
Abstract
Purpose:
This study reports the results of a multimodal thromboprophylaxis protocol for lower limb arthroplasty involving risk stratification, intraoperative calf compression, aspirin prophylaxis and early (within 4 h) post-operative mobilisation facilitated by the use of local infiltration analgesia. The study also aimed to identify risk factors for venous thromboembolism (VTE) within a 3-month period following surgery for patients deemed not at elevated risk.
Methods:
Patients undergoing knee/hip arthroplasty or hip resurfacing were preoperatively screened for VTE risk factors, and those at standard risk were placed on a thromboprophylaxis protocol consisting of intraoperative intermittent calf compression during surgery, 300 mg/day aspirin for 6 weeks from surgery and early mobilisation. Patients were screened bilaterally for deep vein thrombosis (DVT) on post-operative days 10–14. If proximal DVT was detected, patients were anticoagulated and outcomes were recorded. Symptomatic VTE within 3 months of surgery were recorded separately. Patient notes were retrospectively collated and cross-validated against ultrasound reports.
Results:
At initial screening, the rate of proximal DVT was 0.54% (1.1% for knee and 0.27% for hip), and distal DVT was 6.63% (20.11% for knee and 2.31% for hip). One small, nonfatal pulmonary embolism (PE) was detected within 3 months of surgery (0.28% of total knee arthroplasty patients or 0.07% of total). All proximal DVTs were treated successfully with anticoagulants; however, one patient suffered a minor PE approximately 10 months post-operatively. Regression analysis identified knee implant and advanced age as independent risk factors for VTE in this cohort.
Conclusion:
Although knee arthroplasty patients remained at higher risk than hip replacement/resurfacing patients, the incidence and outcomes of VTE remained positive compared with protocols involving extended immobilisation, and episodes of PE were extremely rare. Thus, we conclude that patients at standard preoperative risk of VTE may safely be taken through the post-operative recovery process with a combination of intraoperative mechanical prophylaxis, early mobilisation and post-operative aspirin, with closer attention required for older patients and those undergoing knee surgery.
Introduction
Hip and knee arthroplasty is complicated by the risk of venous thromboembolism (VTE), including deep vein thrombosis (DVT) which in many cases is silent and resolves spontaneously, 1 and pulmonary embolism (PE), which is currently the second most common cause of death following hip or knee arthroplasty. 2 Without thromboprophylaxis, the incidence of DVT is extremely high at an estimation of around 37%. 3 Chemical and mechanical strategies for preventing DVT and PE following arthroplasty are consistently recommended in major orthopaedic thromboprophylaxis guidelines. 3 –5 However, these guidelines do not make strong recommendations for specific prophylactic regimes.
A recent meta-analysis reported that lower risk patients given multi-modal thromboprophylaxis involving risk stratification, aspirin and mechanical compression were at similar risk of fatal pulmonary emboli compared with standard patients on multimodal prophylaxis involving warfarin. 2 The incidence rates reported (approximately a quarter of the overall 0.2% mortality rate reported for the two protocols) were also substantially lower than those reported previously, which ranged from 0.19% to 0.4%. 6 –8 Combined risk stratification, aspirin and mechanical compression has also been suggested to be equivalent to anticoagulants at preventing symptomatic VTE, thought to be the most reliable clinical indicator of risk for PE. 9,10 Thus, it appears that for patients who are not at elevated baseline risk of thromboembolic events, aspirin, early mobilisation and/or mechanical prophylaxis may be equally effective as anticoagulant therapy 11,12 with lower all-cause mortality, 13 fewer major bleeding episodes, fewer wound healing complications and fewer associated costs. 14
Here, we report the results of a multimodal thromboprophylactic regime in a large cohort of hip and knee arthroplasty patients without additional risk factors for VTE. Overall, the aims of this study were to (i) determine the incidence of distal and proximal DVT (regardless of symptomatic status) following lower limb arthroplasty in patients at standard VTE risk subjected to a multimodal thromboprophylaxis protocol; (ii) identify risk factors for DVT in this selected patient group; and (iii) determine the outcome of clinically significant VTE events within 3 months of surgery.
