
Abstract
Purpose:
The aim of this study was to perform a meta-analysis to compare the effects of repair of medial patellofemoral ligament (MPFL) and conservative treatment in patients with acute primary patellar dislocation (PPD).
Method:
The databases we used to search the studies included MEDILINE, EMBASE, and Cochrane registry of controlled clinical trials. Five randomized controlled studies comparing the effects of MPFL repair versus conservative treatment with 300 acute PPD patients were included in the present meta-analysis. Primary outcome was redislocation rate and secondary outcomes included Kujala score, percentage of excellent or good subjective opinion, Tegner activity score, and knee injury and osteoarthritis outcome score (KOOS; pain, symptoms, and activities of daily living).
Results:
The outcome of the Kujala score was statistically significant between the two treatments and indicated that MPFL repair had a higher Kujala score than conservative treatment in patients with acute PPD. There was no significant difference between the two treatments regarding the redislocation rate (p = 0.32), percentage of excellent or good subjective opinion (p = 0.15), Tegner activity score (p = 0.24), and KOOS (p > 0.05).
Conclusions:
Based on the available data, MPFL repair did not reduce the risk of redislocation nor did it produce any significantly better outcome based on the clinical manifestations, including anterior knee pain and knee activities. Only the Kujala score was improved by MPFL repair compared with conservative treatment.
Introduction
Patellofemoral problems are considered to be among the most common conditions in the practice of the general orthopedist and knee specialists. There are data showing that about 2–3% of knee injuries may be related to the primary patellar dislocation (PPD), with the highest incidence in adolescents and active young adults. 1 , 2 PPD refers to malalignment between the patellar tracking and the trochlear groove caused by trauma for the first time. In most cases, the injury site is seen in the medial peripatellar structures with the patella dislocated to the lateral side of the trochlear. Acute PPD always involves a series of symptoms, including severe knee pain, decreased function, frequent dislocation of the patella, and even patellofemoral osteoarthritis in the long term. 3
In the past, conservative treatment of primary patella dislocation was recommended in the absence of severe bone and cartilage damage. However, many studies showed high rates of redislocation (up to 44%) or instability of the patella after the first patellar dislocation at follow-up, which raised the question of the effectiveness of conservative treatment by many scholars. 4 , 5 With the progress of anatomy and etiology of the patella dislocation, the importance of medial patellofemoral ligament (MPFL) has been gradually recognized by many scholars. MPFL was attached between the middle-thirds of the patella and the femur and was considered to be the main soft tissue force that restricts the outward movement of patella, especially bending knees in the range of 0–30°, 6 and MPFL was tended to relax or rupture in more than 90% of previous cases of patellar dislocation or subluxation, mostly at the femoral insertion and traumatic dislocations were often responsible for tearing or loosing of the MPFL. 7 The surgery associated with the MPFL has become a popular technique for management of cases of recurrent patellar instability in the moment. 8 –10 However, for the primary traumatic patellar dislocation, whether MPFL repair is more effective than conservative treatment or not remains controversial. A randomized controlled trial (RCT) from Christiansen et al. compared the efficacy between conservative and surgical treatment of MPFL repair in 80 patients with acute PPD and concluded that the treatment of MPFL repair was not superior to conservative treatment in terms of the redislocation rate and improvement of subjective knee functional. 11 Palmu et al. also doubted routine repair of the torn MPFL is not advocated for the treatment of PPD in children and adolescents. 12 However, according to Askenberger’s research conclusions, it was found that surgically repairing the injured ligament did not achieve higher subjective knee function score but was more effective in reducing patellar redislocation rate than conservative treatment, 13 and other studies proposed that timely repair of MPFL can afforded better clinical outcomes. 14 , 15
To our knowledge, a few meta-analysis studies on this topic have been published. 9 , 16 , 17 However, multiple surgical approaches (e.g. capsule repair, MPFL repair, MPFL reconstruction, MPFL augmentation, and Roux-Goldthwait procedure) were taken together for analysis in those studies. This makes the results difficult to interpret and inevitably increases clinical bias. Few studies have compared the effects of one of the above surgical procedures versus the conservative methods for the treatment of acute PPD.
Hence, the aim of this study was to perform a meta-analysis comparing the effects of conservative versus isolated MPFL repair treatment for PPD with regard to redislocation rate, subjective function scores, and percentage of excellent or good subjective opinion to give clinicians a reference to decide the optimal intervention for patients with PPD.
