
Abstract
Purpose:
Multiple needle punctures (MNPs), for gap balancing in total knee replacement, have less variability in gap widening compared to the conventional released technique. This study aimed to evaluate the outcome of gap-balancing techniques in varus osteoarthritis (OA) knees, by serial MNP, after a total knee prosthesis trial component was placed, combined with repetitive knee manipulation.
Methods:
This study was a retrospective, case-matched study of 161 patients. The data were collected from varus OA knee patients, who had total knee arthroplasty by a single surgeon. Sixty-eight patients required MNP, combined with repetitive knee manipulation for gap balancing, and 93 patients did not. Both groups of MNP patients underwent the same surgical technique and postoperative care protocols.
Results:
Knee society scores, in terms of knee score and functional score, were not different in both groups when we started the study, at 6
Conclusion:
This study found MNP combined with repetitive knee manipulation was effective, reproductive, and a safe method for varus OA knee. We believe that the cycle of performed needle punctures, knee manipulation, and reevaluation could gradually lengthen the medial soft tissue without risk of over lengthening or medial collateral ligament rupture.
Introduction
Excellent knee functional after total knee arthroplasty (TKA) procedures requires proper surgical techniques that are aimed for perfect alignment and good stability. 1,2 Coronal ligament balancing is one of the most important steps that effects outcome and the longevity of implants. 3 In varus osteoarthritis (OA) knee, medial soft tissue is contracted while the lateral soft tissue is elongated. 4 Therefore, medial soft tissue release is performed to correct knee alignment. 5 There were many techniques that reported to have released medial soft tissue.
The conventional release method, which has been reported by Insall et al., is a widely used method. 6 Fixed varus deformity is corrected by a raised sleeve, consisting of medial collateral ligament (MCL), periosteum, and pes anserinus from medial proximal tibia. This technique was able to select the lengthening medial flexion gap or extension gap by selecting the release of either the anterior or posterior portion of superficial MCL, respectively. 7 However, this technique requires experience and precise surgical steps. In cases of superficial MCL being over-released or excessively detached, it might produce severe joint instability. 8 –10
The directed MCL lengthening with multiple needle puncture (MNP) or stab incisions was developed following the pie-crusting technique, wherein it uses multiple stab incisions to the lateral structure of the valgus knee. 9,11 –13 MNPs have been reported in cadaveric studies, in which they found less variability in gap widening compared to the conventional release technique. The study conclude that the MNP technique is safe and could reduce complications due to a reproducible technique. 14
The MNP procedure also has difference techniques. The principle of MCL lengthening was performed by stabbing the MCL, while the MCL was in the position of tension. Siong et al. reported that using a laminar spreader to expand the gap and stretch the MCL upon which the MCL is stabbed with an 18-gauge needle in selective positions requires lengthening: the anterior part for increasing flexion gap and the posterior part for increasing extension gap. 9 There was also a study that reported MNP within the flexion position, with a laminar spreader for balancing only flexion position, it then expanded the extension gap with total knee prosthesis trial component based on experience in that medial soft tissues could be expanded after knee motion. 15
In our practice, we also had experience in that medial soft tissues could be expanded following motion of knee, after the component trial was placed. We found that if we performed MNP until both the medial and lateral gaps were perfectly equaled, by using a laminar spreader, some patients might have a wider medial gap after insertion of the total knee prosthesis trial component, thus having knee movement that resulted in an unequal gap. Hence, we believed that performing serial MNP after total knee prosthesis trial component was in place, combined with repetitive knee manipulation in flexion and extension might reduce the chance of overstretching any medial soft tissue. Our study aimed to evaluate the clinical results and knee radiographic of this method in varus OA knee patients in comparison to varus OA knee patients; wherein, the surgeon could balance the gap without need of MNP.
Material and methods
This study was a retrospective case-matched study. Data were extracted from the electronic hospital database of OA knee patients, who had primary TKA; between January 1, 2017, and December, 2019. All patients were operated on by a single surgeon. This study was approved by the Ethics Committee and Institutional Review Board. Consent was waived by the ethics committee, and the hospital gave permission to extract information from the database.
The inclusion criteria were patients who had TKA for primary OA with varus alignment. The exclusion criteria were patients who had had any previous knee surgery. Finally, patients were grouped into two groups: MNP group and control group. The control group underwent the same surgical steps, but without final MNP for balancing the gap.
