
Abstract
Background:
Screw fixation used in modified Kidner procedures to treat persistent symptomatic accessory navicular in adult cases is often challenging in adolescent cases with a small accessory fragment. The present study aimed to document the clinical effect of a suture anchor stabilization technique applicable to such cases where osteosynthesis is considered an ideal outcome.
Methods:
Consecutive clinical cases who received this surgical treatment from 2009 to 2016 were retrospectively reviewed. The focus of interest included radiographic union of the accessory bone, changes in symptoms evaluated using a validated clinical outcome scale introduced by the Japanese Society for Surgery of the Foot, and changes in the medial arch bony alignment measured in lateral weight-bearing plain radiographs.
Results:
Twenty-two feet in 15 individuals (11 females and 4 males, age at surgery 10–16 years) were identified. In 14 feet (64%), radiographic bone union was confirmed within 8 weeks postoperatively. At the final follow-up ranging 12–51 months postoperation, the clinical scores have significantly improved (p < 0.001) to 96 ± 5.71 (mean ± standard deviation, range 87–100), from 54 preoperatively. Radiographic measurements revealed significant postoperative increase of the sagittal talar tilt angle (p < 0.001, increment 4 ± 3°, range 0–11) and the talo-first metatarsal angle (p < 0.001, increment 5 ± 4°, range 0–12). No significant changes were identified in the calcaneal pitch angle, first metatarsal tilt angle, calcaneo-navicular angle, and the navicular height.
Conclusion:
Despite the modest bone union rate, the clinical outcomes suggest distinct symptom-relieving effect, at least in the short- to midterm, while the radiographic measurements suggest positive biomechanical effects. The present suture-anchor stabilization concept appears to be a promising treatment option for persistent symptomatic accessory navicular in adolescent cases.
Introduction
In type II accessory navicular, the accessory bone and the navicular body are connected with fibrous (unossified) cartilage, and this connection can be destabilized by minor injuries, such as ankle sprain to form a pseudarthrosis. Under repetitive stress, this destabilization is associated with microfractures and bone remodeling in the adjacent periosteum which may give rise to symptoms due to free nerve endings there. 1 In other words, the accessory navicular becomes symptomatic when it takes on pseudarthrosis characteristics. 2,3 For persistent symptomatic accessory navicular, when conservative management is unsuccessful, removal of the accessory fragment followed by repair of the tibialis posterior (TP) tendon insertion (also known as the Kidner procedure 4 ) has long been regarded as the reference standard operative option.
The TP muscle plays an important role in maintaining the medial arch construction of the foot 4 by actively inverting the forefoot complex with respect to the hindfoot complex. Accordingly, the risks of either simple excision or the Kidner procedure appear to be well explainable anatomically, particularly for accessory navicular with a large fragment (i.e. Veitch type II), 5 in which the majority of the TP tendon inserts into the accessory fragment to be excised. Removal of such a mechanically integrated structure could reduce the tendon-to-bone force transmission, potentially leading to (or exacerbating) TP dysfunction over time. 6
Surgical treatment strategies for persistent symptomatic accessory navicular are generally categorized into three types of procedures, including simple extraction of the accessory fragment, 7,8 fragment extraction followed by retracting repair of the TP tendon attachment (also known as Kidner’s procedure), 4,9 –13 and osteosynthesis of the accessory fragment (typically, reattachment using a bone screw). 6,14 –17 For the second of those strategies, several techniques to reattach the TP tendon to the navicular body 9 –11 have been described in the literature, but the efficacy of those procedures to restore or maintain TP function in adolescent patients has not been well addressed. For that reason, we adopt the third strategy for type II accessory navicular, where a considerable proportion of the TP tendon fibers are attached to the accessory fragment.