Materials and methods
Search strategy
All published studies comparing the effects of conservative and MPFL-related surgical treatment for acute PPD were searched independently by two investigators using the databases including MEDILINE, EMBASE, and the Cochrane Registry of Clinical Trials. The publication date were not restricted when retrieving the database. The search terms performed in our study were listed as follows: (surgical OR medial patellofemoral OR operative OR medial patellofemoral OR MPFL) AND (nonsurgical OR nonsurgical OR nonoperative OR nonoperative OR conservative) AND (patellar instability OR patellar dislocation OR patell* dislocation OR luxating patella OR luxating patellar). A large number of searched studies were screened quickly depending on the title. For those studies that were not sure if they met the inclusion criteria, the abstract would be read for further screening. Finally, we would read the entire literature to determine the studies included. In addition, the references of each included study were reviewed to find ones that met the criteria.
Inclusion and exclusion criteria
The inclusion criteria for our study were as follows: (1) RCTs of levels I and II comparing the effect between conservative treatment and MPFL repair surgery for acute patellar dislocation; (2) the target population is male and female patients with skeletally immature or mature; (3) surgical or conservative treatment time initiated within 2 months after injury and ≥1 outcomes were reported including but not limited to the frequency of recurrent patellar dislocation, subjective function scores, and patients satisfaction; and (4) the average follow-up time was 2 years or more. Only published data on peer-reviewed journals were considered. The exclusion criteria are as follows: (1) nonprimary patella dislocation; (2) patients with previous history of patella instability and knee trauma or surgery; (3) patients with femoral–tibial ligament or meniscus injuries; and (4) retrospective studies, case reports, basic science studies, insufficient data, and biomechanical studies
No restrictions on the type of MPFL injury and strategies of conservative treatment were made. Both open and arthroscopic MPFL repair were included in the present study. Lateral retinaculum release and smaller osteochondral fragments remove are performed, if necessary. Conservative treatment strategies for acute PPD included bracing with knee brace or splinting, advice and guidance from surgeon, mild exercise with the help of crutch, exercise basing rehabilitation, and the technique of electromagnetics.
Data management
Once the included study is confirmed, two authors would review the full text of the study and extract the data we need, including study design, sample size, mean age, gender (F/M), the time after injury, and follow-up time. After the data extraction step is completed, all the data are organized in the information table (Table 1). At the same time, the outcomes of the included studies were also extracted including but not limited to redislocation rate, Kujala score, Tegner activity score, percentage of excellent or good subjective opinion, and knee injury and osteoarthritis outcome score (KOOS; pain, symptoms, and activities of daily living (ADLs)). To solve the disagreements or inconsistencies of the data extracted, there would be a third author involved in the discussion and resolution. When the data are incomplete, corresponding authors were contacted. Where possible, all the date extracted from the studies included were pooled and a meta-analysis was performed. In our study, the redislocation rate was the primary outcome variable and the knee subjective function scores mentioned above and subjective opinion percentage according to the Kujala score were the secondary outcome. Although some outcome variables, such as patellar tilt, tibial tubercle trochlear groove (TT-TG) distance, and Caton-Deschamps index, were performed by individual studies, they were not included in the present study because they cannot be pooled and compared significantly.
Modified Jadad quality scale for each included study.

Methodological assessment
The quality appraisal of the methodology of the included studies was performed by two authors using Modified Jadad quality scale (Table 1). The scale contains six assessment items, each of which is answered by “yes” or “no” (“yes” means 1 or 2 points and “no” means 0 point). The higher the score, the higher the methodological quality of the included study.
Statistical analysis
I 2 statistics were used to evaluate the heterogeneity of statistics in multiple studies. When I 2 statistics is no more than 50% (I 2 ≤ 50%), statistical heterogeneity could be accepted, and the fixed-effect model was adopted to calculate the pooled statistics. If heterogeneity existed in multiple homogeneous outcomes (I 2 > 50%), the random-effects model was used. Dichotomous data and continuous variables were presented as risk ratio (RR) and mean difference (MD), respectively, with 95% confidence intervals (CIs). Meta-analysis was performed by using RevMan 5.3 software from the Cochrane collaboratione. A p value of p ≤ 0.05 was considered statistically significant.
