
Abstract
Stenosing tenosynovitis of the extensor digiti minimi (EDM) without trauma is very rare. We report a 21-year-old woman who presented with dorsoulnar wrist pain during palmar wrist flexion and soft tissue mass at the site of pain. Ultrasonography and magnetic resonance imaging showed a round mass radial to the EDM tendon. Conservative treatment for 3 months failed to improve the patient’s pain levels. Intraoperative findings revealed smaller radial slip of the EDM tendon, and bifurcation of these was under the distal portion of the extensor retinaculum (ER). Surgical release of the ER, resection of the smaller slip of the EDM tendon, and tenosynovectomy were performed. Histological examination showed tenosynovitis. At the final follow-up 1 year postoperatively, she was asymptomatic. A literature review suggested that stenosing tenosynovitis of the EDM tendon might be caused by frequent use of the hand with a background history of bifurcation of the EDM tendon.
Introduction
In tenosynovitis of the hand and wrist, trigger finger of a thumb and fingers and de Quervain disease are commonly exhibited in clinical settings. 1 However, stenosing tenosynovitis of the extensor digiti minimi (EDM) without trauma is very rare and has been described in only 10 cases in the literature written in English. 2 –7 The purpose of this case report was to report on a patient with non-traumatic stenosing tenosynovitis of the EDM treated by surgery. We also present a review of the literature on its etiology, cause, treatment, and clinical outcomes.
Case report
Informed consent for publication was obtained from the patient, and this case report was approved by the institutional review board. A 21-year-old left-handed woman was referred to us for further treatment due to 3-month history of pain and soft tissue mass of the left hand. She was employed as an illustrator with 1-year career history. On busy days, she worked 20 h/day. She had no remarkable medical history.
Initially, she felt pain at the dorsoulnar aspect of the left wrist during palmar flexion of the wrist while working and noticed a soft tissue mass at the site of pain. Therefore, she visited a clinic and underwent physiotherapy using low-frequency therapy device for 3 months, which failed to improve her symptoms. She reported that the size of the mass did not change during this 3-month period.
Initial examination revealed a firm mass that was 2–3 mm in diameter on the dorsoulnar aspect of the left wrist (Figure 1(a)). The skin was not reddish, and the mass was not adherent to the overlying skin as it moved during small finger motion. The mass was accompanied by tenderness. There was no triggering and limited range of motion of the left little finger. Plain radiography showed no remarkable findings. Ultrasonography revealed that the low echoic solitary mass was located radial to the extensor of the small finger. Magnetic resonance image confirmed a round mass radial to the EDM tendon. On T1-weighted images, the mass had a low signal intensity; T2-weighted images displayed the low signal intensity of the mass and the high signal intensity of its surroundings (Figure 1(b) and (c)). Fibrous tumor was suspected as a preoperative diagnosis; we planned incisional biopsy for definite diagnosis. She scored 5.8 in disability/symptom and 25 in work section on the Disability of the Arm, Shoulder, and Hand (DASH) questionnaire.

Preoperative macroscopic photograph and MR images. (a) Preoperative macroscopic photograph. Arrow indicates the site of the palpable soft tissue mass. (b) T1-weighed and (c) T2-weighed axial image of MRI. White arrow head indicates the pathological lesion. Asterisk shows the extensor digiti minimi tendon. MR: magnetic resonance; MRI: magnetic resonance imaging.
Operative treatment was performed under supraclavicular regional anesthesia using a pneumatic tourniquet. A transverse incision was made over the mass. After releasing the distal side of the extensor retinaculum (ER), we observed that the EDM tendon had a small bifurcation radial to it, and the bifurcated site of these two tendons was under the distal portion of the ER (Figure 2(a), (b) and (c)). Additionally, there was extensive tenosynovitis around the site of the bifurcation. There was no space-occupied lesion. Intraoperative findings led us to a diagnosis of stenosing tenosynovitis of the EDM tendon due to bifurcation of the EDM tendon at the distal aspect of the ER. Resection of the smaller radial slip of the EDM tendon and tenosynovectomy were performed (Figure 2(d) and (e)). Histological examination for tenosynovitis showed proliferation of the synovium and capillary vessels and infiltration of lymphocytes, which was compatible with a definitive diagnosis of stenosing tenosynovitis of the EDM tendon (Figure 3).