There were a total of 161 patients included in the study. The first group, consisting of 68 patients, required MNP for balancing the gap, with 93 patients not requiring MNP making up the control group. All patients were operated on by a single surgeon. A cemented posterior-stabilized knee prosthesis was used in all patients. The arthrotomy was performed utilizing the medial parapatellar approach. The medial capsule and deep MCL were released subperiosteally, with a periosteal elevator; then the medial osteophyte was removed. Anterior and posterior cruciate ligaments were resected. Distal femur was cut with an intramedullary guide, with a 5-degree valgus setting. Anatomical landmarks of the femur transepicondylar axis, posterior condylar axis, and AP axis were used to reference rotation of the femoral components. After the femoral cut and chamfer, posterior osteophytes were removed with a curved osteotome. A tibial cut was performed with an extramedullary guide that was set perpendicular to a tibial shaft, and the distal part of the guide was placed at the center of the ankle.
Following bone resection, flexion and extension gaps were initially evaluated with a block spacer. In cases of mismatch, such as knees with flexion contracture, the distal femur was further resected. Both medial and lateral gap balancing were evaluated following insertion of the trial components. The flexion gap was evaluated first, in cases of unbalancing varus OA knees that had medial gap narrowing, when at least one of the following signs was found: first, when performed anterior drawer of the tibia, both medial and lateral parts of polyethylene were not anterior subluxate uniformly (lateral tibial plateau would move forward more than the medial tibial plateau). Second, a varus stress test showed lateral opening of more than 2 mm. Finally, in severe unbalance, the condylar lift off sign might be found (femoral component was lifted off from the polyethylene on the lateral compartment). For patients who had the above signs, MNP was performed with tensest fibers of superficial MCL, by digital palpation, with an 18-gauge needle. Five punctures were performed at each time of release at the taut area of the superficial MCL. Then the knee was manipulated to be fully flexed, and further extended 10 times, following each set of punctures; after which, balancing was then reevaluated. Another set of punctures and knee manipulations were then conducted, until the knee was balanced in flexion. Then the extension gap was evaluated by varus and valgus stress test. In case of unbalancing, steps of MNP were performed in the extension at the posterior part of the superficial MCL, combined with knee manipulation and reevaluation. This cycle was repeated until the gap was balanced.
All of the patients underwent the same postoperative protocol. Quadricep isometric exercises and ankle pumping were started immediately after the operation. The day after surgery, all patients had a range of motion exercise; ambulated with a supportive device. Patients had follow-up visits at 6 weeks, 3 months, 6 months, and 1 year. Long-standing radiographing was performed at each visit. Knee society score 16 was recorded by doctors, who were blinded as to which group of patients they were evaluating.
Statistical analysis
Patient demographic data, such as gender, side of operation, Kellgren and Lawrence (KL) classification, 17 history of diabetes, and type of prosthesis, were evaluated with Pearson’s χ 2 test. T-test was used to compare age, weight, height, body mass index (BMI), operative time, tourniquet time, femorotibial angle, and knee society score. Postoperative medial joint opening was evaluated with Fisher’s exact test. All data were analyzed with R version 3.1.0 software (R Foundation for statistical computing, Vienna, Austria). Statistical significance was assumed when p < 0.05.
Results
The patients’ demographic data were not different between the two groups (Table 1). No differences were found between the groups in terms of age, gender, weight, height, BMI, side of operation, KL classification and percentages of patients with diabetes, tourniquet time, and type of prosthesis.
Demographic data.

BMI: body mass index; KL: Kellgren and Lawrence.
a Mean values with standard deviations.
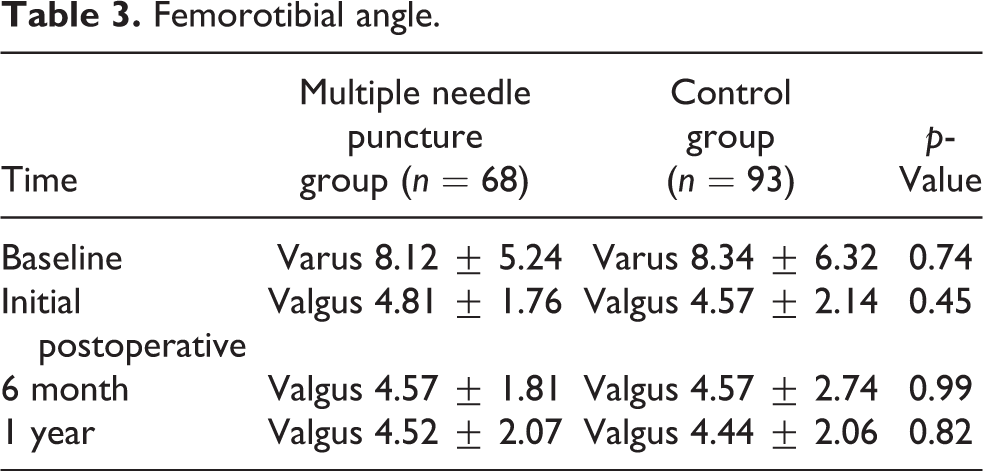
Knee Society Score in terms of knee score was not different in both groups, upon start of the study (p = 0.67). The knee score was also not significantly different at 6 month and 1-year follow-ups (at 6 months: p = 0.82, at 1 year: p = 0.15). The functional score at start, 6 months, and 1 year was not significantly different between either the MNP group or the control group (p = 0.65, 0.52, and 0.33, respectively) (Table 2). Additionally, femorotibial angle was not significantly different at the start of study, initial postoperative, 6 months, and 1 year (p = 0.74, 0.45, 0.99, and 0.82, respectively) (Table 3).