Methods
Study design
A prospective observational cohort study with selective sampling was utilised. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 15 were retrospectively implemented to the analysis and reporting.
Patient selection and recruitment
All patients electing to undergo total hip/knee replacement or hip resurfacing between 2004 and 2014 by a single surgeon were consented into a clinical registry to retain clinical information for research purposes. Ethical approval for retrospective data analysis and publication was provided by an accredited Human Research Ethics Committee (Bellberry Ltd; 2017-03-237). Patients were screened for participation in the thromboprophylaxis protocol during the preoperative anaesthetic consultation. Patients were excluded from the protocol and prescribed anticoagulants if they met one or more of the following criteria: unable or unwilling to comply with the early mobilisation component of the protocol; presenting with a past history of VTE or a family history of thrombophilia (deemed at high risk of thromboembolic complications); undergoing simultaneous bilateral procedures; and undergoing a revision arthroplasty procedure.
Patients taking anticoagulants regularly prior to the operation were also excluded from data analysis due to potential residual effects of the medication.
Surgical and perioperative management
All hip resurfacing procedures were performed via a posterior approach as previously described. 16 Total hip arthroplasty (THA) procedures from 2004 to 2007 were performed using a posterior approach 17 and those from 2008 onwards with a direct anterior approach Anterior Minimally Invasive Surgery (AMIS). 18 Limited crossover occurred in 2007 during the transition from posterior to anterior approaches for THA. THAs were performed using a hybrid system consisting of Birmingham resurfacing acetabular components, Birmingham modular heads and various cemented and uncemented stems. Total knee arthroplasty (TKA) procedures were performed with a subvastus or medial parapatellar approach 19 and manual instrumentation, tibia-first with an extramedullary guide rod followed by the femur with an intramedullary guide. Implants used were Smith & Nephew Genesis II (Smith & Nephew, Memphis, Tennessee, USA) or Medacta GSK spheres (Medacta International AG, Castel San Pietro, Switzerland). For the majority of operations, a tourniquet was not used.
A combination of opiate-free spinal anaesthetic and general anaesthetic without volatile gases was utilised for all procedures. A local infiltration analgesic technique was also performed 20 on a procedure-specific basis. Pneumatic calf compression was also used during the intraoperative period. At the conclusion of the procedure, the wound was catheterised with an in-line bacterial filter included, which was used to top-up the analgesia mixture as required overnight until reinjection and catheter removal the following morning prior to discharge.
DVT prophylaxis protocol
Patients received aspirin (300 mg per day), starting on the day of surgery and continuing for 6 weeks, and bilateral below-knee graduated compression stockings. Mobilisation was initiated approximately 3–4 h following surgery. Patients were administered a fluid bolus of 2–300 mL and were immediately encouraged to stand by the senior physiotherapist or a trained member of the medical team. In cases of postural hypotension, additional intravenous fluids or, rarely, a single dose of atropine were administered. If patients could stand with assistance, they were encouraged to walk a minimum of approximately 30 m with the assistance of a walking frame. This process was repeated every 2–3 h until patients were able to transition to independent walking on elbow crutches, at which point they were encouraged to take charge of their own mobilisation for the remaining hospital stay. Patients were also encouraged to sit out of bed as often as possible and were allowed to use the toilet with assistance as required. Patients were typically discharged the following day if they satisfied the following requirements: restoration of normal haemoglobin and electrolyte values, no uncontrolled comorbidities, independent toileting, walking, transition from seated to a standing position and navigation of one flight of stairs with minimal assistance. Additional requirements for discharge were access to a suitable home environment without stairs and the availability of someone at home to assist with transport and daily activities in the early post-operative period.
DVT screening, treatment and follow-up
All patients attended a follow-up appointment between 10 days and 14 days following surgery for skin clip or suture removal. At this appointment, routine bilateral ultrasound Doppler sonography (‘duplex’) was performed, and the presence or absence of DVT was recorded. One sonographer performed all duplex scans for this study. Positive duplex scans were labelled as ‘significant’ using the following criteria: 10 cm or greater in length
AND
located in or extending into axial veins (i.e. Popliteal, Femoral, Iliac)
OR
located above the knee-crease.