Results
According to our inclusion criterias and exclusion criterias, 5 eligible studies with a total of 300 patients were included after the completion of the literature search (Figure 1). The main characteristics extracted from the included studies were integrated into Table 2. All included studies were limited to comparing the effects of MPFL repair versus the conservative methods for the treatment of acute patella dislocation. There were different in conservative treatment strategies, such as duration and methods of immobilization, advice and guidance from surgeon, and rehabilitation programs.
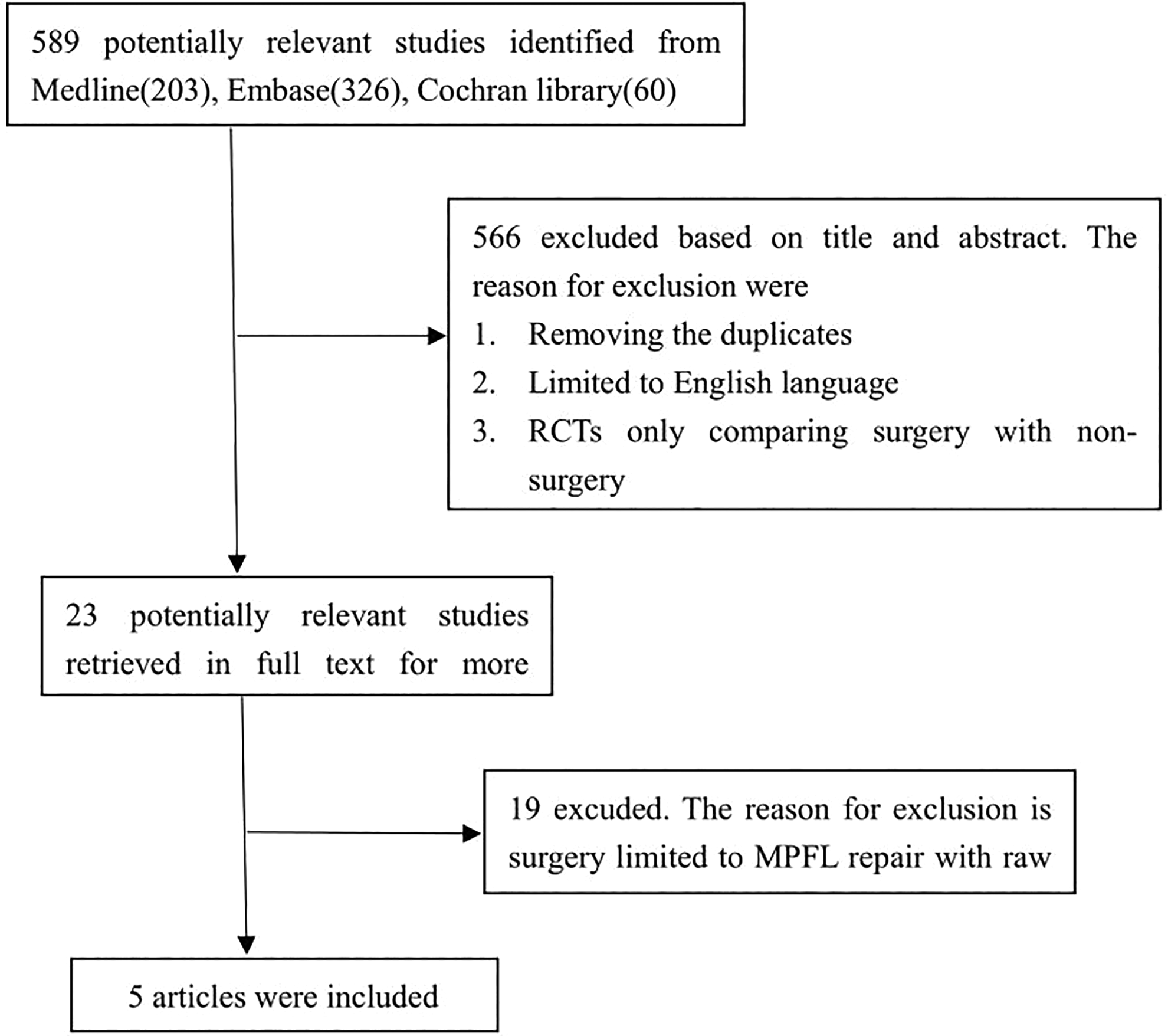
Flow chart of eligibility selection.
Main characteristics of included studies.

RCT: randomized controlled trial.