Anatomically, “the fibrous tendon to bone enthesis is established through a structurally continuous gradient from uncalcified tendon to calcified bone.” 18 The feasibility of replicating the physiological function of such a complex enthesis construct by directly anchoring tendon fibers to bone surface is questionable. Reattachment of the intact tendon insertion complex, including Sharpy’s fibers running across the tendon-to-bone junction 19 into the accessory fragment seems more promising, particularly considering the vigorous bone regenerative capability in adolescents. 15
For adults, to accomplish this objective, our basic procedure for type II accessory navicular consists of: (1) refreshment of the “pseudo arthrosis” lesion (i.e. resection of the fibrous tissue) between the accessory bone and the navicular body, (2) wedge osteotomy for the navicular body side (so as to relieve symptoms associated with the large bony protuberance), and (3) internal fixation of the accessory fragment using a cancellous bone screw along with a washer.
However, due to small bone fragments inherent in adolescent cases, screw fixation commonly utilized for adult cases is often challenging. In the present case series, an alternative minimally invasive surgical stabilization technique intending osteosynthesis, specifically non-screw internal fixation using two types of suture anchors was utilized for adolescent cases with a relatively small accessory fragment. The aim of this study was to document the efficacy and limitations of this treatment innovation.
Subjects and methods
The clinical records of consecutive cases of persistent symptomatic accessory navicular, treated with the procedure of interest from January 2009 to December 2016, were reviewed with appropriate approval from the institutional review board of Dokkyo Medical University Saitama Medical Center (#1710). The need for informed consent was waived due to the retrospective nature of this study. This procedure was selected for symptomatic cases of type II accessory navicular, where the size of the accessory fragment was regarded as insufficient for screw fixation. All patients had received conservative treatment for more than 3 months. The operative records during the search period included symptomatic accessory navicular surgeries for a total of 34 feet in 26 adolescents. Of those, suture anchor fixation was performed in 22 feet (65%) in 15 subjects from 10 to 16 (mean 12) years, including 11 females and 4 males, with a relatively small accessory bone.
Surgical technique
An arc-shaped longitudinal skin incision, approximately 3 cm, was placed on the medial aspect of the mid foot, along the plantar aspect of the navicular. The surgical field was expanded to identify the site of the accessory navicular, with fluoroscopic guidance. Once identified, the fibrous interface between the navicular body and the accessory bone was resected, while preserving the more distal excursions of the TP tendon uninjured. The proximal surface of the accessory fragment was refreshed by minimally resecting the fibrous tissue and consolidated bone, while preserving the integrity of the tendon insertion. For the distal surface of the navicular body, a wedged osteotomy was made to refresh the fixation surface, as well as to normalize the size and shape of the tuberosity. With these actions, while the accessory fragment was retained for the purpose of preserving the TP tendon insertion, the concave surface of the accessory fragment was excised, and pressure was relieved from the medial navicular protuberance. Next, a suture anchor, either a conical titanium alloy screw (TWINFIX Ti®; Smith & Nephew Inc., Andover, Massachusetts, USA) or a soft anchor (JuggerKnot®; Zimmer Biomet Inc., Warsaw, Indiana, USA) was installed in the navicular body, and the attached sutures were used to secure the accessory fragment, along with the TP tendon (Figure 1 (a) to (d)). The conical titanium alloy anchor was utilized in 16 feet, while the soft anchor was utilized in 6. Finally, cancellous bone harvested from the osteotomized tuberosity fragment was grafted into the recess between the fragment and the body, followed by skin closure. Postoperatively, short-leg casting, with the ankle kept in the neutral position, was applied for 4 weeks. Radiographic bone union of the osteosynthesis interface was assessed at 2- to 4-week intervals for 8 weeks. At 12 weeks after surgery, patients were permitted to return to sports, regardless of bone union status. Clinical and radiographic examinations with occasional CT imaging were continued at 3- to 6-month intervals for the duration of follow-up.

(a) The fibrous interface between the navicular body and the accessory fragment is resected while preserving the inferior extension of the PTT uninjured. The proximal surface of the accessory fragment was refreshed by minimally resecting the consolidated bone, while preserving the integrity of the PTT insertion. (b) Wedged osteotomy of the distal navicular body was performed, refreshing the surface for fixation of the accessory fragment, and to normalize the size and shape of the tuberosity. (c) The accessory navicular, with the PTT, was attached to the navicular bone, using a suture anchor. (d). Postoperative plain radiographs of a 16-year old male.