Patients with DVTs deemed significant were placed on anticoagulants for a minimum of 4 weeks, with INR (International Normalised Ratio) maintained between 2.0 and 3.0 when required. Anticoagulants were discontinued once follow-up Doppler imaging confirmed that the thrombus had stabilised or disappeared. Non-significant DVTs (as per the above-mentioned criteria) were not treated, and all patients were advised to report any symptoms such as leg pain, swelling and shortness of breath to the surgeon or general practitioner immediately if they arose. Details of any subsequent investigation and treatment of VTE were recorded in follow-up notes and the database of the treating anaesthetist.
Data and statistical analysis
Incidence of VTE during initial screening and 3-month follow-up
Patients unable to follow the post-operative mobilisation protocol or treated with anticoagulants for a below-knee DVT (at the request of the patient or their general practitioner) were classified as protocol violations and excluded from the analysis (Figure 1). Pertinent findings in ultrasonography reports were recorded in patient notes at the time of follow-up and retrospectively collated for analysis into an Excel spreadsheet. These were cross-validated against hard copies of ultrasound reports prior to analysis. DVT incidence was calculated by dividing the number of positive duplex scans by the sample included for analysis. Incidence of symptomatic DVT or PE within 3 months of surgery was also extracted from these notes.

Flow diagram of patient inclusion, follow-up and analysis of VTE after lower limb arthroplasty. VTE: venous thromboembolism.
Identification of risk factors for VTE
Sample size calculations were based upon a rule of thumb of 10 DVT events per variable entered into a binary logistic regression model. 21 Assuming a DVT incidence of 7% based on preliminary analysis of the clinical registry, 1760 patients would have 80% power to detect a significant effect of up to 6 predictive variables, allowing for up to 10% cohort protocol non-compliance and a two-sided α of 0.05. A logistic regression model with patient, surgical and management factors included as predictors was performed on the binary outcome of VTE presence using a logit link function. The variables included for analysis were patient age, gender, surgical side, procedure type, joint (hip or knee), year of surgery and presence of VTE (yes or no). Univariate comparisons (t-test and χ 2 analysis) were also made between hip and knee groups for individual demographics. All statistical analyses were performed in Minitab (v18, Minitab Inc., State College, Pennsylvania, USA), with α set at 0.05.
Results
Patient exclusion, demographics and descriptive
In the patient cohort, 19% (n = 357) of patients were excluded due to ultrasound reports being unavailable at the time of review, and 1.6% (n = 30) of patients reported protocol violations, such as missed medications, inability or unwillingness to follow post-operative mobilisation instructions, or prophylactic anticoagulation at the patient’s request or by another healthcare provider. This left 1491 arthroplasty procedures in the analysis (Table 1). Patients presented at a mean age of 62.5 years (
Summary of demographic data for analysed cohort.a
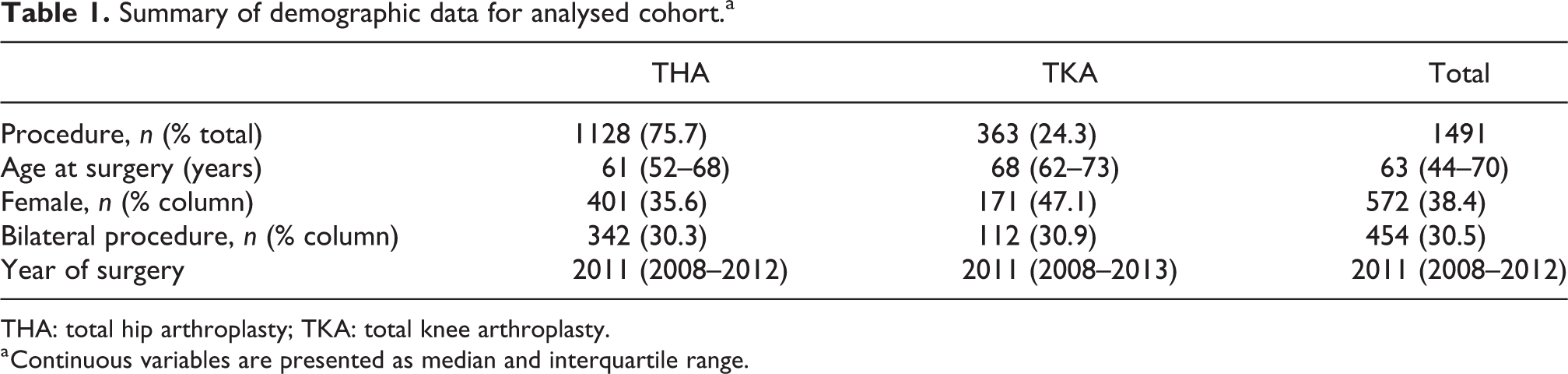
THA: total hip arthroplasty; TKA: total knee arthroplasty.