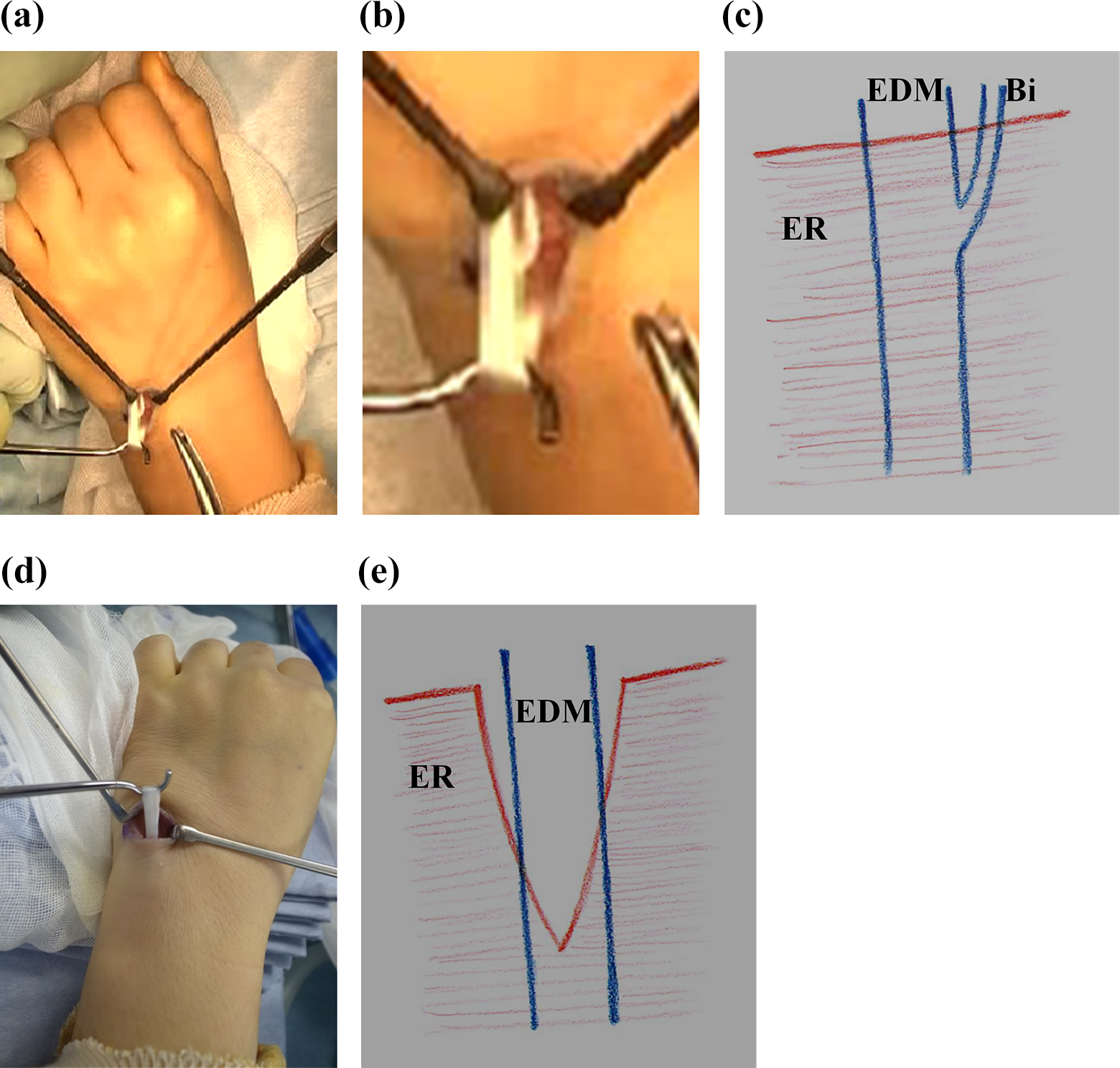
Intraoperative photograph. (a) The EDM tendon has smaller radial slip. (b) Enlarged Enlargedview of the bifurcation of EDM tendon. (c) Schema of the lesion before operation. (d) After resection of the smaller radial slip. (e) Schema of the lesion after operation. EDM: extensor digiti minimi; ER: extensor retinaculum; Bi: bifurcation of EDM tendon.

