
Abstract
Purpose:
Medial meniscus posterior root tear (MMPRT) should be repaired to the correct position as possible to maintain hoop tension of the meniscus. In this study, we propose a comparison of the outcome between the medial tunnel and the lateral tunnel in the pullout suture technique using the tibial tunnel for anatomical repair of posterior root tear of medial meniscus.
Methods:
From April 2010, of patients who underwent pullout suture, 51 cases (24 medial tunnel group (MTG) and 27 lateral tunnel group (LTG)) were able to follow-up with second look arthroscopy. Original Coronal Ratio of Root Attachment (CRORA) was defined as the ratio of the distance from the medial edge of the tibial plateau to the root attach site divided by the entire tibial medial–lateral width on preoperative computed tomography. Error between postoperative CRORA and original CRORA was calculated. We compared this error, clinical outcome, and arthroscopic finding between MTG and LTG.
Results:
The mean error ratio of postoperative CRORA divided by original CRORA was 0.86 ± 0.11 in MTG, which was significantly (p = 0.001) lower than that (1.02 ± 0.06) in LTG. The mean value of the root attach point in the MTG with a post/original CRORA value of 0.86 ± 0.11 means statistically significant medialization after the operation. There was no statistically significant difference in changes of International Knee Documentation Committee (IKDC) and Lysholom score between MTG and LTG. The difference between the two groups of arthritis progression was not statistically significant.
Conclusion:
In patients with MMPRT, CRORA may provide a basis for coronal assessment of root repair position before and after surgery, and lateral tibial tunnel technique can help anatomical repair by reducing technical error due to guide pin slip medially compared to medial tibial tunnel technique.
Introduction
Medial meniscus posterior root tear (MMPRT) was first reported by Pagnani et al. 1 Appropriate treatment is important because it accelerates the progression to arthritis by eliminating hoop tension in meniscus and loss of load transmissibility. 2 In the past, MMPRT was mainly treated by meniscectomy. Improvement in clinical score can be expected. However, pullout repair is the main treatment for MMPRT in recent years because of its proven superiority over meniscectomy in that it will delay arthritis progression. 3 MMPRT should be repaired to the correct position as possible to maintain hoop tension of the meniscus. If the refixation position of the medial meniscus is located laterally than the anatomical position, excessive stress will be applied to the meniscal body. On the other hand, when placed in the medial, it will lose the ability of meniscus to control tibiofemoral contact stress due to lack of hoop tension and consequently lead to the development of arthritis. 4
In most studies, medial tibial tunnels have been used for transtibial repair of MMPRT. 3,5 –10 However, in the process of making tibial tunnel during the pullout suture technique, we often experience medialization of tunnel exit because the guide pin often slips along the medial border of the tibia when using the medial tunnel. Therefore, it has been difficult to attach the medial meniscus to a proper position. Conversely, when lateral tunnel is used, medialization of tunnel exit is less frequent.
In this study, we hypothesize that medialization of tunnel exit in lateral tunnel technique would be less. We defined radiological reference points of medial meniscus root attachment and compared radiological, clinical, and arthroscopic results between medial and lateral tibial tunnels. To the best of our knowledge, this is the first study that compares medial tunnel and lateral tunnel in MMPRT pullout repair.
Materials and methods
Patient characteristics
This retrospective study was approved by our institutional review board (SCHCA 2018-06-025-002). From April 2010 to October 2017, 113 patients diagnosed with MMPRT underwent root repair. We defined MMPRT as a radial tear located within 10 mm from the posterior root insertion of the meniscus. Among these cases, 17 were repaired with the all-inside technique using FasT-fix 360TM (Smith & Nephew, Andover, Massachusetts, USA). For the remaining 96 cases, repair was performed with pullout suture technique using tibial bone tunnel.
We recommended second look arthroscopy for all patients who underwent pullout suture to remove the washer and check intraarticular status. Of patients who underwent pullout suture, 63 cases (13 males and 50 females) were able to follow-up with second look arthroscopy. Among these 63 cases, 26 belonged to medial tunnel group (MTG) while 37 cases belonged to lateral tunnel group (LTG). Patients who were younger than 18 years or older than 65 years of age were excluded from comparison. Patients with ligament injuries or other procedures such as high tibial osteotomy and cartilage repair were also excluded. Finally, 24 cases of MTG and 27 cases of LTG were included for this retrospective study.
Operative technique to create a tibial tunnel
Surgery was performed by a single knee specialist using conventional two portals (anterolateral, anteromedial). anterior cruciate ligament (ACL) tibial drilling guide (Arthrex Inc, Naples, Florida, USA) was used to create the tibial tunnel. Suture method was not distinguished.
In MTG, ACL guide pointer was inserted into the anteromedial portal to create a tunnel with an anterolateral portal as the viewing portal. We applied about 2 cm of incision to the medial side of tibia, exposed it to the cortex, and then inserted the pins to the pointed guide. Before the guide pin penetrates the far cortex, cartilage around the tunnel exit was prepared with curettage. And then we penetrate the far cortex.