a Continuous variables are presented as median and interquartile range.
Incidence of DVT during screening
DVTs were detected in 108 patients during screening, representing 7.24% of the study sample. Of these, 99 DVTs (6.6%) were distal and therefore of limited clinical significance (Table 2). Proximal DVTs were detected in 9 patients or 0.6% of the total cohort. No pulmonary emboli were reported in the 2 weeks between surgery and screening. Age at surgery was associated with the presence of a DVT of any kind (odds ratio (OR): 3.5% per year of age, 95% confidence interval (CI): 1–6% per year of age; p = 0.006), and undergoing a knee arthroplasty was also an independent risk factor (OR: 7.8, 95% CI: 4.9–12.3; p < 0.001), with an incidence of 21.5% knee cases versus 2.7% hip cases (Figure 2).
Proportion of patients with VTE at 3 months stratified according to demographics and operative variables included in logistic regression.

VTE: venous thromboembolism; DVT: deep vein thrombosis; PE: pulmonary embolism; IQR: interquartile range.

Summary of age at surgery by arthroplasty procedure (hip, knee) and presence of DVT (mean and 95% confidence intervals). DVT: deep vein thrombosis.
Outcomes of clinically significant VTE
Patients with proximal DVT were treated with anticoagulants for 1–6 months following diagnosis, with no occlusive thrombi detected by 6 months post-surgery. No pulmonary emboli were reported within the follow-up period for patients receiving hip surgery. One non-fatal pulmonary embolus was detected in a TKA patient treated with warfarin for a small DVT. Despite warfarin prophylaxis and full weight bearing post-operatively, the patient presented with marked leg oedema 6 weeks post-operatively. Testing revealed oxygen desaturation and minor pulmonary defects on ventilation–perfusion scans. Another TKA patient suffered a PE approximately 10 months following detection of a significant DVT extending 2 cm above the knee crease during screening. This patient was treated with warfarin for 4 weeks following discovery of the thrombus, which was deemed to have resolved following treatment. A history of autoimmune disease and previous ipsilateral knee surgery (a tibial osteotomy) were noted for this patient. Both patients with PE were successfully treated and had recovered fully by the next surgeon follow-up.
Discussion
The aim of this study was to establish the results of a multimodal thromboprophylactic protocol, involving optimised analgesia enabling early mobilisation, antiplatelet therapy and routine ultrasonographic screening for DVT, in a large series of lower limb arthroplasty patients at standard VTE risk. The local infiltration analgesic technique has been adopted by a number of centres to facilitate the early mobilisation component of VTE prophylaxis and has enabled patients to mobilise earlier and with less pain than other methods. 22 –24 Using ultrasound screening, we observed a DVT incidence rate of 7.24% at post-operative days 10–14. Of these, the majority were distal DVTs. One patient anticoagulated for a small proximal DVT experienced a PE within 3 months of surgery, leading to an overall 3-month PE incidence of 0.07% in this study cohort.