Histological examination of the tenosynovium. Proliferation of the synovium and capillary vessels, and infiltration of lymphocytes are noted.
The postoperative course was uneventful. At 4 weeks postoperatively, she reported relief of her pain. At the final follow-up 1 year postoperatively, she was asymptomatic and did not have any disability during daily life and while working. Her DASH score was 1.7 in disability/symptom and 0 in the work section.
Discussion
Stenosing tenosynovitis or trigger finger of the flexor tendon is exhibited by a locking or clicking of a thumb or a finger and caused by a mismatch of size between the flexor tendon and A1-pulley. 8 The prevalence of trigger finger is 2.6% in the nondiabetic population. 9 Moreover, stenosing tenosynovitis of the EDM is rarer than trigger finger and de Quervain disease. 1
On reviewing the literature on stenosing tenosynovitis of the EDM without trauma, we discovered 10 cases (11 wrists) with available surgical findings and outcomes. Table 1 lists the demographic data of patients. 2 –7 The mean age of the patients was 29 years, and it was younger than that of trigger fingers. 10,11 Patient occupations and hobbies involved the frequent use of hands.
Demographic data of patients with stenosing tenosynovitis of the extensor digiti minimi on literature review.
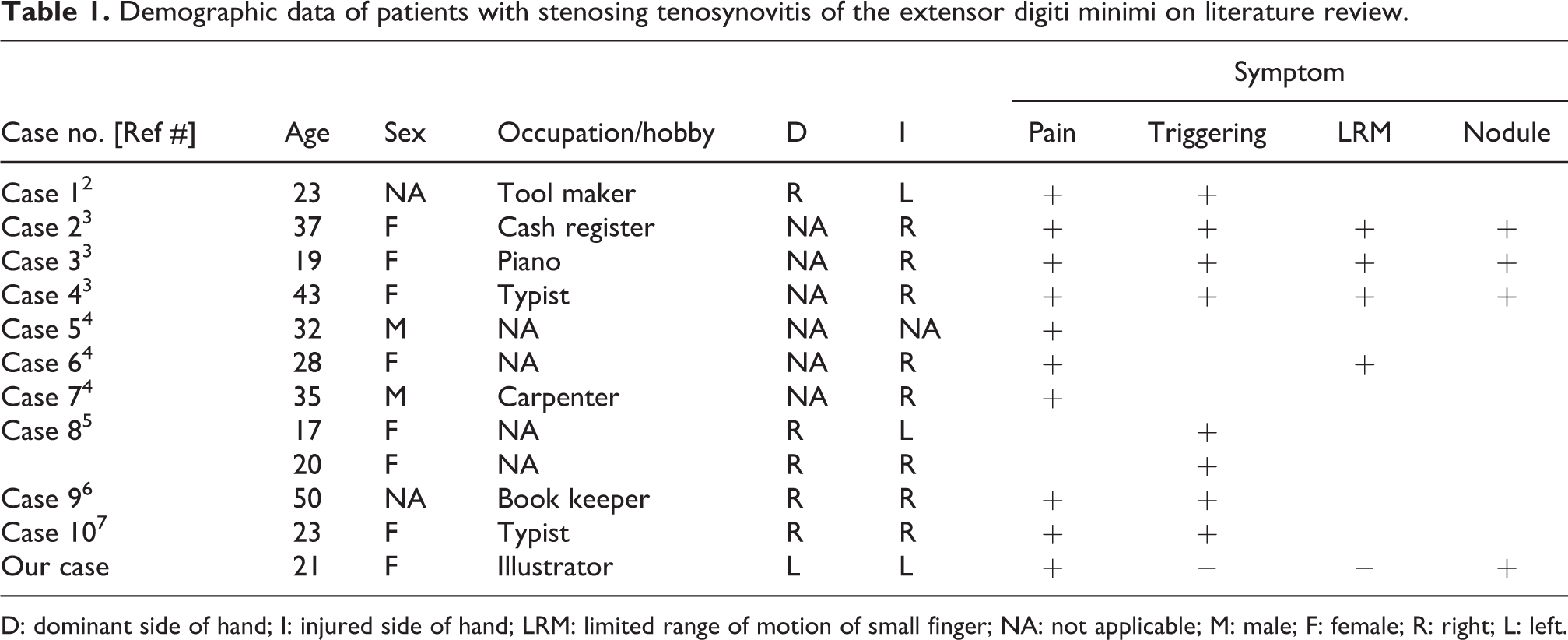
D: dominant side of hand; I: injured side of hand; LRM: limited range of motion of small finger; NA: not applicable; M: male; F: female; R: right; L: left.
There were frequent anatomical variations in the extensor tendons of the ulnar side than the radial side, including multiple tendon slips of the EDM, variable attachments of the extensor digitorum communis (EDC), and deficiency of the EDC in the little finger. 12,13
On review, there were four causes of stenosing tenosynovitis of the EDM based on the original reports, which occurred at the site of EDM separation, tendon sheath-like structure, synovial septum, and hypertrophy of ER (Table 2). First, the duplication of the EDM was well described in a previous cadaver study; our review showed duplication of the EDM in 7 of the 12 wrists. Schenck reported that 48 of the 57 cadaver hands had duplication of the EDM and the site of the division was proximal to the ER in 15%, at the level of the ER in 81%, and distal to the ER in 4%. 