The same portal was used in LTG, and tibialis anterior muscle of lateral proximal tibia was dissected about 2 cm from the tibial attach site. We exposed the tibial cortex to form a tunnel followed by placing the washer and then attaching the muscle again (Figure 1). For both MTG and LTG, position of the tibial tunnel was located at about 3 cm distal level from the joint line.

Lateral tunnel technique of MMPRT repair. (a) Guide tip is pointed through the anteromedial portal. (b) The operator then dissects the tibialis anterior muscle, creates a tunnel, places the washer, and attaches the muscle. MMPRT: medial meniscus posterior root tear.
Image and clinical evaluation
In postoperative computed tomography (CT) coronal view showing the starting point of the tibial tunnel, the angle between the tangential line of the tibial cortex and the direction of the tunnel was defined as cortex-tunnel angle (CT angle). CT angles were compared between MTG and LTG (Figure 2). At this time, the CT angle recorded the angle near the joint among two angles on the tangent line. Based on the assumption that larger difference between this angle and 90° angle would generate more fine slippage when the tibial tunnel was made, we analyzed the relationship between CT angle and slippage of the tibial tunnel.

Postoperative CT coronal view showing the starting point of the tibial tunnel, the angle between the tangential line of the tibial cortex, and the direction of the tunnel defined as the Cortex-Tunnel angle. (a) MTG and (b) LTG. CT: computed tomography; MTG: medial tunnel group; LTG: lateral tunnel group.
To evaluate the adequacy of the repair site before and after surgery, preoperative CT and postoperative CT (1-day postoperatively) were taken. To objectify the location of the tunnel before and after surgery, we measured the coronal ratio of the root attach site on coronal view of CT image. For the sake of simplicity, we called it Coronal Ratio of Root Attachment (CRORA). Original CRORA was defined as the ratio of the distance from the medial edge of the tibial plateau to the root attach site divided by the entire tibial medial–lateral (ML) width in a coronal image showing the insertion point of the root of the medial meniscus on preoperative CT (Figure 3). Osteophytes due to osteoarthritis were excluded from the measurement. On postoperative day 1 CT images, postoperative CRORA was obtained by the same method. Error between postoperative CRORA and original CRORA was calculated. The closer the calculated value (post/original CRORA) is to 1, the more the anatomical position is repaired. If it is greater than 1, the position of the tunnel exit is lateralized. If it is smaller than 1, it means that it is medialized. All measurements were measured by two orthopedic surgeons with 6 (SJ) and 5 (BW) years of experience and were familiar with radiographs of knee, and the average value measured by two measurer was used for statistics.

A coronal image showing the insertion point of the root of the medial meniscus on preoperative and postoperative CT. CRORA was defined as the ratio of the distance from the medial edge of the tibial plateau to the root attach site divided by the entire tibial ML width. (a) Original CRORA and (b) postoperative CRORA. Inset A: ML width. Inset B: the distance from medial edge of the tibial plateau to the root attach site. CT: computed tomography; CRORA: Coronal Ratio of Root Attachment; ML: medial–lateral.
Difference between MTG and LTG of this error was compared. International Knee Documentation Committee (IKDC) score and Lysholm score were also compared between MTG and LTG. Cartilage status of the medial femoral compartment of the first surgery and second look finding was also compared with International Cartilage Repair Society (ICRS) grade.
Statistical analysis
Paired t-test was used to compare MTG and LTG preoperatively and postoperatively. Clinical scores such as IKDC score and Lysholm score of both groups were compared using independent t-test. Radiological and arthroscopic changes in both groups were compared using Fisher’s exact test. All statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, Illinois, USA).
Results
The mean age of all patients included in this study was 54.5 years (range: 39–71 years). The mean age of patients in MTG was 50.4 years while that in LTG was 55.9 years. The average follow-up period to second look arthroscopy surgery was 25 months (range: 12–52.5 months). Preoperative IKDC score was 45.6 ± 11.0 in MTG, which was significantly lower (p = 0.000) than that (60.2 ± 5.8) in LTG. Preoperative Lysholm score was 60.3 ± 12.4 for MTG and 65.2 ± 10.2 for LTG. There was no significant (p = 0.276) difference in preoperative Lysholm score between the two groups (Table 1).
Demographic and preoperative clinical and radiologic characteristics of subjects in MTG and LTG.

MTG: medial tunnel group; LTG: lateral tunnel group; CI: confidence interval; IKDC: International Knee Documentation Committee.
a Student’s t-test.
b Fisher’s exact test.
c Mann–Whitney test.