Frequency of recurrent patellar dislocation
All included studies with patients of 158 MPFL repair and 142 conservative treatment provided the data on frequency of recurrent patellar dislocation. A meta-analysis showed that no significant difference in the MPFL repair and conservative treatment regarding recurrent patellar dislocation (RR = 1.06; 95% CI: 0.55–2.06; p = 0.86, I 2 = 59%; Figure 2(a)). So, sensitivity analysis with one study 15 excluded was performed due to moderate heterogeneity. The results of the sensitivity analysis revealed that the frequency of recurrent patellar dislocation was also not significantly different in the two treatments (RR = 0.85; 95% CI: 0.63–1.16; p = 0.32, I 2 = 19%; Figure 2(b)), and the fixed-effect model was used to calculate the pooled statistics.

Forest plot. Outcome: redislocation rate. (a)
Subjective assessment of symptoms and functional outcomes
Five included studies with 300 patients provided data concerning the Kujala score. The pooled data demonstrated that the Kujala score was significantly higher in patients with MPFL repair than that in patients with conservative treatment. However, the heterogeneity of statistics was higher in these studies (MD = −9.73; 95% CI: −15.90 to −3.57, p < 0.002, I 2 = 85%; Figure 3(a)), in favor of MPFL repair for the treatment of acute PPD. After a retrospective sensitivity analysis, two studies 11 , 14 were excluded and heterogeneity was significantly reduced, and the results of meta-analysis still supported the MPFL repair for acute PPD using the fixed-effects model (MD = −4.43; 95% CI: −8.11 to −0.74, p = 0.02, I 2 = 0%; Figure 3(b)).

Forest plot. Outcome: Kujala score. (a)
The percentage of excellent or good subjective opinion was assessed in two studies included according to the Kujala score, and Kujala score >84 and ≤84 were defined as excellent/good and fair/poor, respectively. No significant difference was demonstrated by the pooled data between the two treatments (95% CI: 0.03–1.74, p = 0.15, I 2 = 77%; Figure 4), with high heterogeneity.

Forest plot of percentage of excellent or good subjective opinion between conservative and MPFL repair for acute PPD. MPFL: medial patellofemoral ligament; PPD: primary patellar dislocation.
Data on VAS were available in two studies, including 71 patients with MPFL repair and 56 patients with no surgery. The summary MD was −0.89 (95% CI: −2.35 to −0.58; p = 0.24, I 2 = 79%; Figure 5), indicating that no significant support for any group of treatments for acute PPD.

Forest plot assessing Tegner score between two treatment strategies for acute PPD. PPD: primary patellar dislocation.
For KOOS including pain, symptoms, and ADLs, there was no significant difference between the two treatment groups. (Figure 6(a) to (c))
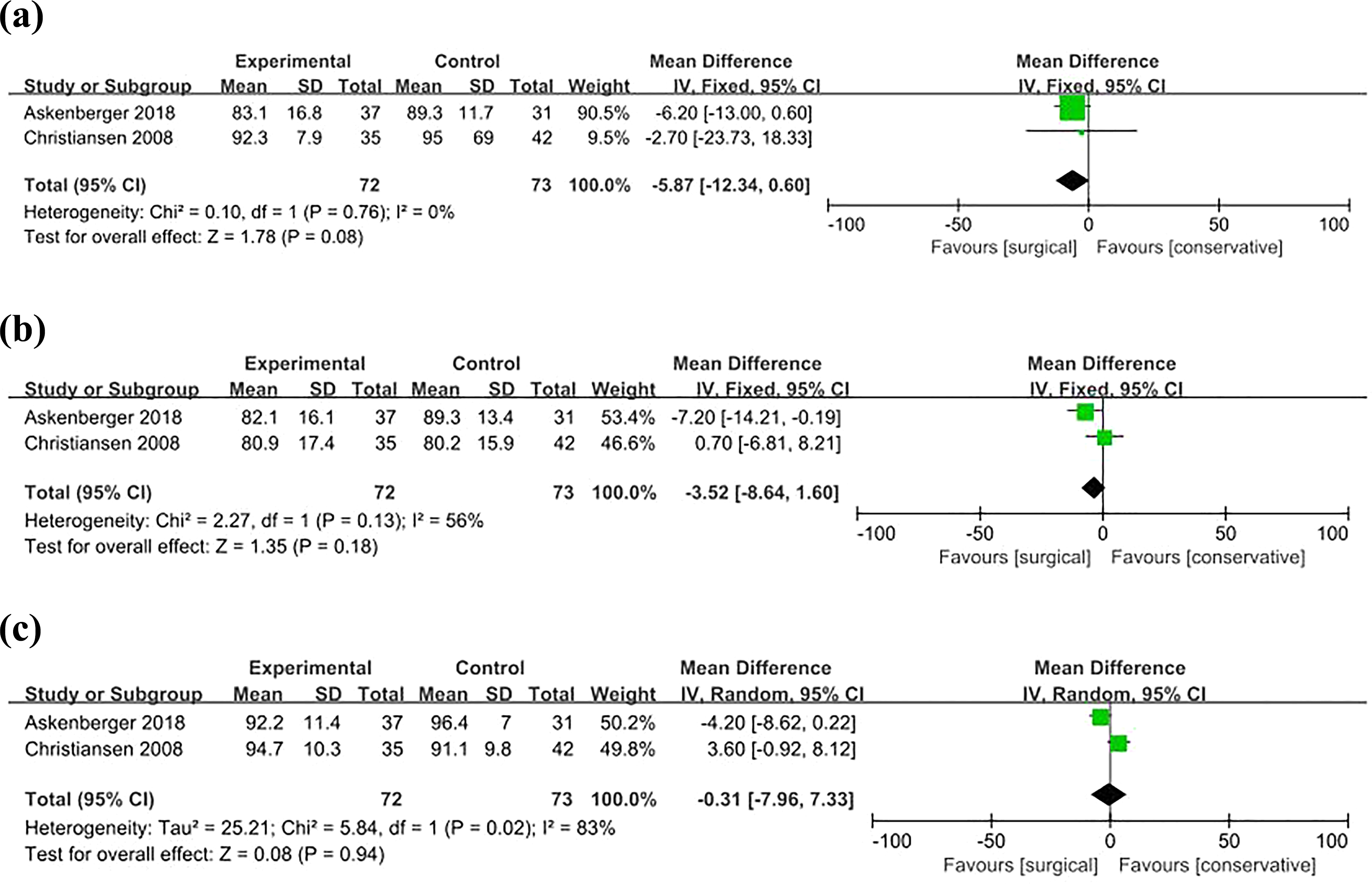
Forest plot assessing KOOS between two treatment strategies for acute PPD. (a): pain; (b): symptom; and (c): ADL. PPD: primary patellar dislocation. KOOS: knee injury and osteoarthritis outcome score; ADL: activity of daily living.
