
Abstract
Purpose:
The asymmetry of muscular strength after anterior cruciate ligament reconstruction (ACLR) is associated with increase in the development of new lesions. This asymmetry is precisely assessed by isokinetic dynamometry which is a high-cost technique, limited to major centers and hospitals. Thus, the aim of this study was to test the accuracy of one of the most frequently used functional questionnaires, the Lysholm score, to diagnose the knee torque deficit.
Methods:
In total, 115 patients were evaluated after ACLR. Knee symptoms were evaluated using the Lysholm questionnaire and knee extensor and flexor peak torque during maximal isokinetic concentric contractions at 60° s−1 (5 repetitions) and 180° s−1 (15 repetitions). Patients with <20% peak torque deficit were considered symmetric (normal).
Results:
An increase in the Lysholm score was associated with a deficit reduction in the peak torque of knee extensors at 60° s−1 (r = −0.294) and 180° s−1 (r = −0.297) (p < 0.05 for both). Cutoff Lysholm scores of >90 points for 60° s−1 allowed the correct diagnosis of symmetry in 71% and of >89 points for 180º·s−1 allowed the correct diagnosis of symmetry in 73%, for knee extensors. Patients with a Lysholm score of >89 points presented an isokinetic deficit 36% lower than patients with a Lysholm score of ≤89 points (p < 0.05).
Conclusion:
A Lysholm score of >89 points has predictive value for deficits in the peak torque of knee extension (<20%). However, replacement of the isokinetic evaluation by this instrument must be performed with caution because of its accuracy.
Introduction
Anterior cruciate ligament injuries are common among active young patients, and surgical treatment is frequently performed to allow the return to play (RTP). After the anterior cruciate ligament reconstruction (ACLR), the duration from rehabilitation to RTP can vary from 12 weeks to 12 months.1, 2 Several criteria and evaluation tools have been used to assess RTP after ACLR, including the post-surgery time, ligament stability, functional questionnaires, dynamic tests, and isokinetic evaluation. 1,2
Objective evaluation of the quadriceps asymmetry muscle strength after ACLR provides important data for determination of the RTP condition. 3 Moreover, an asymmetry (deficit) in muscular strength after ACLR is associated with an increase in the development of new lesions. 4 The isokinetic evaluation has been used in the last few decades to evaluate muscular strength and balance, 5 and it is a precise measurement method for such evaluations. 6 However, because of the high cost and training involved in isokinetic evaluation, this technique is limited to major centers and hospitals and is not available to all patients. 3,7
The Lysholm score is one of the most frequently used functional questionnaires. This questionnaire allows for evaluation of the functional limitations caused by knee disorders through eight questions, is low-cost and easy to apply, requiring little time to perform. 8
Considering that minimization of deficits of muscular strength in the knee joint after ACLR can provide safer RTP and that precise isokinetic evaluation of these deficits is not accessible to all clinical practices, the aim of the present study was (1) to investigate the association between the Lysholm score and muscular strength deficits in the knee and (2) to assess the accuracy of the Lysholm questionnaire as a tool to predict the diagnosis in the absence of peak torque deficit of >20% after ACLR.
Materials and methods
Participants
In total, 115 adult patients (Table 1) who underwent isokinetic evaluation of knee extension and flexion and completed the Lysholm questionnaire after ACLR were included in this study. Hamstrings or patellar tendon graft were applied in all cases. The minimum time until performance of the evaluations was 4 months postoperatively. Patients who underwent anterior cruciate ligament revision and those with a contralateral knee lesion were excluded. This research project was approved by the regional Ethics Committee in Research (protocol number 995/2011). All participants provided written informed consent to participate.
Characteristics of studied patients (n = 115).a

PT Ext: peak torque extensor; PT Flex: peak torque flexor.
a Data are mean (± standard deviation), median (interquartile interval), and frequencies, respectively.
Lysholm questionnaire
All patients read and completed the Lysholm questionnaire 8 with no external interference by the evaluators. Lysholm score allows for evaluation of the functional limitations, and the sum obtained in each of the eight questions was considered for further analysis. The total score points vary from 0 (worst result) to 100 (best result).