Outcome assessment
Clinical evaluations were executed preoperatively and at the final follow-up, a minimum of 12 months postoperatively. The Japanese Society for Surgery of the Foot (JSSF) midfoot scale, which has been validated elsewhere, 20,21 was utilized to assess changes in symptoms. Radiographic bone union was defined as disappearance of the gap between the navicular body and the accessory fragment in either plain radiographs or CT images. Change in the tarsal bone alignment of the medial arch was measured in lateral weight-bearing plain radiographs preoperatively and at the final follow-up. The parameters of interest (Figure 2) included the sagittal tilt angles of the calcaneus, talus, and the first metatarsal shaft, from which the talo-first metatarsal and talo-calcaneal angles were computed. The navicular height from the floor (measured at the dorsal end of the talo-navicular joint, standardized by the length from the posterior end of the calcaneal tubercle to the anterior end of the first metatarsal head) was also computed. These measurements were executed by two board-certified orthopedic surgeons and a senior resident, and the outputs were averaged across observers. A paired t-test was utilized to identify changes between the time points, with significance set at p ≤ 0.05.
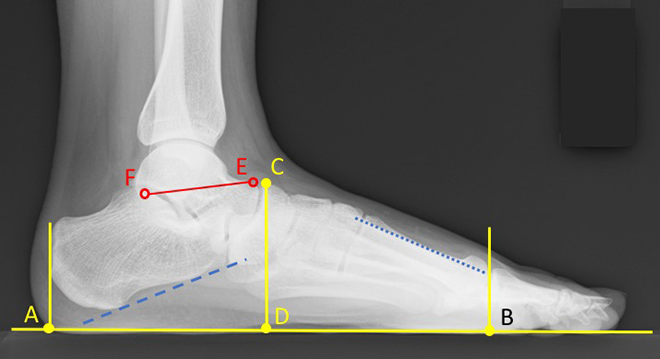
Calcaneal pitch angle is the angle between bottom of calcaneus and AB. Navicular height is the ratio of CD/AB. Sagittal talar tilt angle is the angle from EF to AB. Talo-first metatarsal angle is the angle from EF to first metatarsal axis angle. (A) Point of intersection of perpendicular line placed at the most posterior border of the calcaneus to floor. (B) Point of intersection of perpendicular line placed at the most anterior point of the first metatarsal bone to floor. (C) Dorsal edge about navicular bone at talo-navicular joint. (D) Point of intersection for perpendicular line about point C to floor. (E) Dorsal edge about talus at talo-navicular joint. (F) Tip of medial side of the posterior facet. Blue dotted line indicates axis of the first metatarsal bone; blue dashed line indicates bottom of calcaneus.
Results
At the final follow-up, ranging from 12 to 51 months after surgery, radiographic bone union was confirmed by X-ray in 14 of the 22 feet (64%) and non-union cases were confirmed by CT scan. Bone union rates were 81% (13 of 16) in the metal anchor cases and 12% (1 of 6) in the soft anchor cases. JSSF scores improved in all cases, from 54 points preoperatively to 96.3 postoperatively (range 87–100). All patients were able to return to sports without complications, and all patients reported satisfaction at the final follow-up. None of the incomplete union cases complained of residual symptoms requiring revision surgery, as indicated by the final JSSF scores ranging from 87 to 100 points. In our small series, there were no cases of infection, and no cases requiring removal of anchors or revision surgery for any reason. The lateral weight-bearing plain radiographs, both preoperatively and at the final follow were available only in 16 feet in 11 subjects (Figure 3). In the sagital talar tilt angles, a significant increase (p < 0.001) was found, from the preoperative 7 ± 4° (mean ± standard deviation, range 1°–20°) to 11 ± 5° (2°–22°) at the final follow-up (Figure 4). The talo-first metatarsal angles also significantly increased (p < 0.001), from 28 ± 5° (20°–40°) to 33 ± 5° (23°–43°) (Figure 5). No significant postoperative changes were found in the calcaneal pitch angle (p = 0.24; Figure 6), nor there were changes in the navicular height ratio (p = 0.86; Figure 7).

