
Abstract
Objective:
Recurrent fifth metatarsal base stress fractures (MT5-BSF) in athletes present a challenging problem. The aim of this study was to evaluate the result of conservative treatment for the refracture of MT5-BSF after modified tension band wiring (MTBW).
Materials and Methods:
The outcomes of 15 elite athletes undergoing conservative treatment for refracture of MT5-BSF after MTBW were retrospectively reviewed. They were instructed to avoid weight-bearing with short leg cast for 6 weeks. After that, they started partial weight with a postop shoe. Stepwise exercise followed bone union by radiographs.
Results:
Thirteen cases (86.6%) had a complete bone union after a mean of 18.9 ± 8.6 weeks. Twelve cases (80%) returned to their previous activity level and maintained for at least two consecutive seasons.
Conclusion:
Eighty percent of all athletic patients with the conservative treatment for refractures with healed MT5-BSF after MTBW on the plantar-lateral side could maintain and return to their previous sports activity for at least 2 years.
Introduction
Fifth metatarsal base stress fracture (MT5-BSF) in athletes presents a challenging problem. Conservative treatment for this fracture type shows high rates of delayed unions, nonunions, and refractures. 1 –4 Therefore, operative treatment such as an intramedullary screw fixation, 4,5 modified tension band wiring, 6 (MTBW) or plantar plate 7 has been suggested as the treatment of choice for athletes and physically active patients, 8 although a refracture rate of 5–30% has still been reported. 6,9,10
After the report of six fracture cases of 1.9 cm from the fifth metatarsal base in 1902, 11 the proximal part of the diaphysis distal to the tuberosity was recognized as the “Jones fracture” and radiologically subdivided into three types by Torg in 1984 12 : (1) an acute fracture defined by a narrow fracture line without an intramedullary sclerosis, (2) fractures with a delayed union accompanied by the widening of the fracture line with intramedullary sclerosis, and (3) fractures with nonunion and full intramedullary obliteration by the sclerotic bone. In 1993, Lawrence divided the proximal fifth metatarsal fracture into three categories according to the anatomical position 13 : tuberosity (zone 1), the Jones-type (zone 2), and a base stress fracture (zone 3) (Figure 1). The Jones-type fracture is generally caused by a large bending force on the plantar aspect of the fifth metatarsal head. 14 On the other hand, a proximal fifth metatarsal base fracture in zone 3 is a stress fracture. According to biomechanical and clinical research findings, repeated stress between the base and head during acceleration or a cutting movement can provoke this type of injury. 15,16
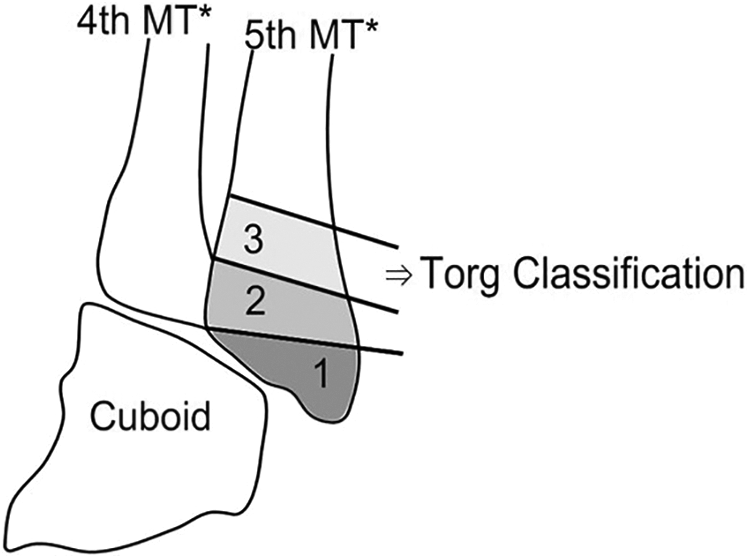
Lawrence and Botte’s classification of proximal fifth metatarsal fractures (zones 1, 2, and 3). Zone 3 was subclassified by Torg classification. MT: metatarsal.
Although the majority of investigators to date recommend surgical fixation of the initial Jones-type and MT5-BSF for high union rate and fast return to sports at their previous activity level, 9,17 –20 a consensus for the management of refractures has yet to be reached. Hunt and Anderson reported refracture cases after operative treatment for Jones fractures. Fifteen refracture cases were managed surgically with positive outcomes. 21 However, they did not distinguish between the Jones-type and MT5-BSF. They defined the proximal fifth metatarsal fracture as originally described by Jones 11 and Dameron 22 —a tuberosity and proximal portion of the shaft. Although these refracture cases could not fully represent MT5-BSF, from the results, the operative treatment for refractures appeared to be successful. 3,23 On the other hand, in a few cases, there have also been promising results of conservative treatment for refractures after operative treatment. 3,23 Despite favorable results in these cases, the zone of injury was not located clearly.
The purpose of this retrospective study was to make an evaluation of clinical and radiographic data of athletes who had undergone conservative treatment for the refracture of MT5-BSF after MTBW.