Knee society score.

Femorotibial angle.
Medial joint opening in radiographic was found in both groups, at initial postoperative and 1-year follow-up. At the initial postoperative, there was 3% of patients (2 patients) in MNP and 7.5% of patients in the control group that had medial joint opening (7 patients) (p = 0.21). At 1-year follow-up, there was not an increasing number of patients with radiographic medial joint opening (3% of patients (2 patients) in the MNP and 4% of patients in the control group (4 patients, p = 0.65)). There were no surgical wound infections or reoperations for either group.
Discussion
Ligament balancing in TKA is an important step that effects postoperative function and longevity of prosthesis. 3 Medial release of fixed contracture of medial soft tissue in varus OA knee is necessary to obtain perfect gap balancing. 5 MNP is one technique that has reported to be successful in reaching this goal. The benefits of MNP are reproducible and have less variability in gap widening, compared to the classic subperiosteal release technique. 14 However, the MNP technique has been reported with varied technical steps. 9,15,18 Our study aimed to evaluate the effect of MNPs, under the knee prosthesis trial component after insertion, combined with knee movement in varus OA knee patients, in comparison to those who did not require release.
Our study found that the postoperative clinical outcomes, which were evaluated with the Knee Society Clinical Rating System in terms of knee score and functional scores, were not different in our two groups. Similarly, in previous studies by Kim et al., it was found that the Knee Society Score and Western Ontario and McMaster Universities Osteoarthritis Index score were also not different between patients requiring MNP and those that did not. 15 There was also another study that found no differences in the American Knee Society score, Western Ontario and McMaster Universities Osteoarthritis Index, SF-36, Short Form 36 between MNP and non-MNP patients. 9
The incidence of medial laxity in radiograph, after follow-up, was not different between the MNP group and the control group in this study. These results are supported by two previous studies that reported no differences in radiographic medial opening angle with valgus stress test at 1 year. 9,15 The postoperative femorotibial angle in MNP patients was not different than that of the control group at any time point of follow-up in our study. Other studies using MNP also found similar results. 9,15
All of our patients, in this study, could achieve intraoperative ligament balancing without noticing any over releasing or medial instability. Hence, our patients did not require any constraint implant or reconstruction of medial soft tissue. This contradicted some previous report that considered the use of constrained inserts, following MNP in cases that had a presence of residual ligament imbalance, or irreconcilable flexion/extension mismatch. 19 In so saying, we believe that our technique that conducted sequential MNP combined with repetitive manipulation of the knee could gradually stretch medial soft tissue. The gap balancing was evaluated following each cycle of puncture and knee movement. Therefore, this step could avoid over lengthening with a technique using only the laminar spreader, because the soft tissue might be stretched more after knee movement with trial components.
This study has a number of limitations. First, this study evaluated standing knee radiographic without varus or valgus stress test views. So, medial laxity might be found only in severe cases. Second, this study evaluated only extension stability in knee standing radiographic. However, both groups of patients had no difference in postoperative function, and there were no reoperations due to instability problems. Third, authors didn’t collect the number of sets of MNP, which we performed in each case. This was based on our experience in that the number of MNP varies from case to case and not related to preoperative varus deformity. Finally, this study reported only 1-year postoperative follow-up; further studies with longer postoperative follow-up should therefore be performed.
Conclusions
This study found that MNP combined with repetitive knee manipulation was effective, reproductive, and a safe method for varus OA knees. We believe that the cycle of performed needle punctures coupled with knee manipulation and reevaluation could gradually lengthen medial soft tissue, without risk of over lengthening or MCL rupture.
Footnotes
Acknowledgements
The authors wish to thank Andrew Jonathan Tait for his assistance in proofreading the English of this report.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by the Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand (grant number 62-110-11-1).