(a) Preoperative lateral weight-bearing plain radiographs of a 14-year-old female. (b) Postoperative radiograph after 51 months at the final follow-up. The preoperative JSSF midfoot scores improved from preoperative 54 points to 100 points at the time of the final follow-up, 51 months postoperation. In standing position, simple X-ray images calcaneal pitch angles improved from 16° to 18°, navicular height improved from 0.31 to 0.35, sagittal talar tilt angles improved from 3° to 6°, and talo-first metatarsal angles improved from 21° to 30°. JSSF: Japanese Society for Surgery of the Foot.

Sagital talar tilt angle. *Significant increase (p < 0.001) was found from the preoperative to at the final follow-up.
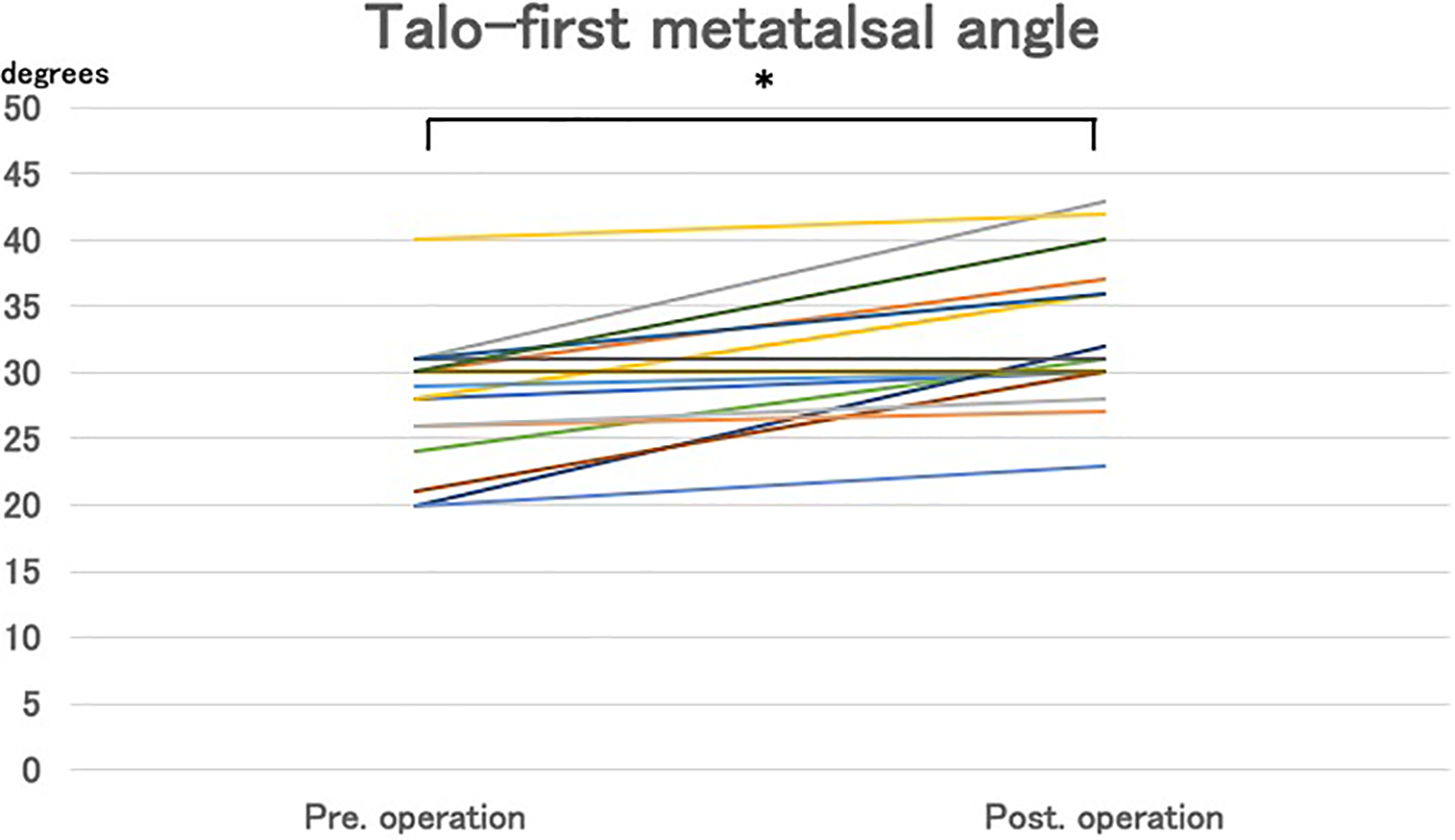
Talo-first metatalsal angle. * Significant increase (p < 0.001) was found from the preoperative to at the final follow-up.