Isokinetic evaluation
The isokinetic evaluation of the extensor and flexor articular peak torque of the knee was measured by an isokinetic dynamometer (System 4 Pro; Biodex, Shirley, New York, USA). The positioning of the patients in the dynamometer, the preparation and calibration of the equipment were conducted according to the manufacturer’s instructions.
During the evaluation, the patients were seated with chest inclination fixed at 85° and hips flexed at 90°. The dynamometer lever arm was positioned parallel to the leg, aligning the lateral femoral condyle of the tested leg with the rotation axis of the dynamometer. Distally, the leg was fixed immediately over the lateral malleolus of the ankle. The patient was stabilized in the dynamometer chair by belts fixed at the chest, hips, and thigh (distal third of the tested limb) to avoid compensatory movements. The gravity force was corrected once the patient’s performance in the test implied completion of the movement against gravity. During the test, the patient was constantly stimulated verbally and received visual feedback regarding the tested muscular group activity through the monitor coupled to the dynamometer.
Before the evaluation, the patients executed four submaximal repetitions for familiarization and warming purpose. 9 The evaluation was performed in the unaffected limb followed by the affected limb during 5 repetitions of maximum isokinetic concentric contractions of knee extension and knee flexion at 60° s−1 followed by 15 repetitions at 180° s−1. A 3-min interval was allowed between the movement velocities. 9 The higher peak torque recorded during the knee extension and flexion movements at each tested speed was considered for analysis. The 28 patients who were within the 4- and 5-month postoperative period did not perform the evaluations at 60° s−1 to avoid overloading the graft during knee extension at low speed.
Statistical analysis
The data distribution was verified using the Shapiro–Wilk test. Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables are presented as absolute and relative frequencies of occurrence. The association between the Lysholm score and the module of the peak torque deficit ((affected limb/unaffected limb) × 100) was assessed with the Pearson correlation test followed by simple linear regression to obtain the explained variance. The ability of the Lysholm questionnaire to accurately diagnose patients with absence of a peak of torque deficit of knee extension and flexion of <20% was verified by calculation of the true-positive rate (sensitivity) and true-negative rate (specificity), construction of a receiver operating characteristic (ROC) curve, and analysis of the area under the ROC curve (AUC) and its 95% confidence interval. The AUC was classified as “perfect” (AUC = 1), “excellent” (0.9 ≤ AUC < 1), “good” (0.8 ≤ AUC < 0.9), “reasonable” (0.7 ≤ AUC < 0.8), or “poor” (AUC < 0.7); an AUC of ≤0.5 was considered not statistically different from that obtained randomly. Finally, using the cutoff Lysholm score obtained in the ROC curve analysis, the peak torque deficit was compared between patients with values higher and lower than the cutoff value using the Mann–Whitney U test. All analyses were conducted using the software PASW Statistics 18.0 (SPSS Inc., Chicago, Illinois, USA) with a significance level (α) of 5% (p < 0.05).
Results
Sample description
The patients’ characteristics are shown in Table 1.
Association between Lysholm score and peak torque deficit
A negative correlation was found between the total Lysholm score and the peak torque deficit of knee extension at 60° s−1 (r = −0.294) and at 180° s−1 (r = −0.297); 8.7% and 8.8% of the variance in torque deficit at 60° s−1 (p = 0.006) and at 180° s−1 (p = 0.001), respectively, could be explained by the variance in the Lysholm score. In other words, for each one-point decrease in the Lysholm score, an increase in the peak torque deficit of 0.32% at 60° s−1 and 0.24% at 180° s−1 was expected (Table 2).
Regression coefficients, p values, confidence limits, and variance explained by Lysholm score predictors.
