved function and activity with a plantigrade foot and could walk with the aid of a walker despite nonambulatory status for 4 years (Figure 8). She needed custom-made insole and shoe used for improving the gait pattern. Her home is at the second floor and now she can go upstairs and downstairs for taking some outdoor exercise. Walking distance is 500 m and then she needs to take a rest as desired before starting the next ambulance.

Clinical picture at 6 months postoperatively showed the patient got a plantigrade foot with a mild dorsiflexed ankle. Residual claw toe deformity can be visualized despite the plantar fascia release processed during surgery.
Discussion
WD is an autosomal recessive disorder of copper metabolism. 1,2 Neurologic symptoms such as dysarthria, dystonia, tremors, and parkinsonism may lead to severe disability if the disease is poorly controlled. In some patients with severe dystonia, limb contracture and deformity may develop, and surgical correction may be indicated in patients with disabling severe foot deformities.
Our patient developed dystonia, dysphagia, and dysarthria and could not walk due to severe right foot deformity. MRI examination revealed both extrapyramidal and pyramidal tract were involved. Although white matter involvement was observed in 10% of autopsy patients especially in Asian citizens and correlated to the pyramidal signs. 19 –22 The presentation of severe spastic contractures in our patient was not owing to the subcortical white matter. The signal change in the subcortical white matter of precentral gyrus (primary motor cortex) is not obvious. The evidence of pyramidal tract (corticospinal tract) involvement in this case was shown as abnormal hyperintensity signal change in posterior limb of internal capsule. Equinocavovarus foot is one of the presentations of severe spastic contracture and has been reported in some neurogenic conditions such as clubfoot and spastic foot after stroke. The management strategies including conservative treatment and surgical correction have been proposed. 13,16 –18 However, conservative treatment such as oral medication, rehabilitation, the use of a brace, and botulinum toxin injections were all used in our patient, but without significant improvements.
Surgical methods including soft tissue balancing, tendon transfer, talectomy, calcaneal osteotomy, dynamic correction using a hinged distraction apparatus, and triple arthrodesis have been used to manage the equinocavovarus deformity. 13,16 –18 Soft tissue balancing such as Achilles tendon lengthening, tendon transfer, or release of the plantar fascia may be effective enough in cases with less neurological involvement with a flexible foot deformity such as in the left foot of our patient. In comparison, the right foot of our patient had a severe, fixed, equinocavovarus deformity involving the bone which required an additional extensive bony procedure to achieve thorough correction. Fixed equinovarus deformities are more often reported in cerebral palsy patients, and they cannot tolerate gradual correction with external fixation frames due to strong spasticity. Other disadvantages of external fixation include wire dislodgment, a high incidence of pin site infection, and recurrence of the deformity. 23 –26 The rigidity and complexity of equinocavovarus deformity often requires more extensive procedures such as multiple osteotomy or Lambrinudi triple arthrodesis. 26 –28
In our patient, we chose modified Lambrinudi arthrodesis due to its high efficiency in correcting deformities considering three dimensions. The correction obtained in Lambrinudi arthrodesis is created with closing wedge osteotomy. The osteotomy excises the inferior portion of the head and neck of the talus. The bony resection begins at the upper third of the talar head and inclines toward the posterior process of the talus and toward the inferomedial part of the talus. Minimal bony resection of the calcaneus, limited joint preparation of the talonavicular joint and calcaneocuboid joint were accomplished, and an anterolaterally based wedge from the head and the neck of the talus was achieved after removal of the resected bone. The difference from the traditional Lambrinudi procedure is that the talar head was not excised thoroughly in our method. The reason for preserving the upper part of the talar head was so that the foot length would not be shortened too much after deformity correction. Another modification was that the shape of the wedge was anterior and lateral based, which is different from the anterior base only of the traditional method. A double based wedge can achieve a better plantigrade foot by eversion of the hindfoot and dorsiflexion of the midfoot simultaneously.
Conclusion
We report our experience of treating equinocavovarus deformity, a rare neuromuscular presentation in a patient with WD, with one-stage correction using modified Lambrinudi arthrodesis with additional soft tissue procedures. Shortening the treatment period and decreasing possible complications due to multiple procedures are the main benefits of this technique. This study provides a practical and reasonable surgical procedure with a satisfactory outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.