Materials and methods
The institutional review board approved this retrospective study. The treatment results were evaluated by reviewing hospital records and radiographs of MT5-BSF cases from March 2002 to October 2015. A total of 356 cases were included. Among them, 354 cases were athletes and 2 cases were ordinary people enjoying sports activity. All cases treated by conservative management or other surgical management except MTBW for initial MT5-BSF were excluded. Among them, 251 cases were treated by operative treatment using MTBW on the plantar-lateral side. 6 Inlay bone grafting was employed for Torg type III fractures. The patients were then immediately immobilized in a posterior short leg splint. After swelling around the operation wound was resolved, the patients were instructed to avoid bearing weight and to use a short leg cast for 6 weeks postoperatively. Afterward, they were allowed to start progressive weight-bearing to a tolerable extent with a walking boot. When they were clinically asymptomatic and when bone union progression was verified by plane radiographs and CT scans, they could attempt jogging. When the athletes could endure a more intense activity such as spurting and cutting, they were allowed to return to sports at their previous activity levels. To verify a bone union, CT scans were routinely performed about every 2 months postoperatively. A bone union was regarded as accomplished when the cortical bone continuity of the plantar side of the fracture (plantar) gap was reestablished with the callus on a CT scan. 24,25 All patients were with refracture of MT5-BSF after MTBW.
For inclusion, all patients had obvious clinical symptoms such as tenderness and pain aggravation when being active during sports, cortical discontinuity by CT scans or radiographs at the proximal fifth metatarsal area after MTBW on the plantar-lateral side for the MT5-BSF, and a minimum follow-up of 24 months.
Of the 251 cases, 29 cases (29 patients) were diagnosed with refracture. They decided to try conservative treatment and to delay operative treatment for 2–3 months for the failure of previous operative treatment. The patients were instructed to avoid weight-bearing and use a short leg cast for 6 weeks following which they were allowed to bear partial weight with a postop shoe. Radiologic evaluations were routinely repeated about every 2–4 weeks. When clinical symptom was resolved and restoration of cortical continuity was observed by plane radiographs, a CT scan was used to confirm bone healing. If bone healing was not confirmed, protective weight-bearing was sustained until bone healing using CT scans every 1 or 2 months. When bone union was confirmed radiographically, stepwise exercise such as jogging, running, sprinting, cutting, and jumping was allowed.
Among 29 refracture patients, 14 were excluded due to interrupted contact or an inadequate follow-up period. Finally, the remaining 15 cases were included and followed up for at least 24 months. They were all male: 12 were soccer players, 2 were basketball players, and 1 was a handball player. The mean age at the time of initial surgery was 21.2 ± 3.6 (standard deviation) (range 16–29) years. The time taken for bone union from initial surgery was 10.6 ± 4.1 (range 5.9–22) weeks. The time taken to return to jogging from initial surgery was 12.4 ± 3.9 (range 7.1–22) weeks. The time taken for the patient to return to their sports at previous activity levels from initial surgery was 18.3 ± 4.7 (range 12.1–29) weeks.
A delayed union was defined by the time the fractures did not heal for 6 months, but there was evidence of a callus formation or progression of closing of the fracture gap. A nonunion was determined if no definite progressive signs were observed of the healing of the fracture for 6 months postoperatively.
Short-term success was defined as the patient’s ability to return to their sports at their previous activity levels. The definition of long-term success was the maintenance of the former activity level for at least two consecutive seasons. We investigated both short-term and long-term success rates.
Results
All 15 patients with identified refractures initially underwent MTBW of the MT5-BSF. Demographic data of all patients are reported in Table 1. The time from the date of the surgery to the date of the refracture was 25.2 ± 15.9 (range 7.3–65.4) weeks. In 14 patients, they remembered the injury time of their refracture. One patient complained of insidious and aggravating pain for 3.5 months from the return to jogging after surgery.
Patient demographic and clinical data.

RTPA: return to previous activity.
For 12 patients who returned to sports at their previous activity levels, the time to the date of the refracture was 10.6 ± 14.2 (range 0–46) weeks (Figure 2). Three patients experienced refractures on the day they returned to sports at their previous activity levels. The mean length of the follow-up periods from the date of the refracture diagnosis to the last follow-up was 68.7 ± 35.1 (range 25–155) months. Of the 15 patients, a complete bone union was achieved in 13 (86.6%). Bone unions were achieved after a mean of 18.9 ± 8.6 (range 10–40.6) weeks. Of the 13 radiological bone union patients, 2 (15.4%) were delayed bone unions. In one of these, the patient underwent a third-time recurrence upon returning to his previous activity. This patient received intramedullary screw fixation. Two patients had a nonunion; one of them experienced a tension band wire breakage and pain (Figure 3) and then needed to retire from his career as an athlete. The other patient received an alternative operative treatment with an intramedullary screw fixation. Thus, of the 15 patients, 12 (80%) had short-term success and all retained their activity level for at least 2 consecutive seasons, which were regarded as long-term successes. The time periods from the fracture diagnosis to the return to jogging and sports at their previous activity levels were 22.2 ± 8.7 (range 11.6–42.4) and 23.2 ± 8.9 (range 12.6–45.4) weeks, respectively.