Upon screening at days 10–14, distal and proximal DVTs were detected in 99 (6.6%) and 9 patients (0.6%), respectively, with no PE observed during this time. Although studies vary in their approach to capturing DVT rates, we identified a number of large studies using screening at similar durations. 25 –28 One such study 27 reported screening a large number of patients with venography; however, patients were ambulated slightly later, between 24 h and 48 h post-operatively. The DVT incidence approximately 1 week after THA was 10.3%, substantially more than our overall DVT rate approximately 10 days after hip replacement or resurfacing, which was 2.7%. Although Doppler ultrasonography is less sensitive than venography for identifying DVT, estimates of sensitivity are around 96.5% for proximal and 71.2% for distal DVT. 29 Taking this into account, the true rate of DVTs in this study is likely to be closer to 3.8%. Thus, our findings, particularly the low rate of proximal DVT, are unlikely to be entirely due to differences in sensitivity.
We have identified age as an independent risk factor for DVT, which is consistent with results of a recent meta-analysis of risk factors for VTE. 30 Knee surgery was also an independent risk factor for DVT even when the small age discrepancy between knee and hip arthroplasty groups was taken into account, with a far greater DVT incidence in knee versus hip patients, and no PEs reported in hip patients. This is consistent with a systematic review of randomised controlled trials assessing screening studies involving 2912 TKA and 1455 THA patients, which reported an OR of 1.85 for TKA compared with THA. 31 The source of this increased risk has not been definitively established, with controversy over the impact of tourniquet 32 or intramedullary guide use. 33 It is also not clear whether this risk is modifiable or intrinsic to the location or specifics of the procedure. It is possible that TKA patients suffer from greater venous outflow obstruction due to swelling and inflammation caused by trauma associated with prolonged forcible eversion of the extensor apparatus and forcible anterior dislocation of the tibia required to implant the TKA components. 34 Nonetheless, in spite of the increased incidence of DVT in knee arthroplasty patients observed here and elsewhere, the rates of clinically significant VTE are equivalent to those typically reported for the hip arthroplasty population. 6 Further investigations are required to determine whether negative sequelae such as post-phlebitic syndrome is also more common in patients undergoing knee arthroplasty.
No patients treated for proximal DVT had occlusive thrombi by 6 months post-operatively. However, one patient (0.07%) was diagnosed with a symptomatic pulmonary embolus within 3 months post-operatively following resolution of a DVT. Another patient experienced a PE at approximately 10 months following discovery, and subsequent treatment, of a proximal DVT. Due to the extensive time delay, it is the opinion of the authors that this PE is unlikely to be directly related to the surgery. The overall 3-month PE rates observed in this study compare favourably with a recent large study of patients undergoing early mobilisation and short-duration anticoagulant thromboprophylaxis for TKA and THA, which reported a 90-day symptomatic PE incidence of 0.11%. 35 In addition, a recent systematic review of in-hospital symptomatic VTE incidence using conventional anticoagulants reported a symptomatic PE incidence of 0.27% after TKA or partial knee arthroplasty, and 0.14% after hip arthroplasty at a mean follow-up of 13 days, ranging from 8 days to 35 days. 36 The present study reveals zero PE incidence within the same time frame for patients following the described protocol. This suggests the multimodal protocol was effective at eliminating the short-term risk of potentially fatal VTE without the need for anticoagulant use, provided patients were not at elevated thromboembolic risk prior to surgery. While many similar multimodal protocols have been reported elsewhere (a summary of these is presented in Online Supplementary table 1), the wide heterogeneity in outcome criteria (i.e. symptomatic vs. asymptomatic VTE) and surgical techniques preclude a direct comparison. Therefore, it is challenging to determine which elements of our protocol were of most clinical benefit. As the costs and risks associated with our protocol are very low, we are confident that all elements of the protocol can be clinically justified and appropriately resourced at other sites.