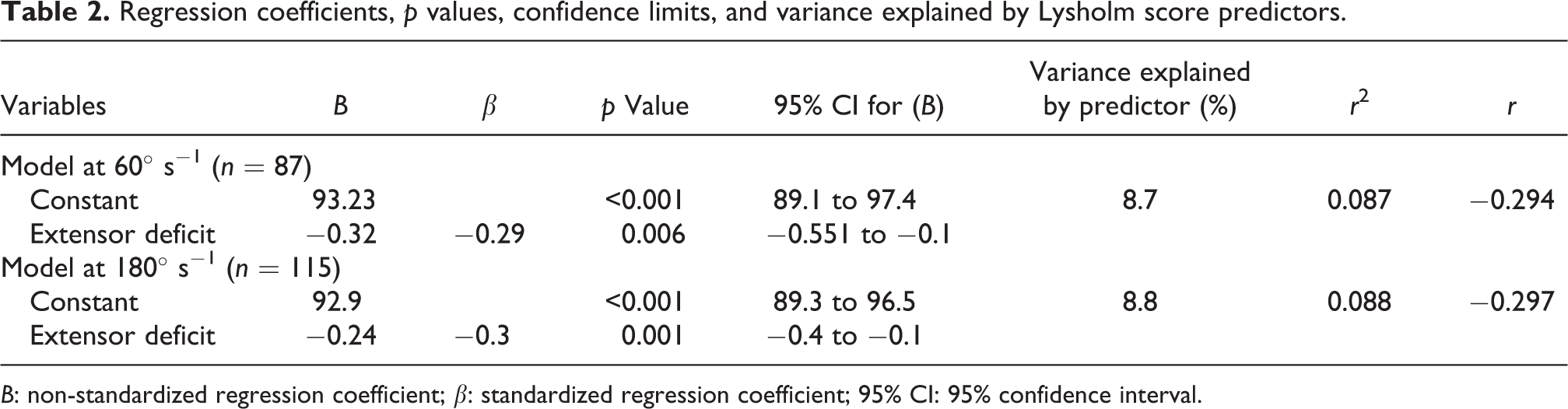
B: non-standardized regression coefficient; β: standardized regression coefficient; 95% CI: 95% confidence interval.
Accuracy of Lysholm score for prediction of absence of muscular deficit
The ROC curve analysis showed that the Lysholm score had a better power of prediction for a muscular deficit of <20% for knee extension compared with flexion at both tested velocities (Figure 1).

ROC curve analysis of the Lysholm score as a predictor of muscular deficits of knee extension and flexion at 180° s−1 (n = 115) and 60° s−1 (n = 87). The AUCs are presented with the 95% confidence interval. The symbol “•” represents the cutoff suggested for discharge of patients with muscular deficits of <20%, with the respective values of sensitivity and specificity. ROC: receiver operating characteristic; AUC: area under the curve.
For knee extension at 60° s−1 and at 180° s−1, the ROC curves showed that cutoff Lysholm scores of >90 points allowed the correct diagnosis of symmetry in 71% and of >89 allowed the correct diagnosis of symmetry in 73% (test sensibility), respectively. For diagnosis of patients with a peak of torque deficit of >20% (test specificity), the questionnaire was accurate for 66% and 69% of patients at 60° s−1 and 180° s−1, respectively (Figure 1).
The Lysholm questionnaire was not validated to diagnose the peak torque deficit of knee flexion at any of the tested velocities, presenting an AUC of 0.5 (not significantly different).
Additionally, based on the cutoff values suggested by the ROC curve analysis, patients with a Lysholm score of ≤89 points presented a peak torque deficit of knee extension 36% higher than patients with a score of >89 points at a peak torque of 180° s−1 (p < 0.05) (Figure 2). In contrast, there was no difference at 60° s−1 for the cutoff value of 90 points (Figure 3).

Peak torque deficit of knee extension at 180° s−1 for a Lysholm score cutoff of 89 points. † p < 0.05 compared with ≤89 points.