13 As shown in the present case, three wrists showed bifurcation of the EDM distal to the ER, and symptoms were recovered by release or excision of the ER. 6 Thus, the important anatomical cause is not duplication of the EDM, but the site of duplication (distal to the ER), which is a finding that can be supported by the decreased frequency of cadaver wrists exhibiting division of the EDM distal to the ER. Second, anatomical findings of the tendon sheath-like structure or synovial septum using cadavers are reported. 4,12,14 Third, Khazzam et al. reported hypertrophy of the ER in a diabetic patient. 5 Frequent use of hands might precipitate stenosing tenosynovitis of the EDM tendon with a background history of the bifurcation of the EDM.
Pathogenesis and treatment for patients with stenosing tenosynovitis of the extensor digiti minimi on literature review.

TS: tendon sheath; TSLS: tendon sheath-like structure; SS: synovial septum; Hyper., hypertrophy of extensor retinaculum; ER: extensor retinaculum; Bifur., bifurcation of EDM; inj., injection; PT: physical therapy; EDM: extensor digiti minimi; Res., resection; S: synovectomy; Rel., release; NA: not applicable.
For conservative treatment, steroid injection for three wrists and medication for two wrists were not effective. While a prospective study showed that a single steroid injection was effective in 64% of patients with trigger finger, there might be publication bias to these outcomes because all cases with stenosing tenosynovitis of the EDM were treated by surgery. 11 Surgery showed excellent results, and all wrists became asymptomatic postoperatively. In the present case, release of the ER and resection of the EDM minor slip were performed, but the latter might not be necessary. The limitation of this case report was no assessment for the distal attachment of the EDM minor slip.
Conclusion
Stenosing tenosynovitis of the EDM is rare and has several causes due to variations in anatomical structure. Clinical results by surgical treatment were excellent, and quality of life in patients with stenosing tenosynovitis could be improved after surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.