The strengths of this study include direct observation of a large series of patients through Doppler screening, and consistent implementation of the mobilisation protocol enabled through the use of an optimised analgesic regimen. However, as the study relied on retrospective evaluation of patient records spanning a large period of time, a number of ultrasound screening reports were not accessible for analysis. While there is a possibility this may have introduced bias into the analysis, it was possible to cross-validate the majority of major events from the anaesthetist’s database. Thus, if bias due to availability of data were introduced, the incidence rate of symptomatic VTE is likely to have been overestimated in this cohort. We note that the ability to draw firm conclusions on the efficacy and safety of a given protocol based on a single cohort without a comparison group is limited; however, our incidence rates are in line with those reported previously for similar protocols, 10,22,26,37 and an appropriately powered randomised clinical trial would require many thousands of patients to perform. 22 Given the incidence of PE is extremely low in the arthroplasty patient population irrespective of intervention, 6,22,35 demonstrating the superiority of one prophylaxis regime over another at preventing this rare but potentially devastating outcome is challenging. Nonetheless, the accumulating evidence indicates the approach used here is well justified. Lastly, while we did not assess other complications such as bleeding and infection for this particular study, we have previously reported encouraging results in hip resurfacing patients, 38 and other studies have addressed this question in their own patient groups. 12,39
VTE is a relatively infrequent cause of rehospitalisation and mortality after joint arthroplasty, with bleeding and infection more common. 2,13,40 The positive results of our multimodal thromboprophylaxis protocol indicate that a careful approach to risk stratification combined with intensive early post-operative mobilisation and close monitoring of thromboembolic complications is an effective and safe approach to thromboprophylaxis. Further consideration should be taken for patients undergoing TKA due to their inherently higher risk of VTE; however, the results of this study suggest that with appropriate mobilisation the risk of PE is extremely low regardless. Therefore, we recommend a conservative approach to chemical thromboprophylaxis, with the use of stratified risk assessments and measures to ensure compliance with multimodal protocols, reserving the use of anticoagulants for patients with known excess risk, or for those who cannot comply with standard protocol.
Overall, the aims of this study were to determine the incidence of distal and proximal DVT (regardless of symptomatic status) following lower limb arthroplasty in patients at standard VTE risk subjected to our multimodal protocol, to identify risk factors for DVT in this selected patient group and to determine the outcome of clinically significant VTE events within 3 months of surgery. We found the incidence of DVT at 2 weeks following surgery to be 6.6% distal and 0.6% proximal among our standard risk patients, and an overall 3-month PE incidence of 0.07%. We also found that older age and undergoing a knee arthroplasty were independent risk factors for DVT among this population. Importantly, we found all of the clinically significant VTE events resolved with appropriate anticoagulation, with no fatalities for this patient group. Thus, we recommend the above-mentioned protocol most strongly for younger hip implant recipients who are at low preoperative risk for VTE, and all other patients at standard preoperative risk with the caveat that older patients and those undergoing knee surgery are at higher risk and therefore should be monitored more closely following surgery.
Supplemental material
Supplementary_table_1_Summary_of_comparative_literature - Multimodal thromboprophylaxis in low-risk patients undergoing lower limb arthroplasty: A retrospective observational cohort analysis of 1400 patients with ultrasound screening
Supplementary_table_1_Summary_of_comparative_literature for Multimodal thromboprophylaxis in low-risk patients undergoing lower limb arthroplasty: A retrospective observational cohort analysis of 1400 patients with ultrasound screening by Meredith Harrison-Brown, Corey Scholes, Stephen L Douglas, Sami B Farah, Dennis Kerr and Lawrence Kohan in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of Joan Minty and Maria Falato with data collection and record retrieval. They also acknowledge with gratitude Mr Shivan Jassim for assistance with statistical analysis of an earlier version of this research.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L Kohan and S Farah report funding received from Smith and Nephew, Ltd. for patient recruitment, data collection and manuscript preparation, and consultant/speaker fees from Medacta, Inc. outside the scope of the submitted work. S Farah also reports serving as a paid expert orthopaedic advisor to the Therapeutic Goods Administration of Australia’s Advisory Committee on Medical Devices. C Scholes and M Harrison-Brown were paid employees of the senior author for the conduct of this work. D Kerr and S Douglas have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.