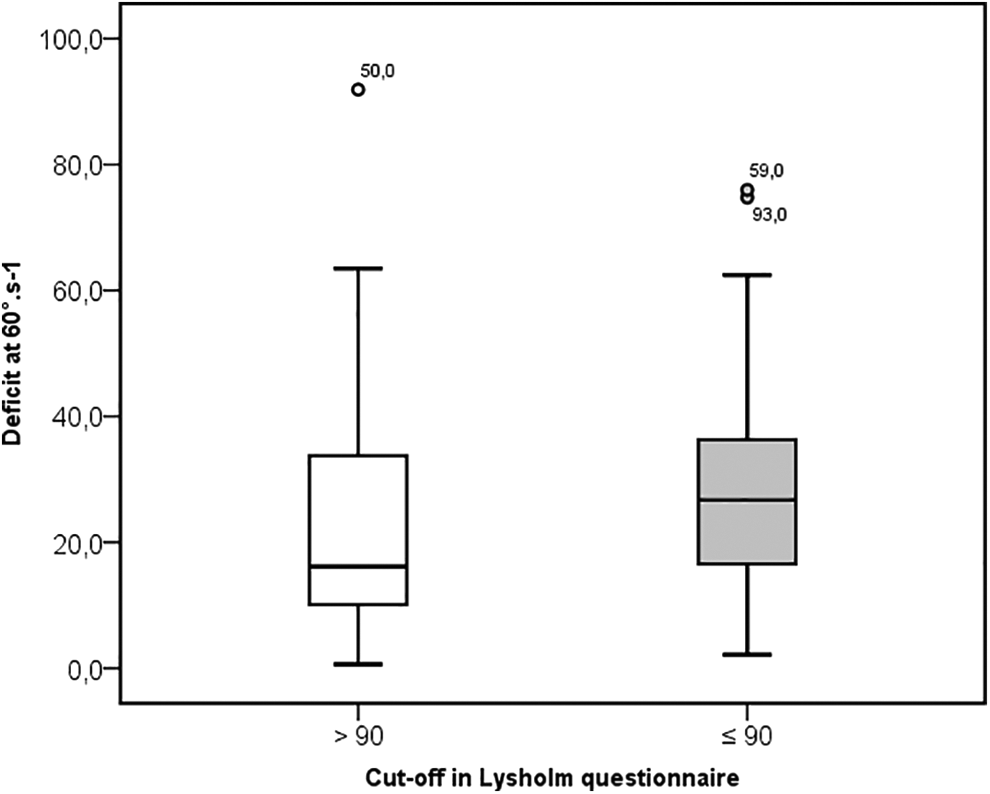
Peak torque deficit of knee extension at 60° s−1 for a Lysholm score cutoff of 90 points.
Discussion
This study demonstrated that a Lysholm score of >89 points has predictive value for a peak torque deficit in knee extension of <20%. Specifically, for the evaluation at 180° s−1, patients with a Lysholm score of ≤89 points presented a strength deficit 36% higher than those with a Lysholm score of >89 points. Thus, 8.8% of the variation in the peak torque deficit at 180° s−1 can be explained by the variation in the Lysholm score. Identification of the predictive measures of muscular deficits has relevant clinical implications, once higher deficits in the knee extensor peak torque are associated with the occurrence of lesions in the patellofemoral joint. 10
The difficulty of accessing isokinetic dynamometry devices in some fields has led researchers to develop alternative models for muscular evaluation that are objective and reproducible. 7 On the other hand, some investigators have found correlation between functional score and limb strength asymmetry. Zwolski et al. 3 used the International Knee Documentation Committee (IKDC) Questionnaire to predict quadriceps strength limb symmetry. Authors evaluated 139 young subject after released to RTP and found a predictable 90% symmetry quadriceps isometric strength when the IKDC score is over 94.8. 3
However, this study assessed isometric strength, while isokinetic strength better reproduces the daily needs and sports application of limb strength. An isokinetic dynamometer allows the evaluation of the muscular torque during the entire amplitude of muscular movement. 11 The presence of meniscal and chondral lesions tends to increase the strength deficit at higher angles of flexion and anterior cruciate ligament lesions the strength deficits are observed closer to the extension, at 30° of flexion. 12 Furthermore, Zwolski et al. 3 showed the prediction of asymmetry with IKDC in young athletes, while the present study showed prediction of asymmetry with Lysholm for a broad age and level of physical activity range.