Discussion
The main purpose of this retrospective meta-analysis was to find the advantages and disadvantages of conservative strategies and MPFL repair for the treatment of acute PPD to provide a reference for clinicians. When all the data of the studies were pooled and analyzed, it was found that the patients with MPFL repair had a higher Kujala score than conservative treatment. However, there is no significant difference in redislocation rates, Tegner activity score, KOOS, and percentage of excellent or good subjective opinion between the two treatments. Conclusions of the present study were inconsistent with the previously published meta-analysis, 9 , 16 which concluded that surgical treatment has a lower redislocation rate compared with conservative treatment and showed that there were significant differences in subjective functional scores (some supporting surgery and some supporting conservative treatment) between the two treatments. The most likely reason caused the difference was that a variety of different surgical interventions were involved in previous meta-analysis (e.g. capsule repair, MPFL repair, MPFL reconstruction, MPFL augmentation, and Roux-Goldthwait procedure). It is difficult to compare the effects of multiple surgical methods and conservative treatments in one study. This is likely to reduce the credibility of the results and make the conclusions difficult to interpret.
Patellar dislocation is a common disease of the patellofemoral joint. In recent years, substantial progress has been made in the studied of the etiology and treatment of patella dislocation, such as formation of the trochlear for the treatment of femoral trochlear dysplasia, tibial tubercle transfer for the treatment of increased Q angle, MPFL reconstruction for injured ligament and femoral derotation osteotomy for the treatment of the excessive femoral internal rotation, and so on. A study pointed out that MPFL was attached between the middle-thirds of the patella and the femur and was considered as the main force limiting the lateral dislocation of the patella, which accounts for about 53% of the total strength. 18 Many scholars reported that MPFL reconstruction can achieve good results in the treatment of acute patella dislocation and were keen on MPFL reconstruction for acute patella dislocation. 19 , 20 However, in children with open epiphysis, MPFL reconstruction for the treatment of patella dislocation may increase the risk of epiphysis injury. Therefore, few scholars recommend MPFL reconstruction in children. MPFL repair may be a suitable treatment for acute dislocation of the patella during the period of child. However, there was still controversy about the advantages and disadvantages of MPFL and conservative treatment of acute patella dislocation. 12 , 13 The purpose of our study is to retrospectively analyze and compare the advantages and disadvantages of the two treatments.