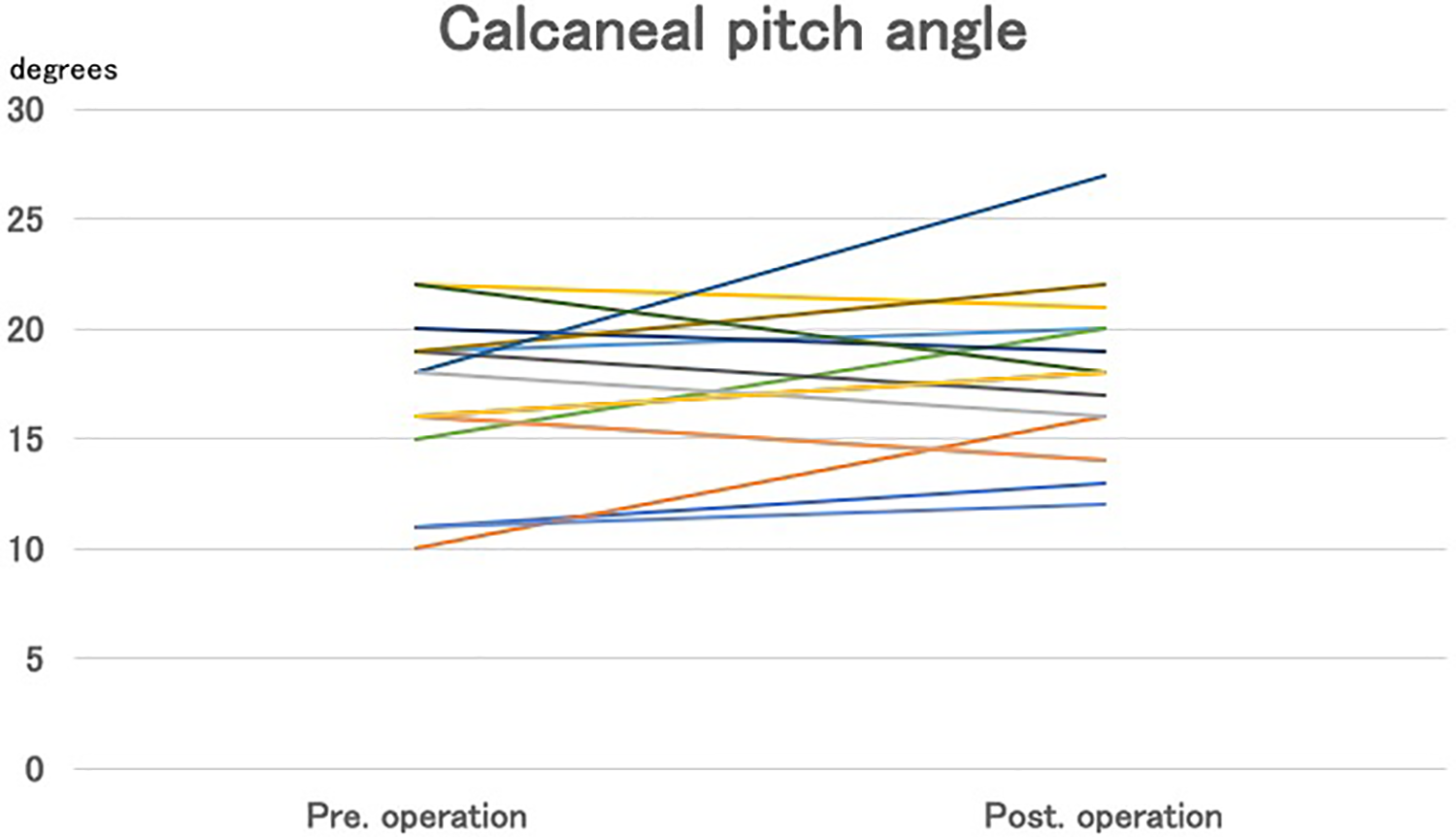
Calcaneal pitch angle. p = 0.24: no significant postoperative changes were found.

Navicular height. p = 0.86: No significant postoperative changes were found.
Discussion
Radiographic fragment union was confirmed in less than two-thirds of the cases in the present series. The union rate was particularly lower when the soft anchor was utilized, implying that this type of suture anchor may be unsuitable for an osteotomized cancellous bone surface on the adolescent navicular. For improved bone union outcomes, a more reliable internal fixation technique (such as a screw-type suture anchor combined with a small anti-rotation pin or screw) might be effective.
Despite the modest bone union rate, symptom relief was highly reproducible. The histological findings in the type II accessory navicular are characterized by a proliferation of vascular mesenchymal and cartilaginous tissue, fibrous connective tissue accompanied by collagen fibrosis hyperplasia, and bone remodeling, which is consistent with that in pseudoarthrosis. 2,3 In a histological study of symptomatic tarsal coalition, Kumai et al. documented a similar vascular proliferation, and expression of abnormal free nerve endings in the repetitively stressed periosteum and articular capsule surrounding the non-osseus coalition, which was regarded as a potential source of pain under abnormal mechanical loading. 1 Assuming similarity in the mechanism of pain under repetitive stress in accessory navicular, the osteotomies in our procedure would have eliminated abnormal nerve endings in the boundary bone tissue, presumably explaining the effective pain relief. In addition, normalization of the size and shape of the navicular tuberosity by plastic osteotomy might have reduced the risk of inflammatory subcutaneous bursitis occurring at the bony protuberance of the accessory navicular.
The postoperative changes in the medial arch alignment suggest amendment in the tarsal joint mechanics. A tendency toward flatfoot in patients with symptomatic accessory navicular has been reported. 22 In adult surgical cases, Chung and Chu 14 reported that osteosynthesis using a metal fixation screw improved tarsal bone alignment in adult surgical cases. In contrast, after Kidner-type procedures, Cha et al. 23 did not find such improvement, while Scott et al. 17 reported that some cases had progressive postoperative loss of the medial longitudinal arch. In our series, although the navicular height did not exhibit significant changes, increases of the talo-first metatarsal angle suggest some sort of tarsal arch reinforcing effect, presumably from improved TP muscle function.
Unfortunately, the data set from this small-cohort, retrospective, non-control study with short follow-up does not support definitive claims regarding the above suggested advantages of the present fragment stabilization strategy. A larger scale prospective randomized study would be needed, and biomechanical evaluation is needed to optimize the surgical technique to stabilize the small accessory fragment in adolescent cases.
Conclusion
For persistent symptomatic type II accessory navicular in adolescents, when TP tendon dysfunction after accessory fragment resection would be a concern, but where the fragment size would not be large enough to accept a fixation screw, the present suture anchor stabilization technique should be considered as a surgical option.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.