One reason for the correlation between Lysholm score and peak of torch asymmetry could be the pain-induced limitation during isokinetic evaluation. Ueda et al. 13 showed that pain during the isokinetic evaluation was one of the factors associated with the differences in the strength of the quadriceps. 13 Pain-induced limitation is one of the aspects of the Lysholm evaluation and can also be related to other items in the questionnaire, such as limitations in ascending a ladder and crouching. In addition, ACLR patients who had undergone meniscectomy scored worse on IKDC evaluation, 14 Lysholm score and, comparing with the contralateral knee, meniscal tears cause proprioception deficit in higher knee angles of flexion. 15 Thus, meniscal, chondral, and other lesions could negatively influence functional score and isokinetic strength concomitantly.
Despite we found positive association between Lysholm score and extension peak torque deficit at 60° s−1, we observed no differences in this deficit between patients with a Lysholm score of <90 and >90. These results can be explained by the smaller patient sample evaluated at 60° s−1 and corroborate the findings of Wang et al. 10 who examined 87 patients and observed no differences in the Lysholm score between patients with a peak torque deficit of >20% and <20% at 60° s−1.
The present study showed no correlation of the Lysholm score with the difference in strength among the knee flexors. Although the action of the knee flexor musculature protects the anterior translation of the tibia, 16 it is generally not used as a criterion for rehabilitation progression or RTP. Post ACLR, the difference in flexion peak torque was lower than the difference observed in peak torque of extension, despite most of the reconstructions remove part of the hamstrings tendon to use as graft. These findings are consistent with those in the literature 10,16,17 and suggest that other factors affect strength more than the donor site morbidity.
The loss of strength can explain the high incidence of new lesions in patients with muscular deficits. Loss of muscular strength is associated with altered knee kinematic and kinetic during running. These biomechanical alterations during activity such as running could lead to knee lesions. 18 Despite all efforts to improve rehabilitation outcomes and muscular strength, the success rate in achieving the proposed RTP criteria remains unknown. 19 The quadriceps strength after ACLR can be improved with physical exercise; therefore, muscular asymmetry could be improved before RTP. 19 Strengthening of the thigh musculature after ACLR can be one strategy used to improve muscular symmetry. In a randomized study of preoperative muscle strengthening, Kim et al. 20 prevented quadriceps weakening and accelerated its strengthening after surgery, allowing the patient to quickly adapt to the rehabilitation environment. Furthermore, Ueda et al. 13 showed the higher quadriceps strength before ACLR is determinant to achieve sufficient quadriceps strength recovery at the timing of RTP.
One limitation of this study was the patient selection in different postoperative periods because the quadriceps strength improves over time. 21 However, the assessment of Lysholm scale was done in the same time period than isokinetic evaluation.
Another limitation of the present study is the lack of consensus to use the difference of 20% of peak torque asymmetry as the criterion to allow running or field activities. 6,22 Other protocols use different deficits for RTP. 10,23 Nevertheless, since a 20% peak torque deficit can be an effective progression criterion in rehabilitation or RTP after ACLR, this cutoff was applied in this study.
Conclusion
The Lysholm questionnaire is a useful prediction instrument for a peak torque deficit of knee extension of <20% and it might help clinicians to decide the better time to progress on the rehabilitation or RTP. However, its accuracy necessitates caution when it is used to replace the isokinetic evaluation in the diagnosis of muscular deficits.
Footnotes
Author contributions
Each author contributed individually and significantly to the development of the manuscript. ALLA designed the study and was responsible for data collection, data interpretation, drafted the first version of the manuscript and revised it critically for important intellectual content. AC performed statistical analysis, helped to draft the first version of the manuscript and revised it critically for important intellectual content. BL helped to design the study and data collection and revised the manuscript critically for important intellectual content. WDB designed the study and supervised the data collection, helped to draft the first version of the manuscript and revised it critically for important intellectual content. Finally, all authors approved the version of the manuscript to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.