In the present meta-analysis, only the Kujala score showed a significant difference between the two treatments in support of MPFL repair for the treatment of acute PPD, and there was no statistical difference in dislocation rate or other subjective functional scores. Initially, when the data were pooled to analyze, the outcomes showed a high heterogeneity in those studies included. Later, we reviewed the literature retrospectively and found that a study published by Camanho et al. 15 differed from other studies as follows: a smaller sample size, a shorter knee fixation time of only 3 weeks in the conservative treatment group before rehabilitation exercise and MRI was not performed in the conservative group of patients. Any of these differences may increase the heterogeneity. After a sensitivity analysis with this study excluded was performed, heterogeneity could be accepted and no change was made in the systematic evaluation of the redislocation rate. A previous study 21 reported that the MPFL injury site may affect the clinical outcome of treatment of patellar dislocation. The target populations of the study published by Ji et al. 14 were limited to patients who were treated for acute PPD with a nonoverlap region injury (no overlap area with vastus medialis oblique (VMO)). Heterogeneity reached an ideal level after sensitivity analysis with two studies excluded. 14 , 15 There was still no difference in the Kujala score between two analyses which meant the reliability of our results.
According to the result of our study after pooling and analyzing the data in this meta-analysis, the Kujala score was higher in the MPFL repair group. Consistently, previous studies also found a higher Kujala score and a better subscore regarding patella stability within the Kujala score in the MPFL repair group, which indicates that surgical repair of MPFL can better improve the subjective sensation of patients with patellar dislocation. 11 , 15 To our knowledge, previous meta-analysis reported no significant difference in the Kujala score between the surgical and conservative groups. 9 , 17 However, the surgical procedures in their study involved a variety of medial retinaculum procedures but did not emphasize the repair of MPFL. Therefore, the difference in surgical procedures makes it impossible to compare the previous studies with our study.
The strengths of the present study were that high-quality literature containing the latest studies were included 13 , 14 and MPFL repair was limited as a major surgical procedure for the treatment of acute PPD. In Palmu’s study, 12 some of the patients underwent MPFL repair combined with lateral retinaculum release. Several anatomical studies have shown lateral release results in a reduction in the force required to dislocate the patella laterally as it becomes easier for the patella to ride up and over the lateral side of the trochlea. 22 –24 When an lateral retinaculum release was performed after MPFL repair, the effect was to decrease the ability of the patella to resist laterally directed force by 7–11%, 23 which may affect our final findings. In view of that, we then excluded this study for another analysis after the sensitivity analysis and found that the outcomes of redislocation rate (p = 0.43) and Kujala score (p = 0.01) did not change essentially, meaning the stability of our results.
Certainly, our study still had the following shortcomings: First, although the surgery was limited to MPFL repair, the MPFL injury area was not consistent. Some studies 9 , 21 reported that understanding the relationship between MPFL injury and the VMO may improve the therapeutic effect of patella dislocation and suggested that the MPFL lesions should be divided into three types according to whether the MPFL overlaps with the VMO: the VMO overlap zone, the VMO nonoverlapping zone, and the combined injury. They concluded that conservative treatment achieved a higher function score and a lower redislocation rate for the VMO overlap zone injury than VMO nonoverlapping zone injury of MPFL and surgical treatment of MPFL lesions in VMO nonoverlapping areas was recommended. Second, there were diversifications in conservative treatment strategies. To date, no one optimal conservative treatment strategy was suggested and different conservative treatments were performed in each study or individual. It is difficult to compare the therapeutic effect of a surgical procedure with a variety of conservative treatments for the treatment of acute PPD. Third, there were differences in age and sex ratio or unequal risk factor for dislocation of the patella in the study population we included. Fithian et al. 25 reported that girls had a higher risk of PPD and redislocation rate than boys and young patients had a lower risk of PPD than the older ones. The subgroup analysis is not carried out because of the limited number of studies included. We recommend that higher quality RCTs should be carried out to overcome many of the deficiencies in our research.
Conclusions
The available evidence indicated that MPFL repair could produce significantly better functional outcome based on the Kujala score after acute primary patella dislocation. However, there was not enough evidence to show that MPFL repair was more likely to lower the redislocation rate compared to conservative treatment in our study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.