A 19-year-old male soccer player visited abrupt aggravation of insidious pain after training on the lateral aspect of left midfoot. Sclerotic bone lesion surrounding radiolucent lineal crack was observed at zone 3 on the base of fifth metatarsal bone. (a) He returned to his previous activity 1 week after the radiological recovery of bone continuity after MTBW. (b) Six weeks after return to the previous activity level, he visited complaining of pain aggravation. The crack reappeared on the radiograph. (c) He returned to his previous activity after the bone union of 4 months of conservative management. (d) He has kept his activity level for 2 years. MTBW: modified tension band wiring.

A 29-year-old soccer player returned to his previous activity 7 weeks after radiological nearly full bone union for tension band wiring of initial left MT5-BSF (a). One week after return to the previous activity, he visited complaining of sudden onset of his left foot pain again. The crack was widened and deepened, and tension band wire was broken (b). Three months of conservative management could not heal the fracture (c). MT5-BSF: fifth metatarsal base stress fracture.
Discussion
The previously reported time to achieve bone union in conservative treatment for recurrent MT5-BSF after surgical intervention is 14.5–24.5 weeks. 4,5,18,26 The mean time for bone union of conservative treatment of recurrent MT5-BSF after MTBW in this study was 18.9 weeks, which was similar to the above-mentioned results.
Many studies reported a healing rate of 30–72% with conservative treatment for initial MT5-BSF. 3,5,12,18,27 One of them reported a high failure rate (44%) after conservative treatment even in acute fracture. 18 However, 80% of conservative treatment for refractures with healed MT5-BSF after MTBW in this study successfully returned and kept their previous activity for at least two consecutive seasons. This result showed a higher successful long-term result than previous reports. This result suggests that conservative treatment of refracture after MTBW differs from that of initial MT5-BSF.
Carlo et al. reported that patients with a fifth metatarsal base fracture in zone 3 showed a slower return to work and sports activity than zones 1 and 2 fractures. Although none of their patients was a professional athlete, only half of zone 3 showed radiologic consolidation and took 20–22 weeks to return to sports activity. 28 This means some patients could achieve sufficient bone strength to endure the intensity and duration of the preinjury level activity after conservative treatment. However, about 4 months was required to return to their previous sports activity level. 4,5,18,26
Although a few reports have suggested a conservative treatment, 29,30 operative treatment has been advocated due to prolonged length of time to heal and high rate of delayed union, nonunion, and refracture after conservative treatment in initial MT5-BSF of athletes. 3,4,13,22,31 For this reason, the treatment protocol was changed to surgical management for all initial MT5-BSF in our cases.
Although fulcrum is still not well known in MT5-BSF, several biomechanical studies have demonstrated the setting of the dorsal to plantar loading over 2 mm distal from simulated transverse “fracture” at the metaphyseal/diaphyseal junction, a mean of 2 cm distal to the proximal tip of the tuberosity. 32,33 Taking the fifth metatarsal bone subjected to bending, it elongates more as the distance from fulcrum gets longer. Therefore, the bottom surface is subject to the highest tensile force. While the intramedullary screw passes through the center of cross-section area of the stress fracture region, the tension band wire is applied on the region of the highest tensile lesion. 4,24
In a biomechanical study using cadaver, plantar-lateral plating sustained greater cycles to failure and peak load than intramedullary screw fixation. 34 This suggests that plantar-lateral fixation could increase strength against cyclic loading above the bone’s ability on the fifth metatarsal base vulnerable region and renders it sufficient time for bone remodeling to adapt preinjury-level training intensity and duration compared to intramedullary fixation.
It is well known that by applying plate or tension band wiring on a tensile force region, the tensile force changes to the compression force on the opposite side of the tensile region. 35 In a proximal MT5-BSF, cyclic loading induces a distraction in the inferior-lateral cortex. The tension band wiring, another form of fixation applied on tensile region, neutralizes this traction force and compresses dynamically during loading (Figure 4). 35,36 It is not sure how refracture can happen without the loosening or failure of tension wire after healed MT5-BSF after MTBW. We presume that the restoration of cortical continuity using CT did not wholly reflect bone strength to return and sustain previous activity level and tension band wire could not fully cover all stress susceptible area because the wire is lineal and pinpoint overlapped at the center of figure of “8” between two screws. However, the transition to compression force from distraction force is considered to be the reason why 80% of patients with short-term success result in this study keep their activity for at least two consecutive seasons and one case with breakage in the tension band wire of the patients had failed to return to their previous activity.

The plantar-lateral side of the intramedullary screw gets tensile force when dynamic loading (a). However, the plantar-lateral side underneath tension band wire gets compressive force (b). MT: metatarsal.
Limitations of this study are the same as those inherent in a retrospective study. About 50% of patients (15 patients among 29 refracture patients) were followed up for at least 24 months, which induces selection bias. Furthermore, the number of these cases was too small for statistical analysis. In addition, control group was not used for comparison.
Conclusion
We suggest 80% of all athletic patients with the conservative treatment for refractures with healed MT5-BSF after MTBW on the plantar-lateral side could maintain and return to their previous sports activity for at least 2 years.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.