Mean CT angle was 36.52 (range: 27.8°–58.6°) in MTG and 91.31 (range: 79°–98.9°) in LTG. When CT angles were compared between the two groups, the angle formed by contacts of the guide and the tibial cortex was more acute in MTG (p = 0.000) than that in LTG. The mean preoperative CRORA was 39.7 ± 2.59 in MTG and 39.41 ± 1.89 in LTG while mean postoperative CRORA was 33.8 ± 3.44 in MTG and 40.30 ± 2.58 in LTG. The mean error ratio of postoperative CRORA divided by original CRORA (post/original CRORA) was 0.86 ± 0.11 in MTG, which was significantly (p = 0.001) lower than that (1.02 ± 0.06) in LTG. This can be interpreted that there is about 14% medialization from the anatomic root attachment site in MTG, and 2% lateralization in LTG. And, in MTG, the smaller the CT angle, the smaller post/original CRORA (Figure 4).
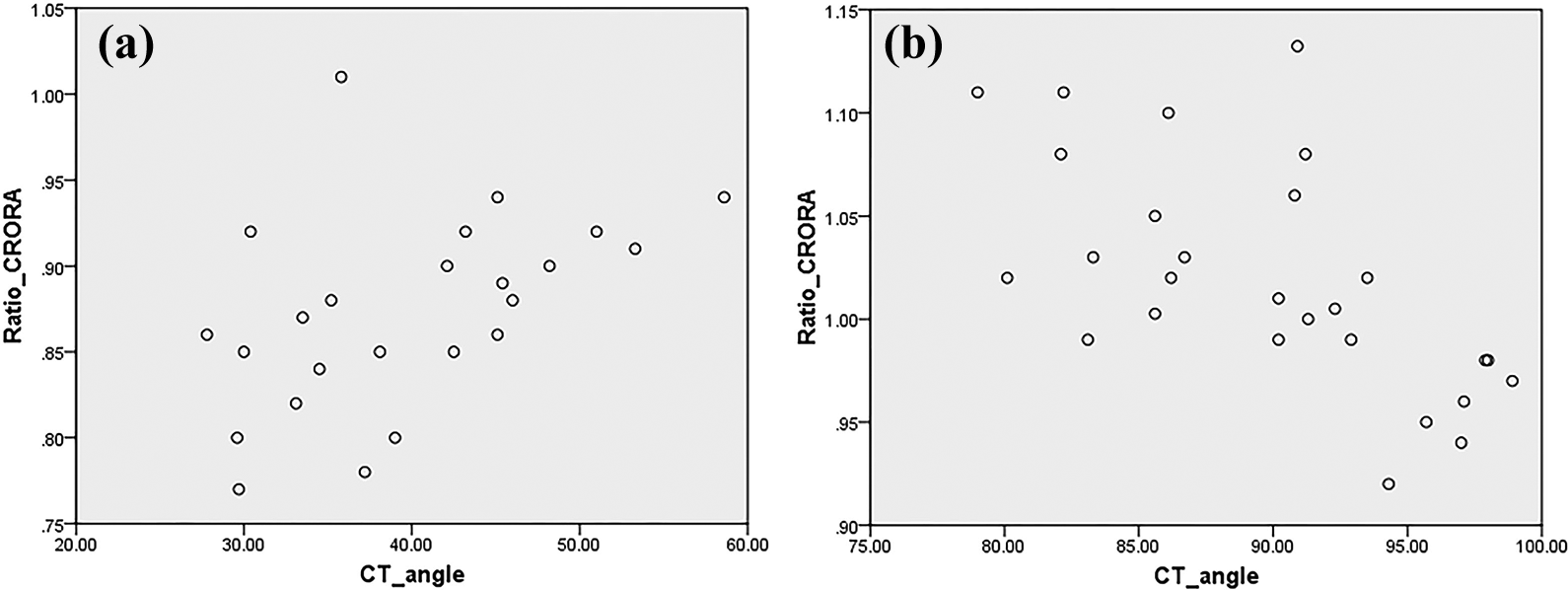
A scatter plot showing the relationship between CT angle and ratio (post/original) CRORA. (a) MTG and (b) LTG. CT angle: cortex-tunnel angle; CRORA: Coronal Ratio of Root Attachment; MTG: medial tunnel group; LTG: lateral tunnel group.
In MTG, the mean IKDC score was improved from 45.6 (range: 26.4–65.5) preoperatively to 63.6 (range: 20–96.5) postoperatively, while the mean Lysholm score was improved from 60.3 (range: 34–85) preoperatively to 76.1 (range: 33–100) postoperatively. In LTG, the mean IKDC score was improved from 60.2 (range: 51.7–72.8) preoperatively to 80.0 (range: 73.6–87.4) postoperatively while the mean Lysholm score was improved from 65.2 (range: 39–81) preoperatively to 80.3 (range: 57–91) postoperatively (Table 2). There was no statistically significant difference in changes (postoperative − preoperative) of IKDC score (p = 0.919) or Lysholom score (p = 0.777) between MTG and LTG. ICRS grade and Kellgren–Lawrence grade of medial femoral compartment cartilage in second look arthroscopic finding showed a progression pattern in both groups compared to those in the first operation. The proportion of patients showing progression in both grade scales was higher in LTG than that in MTG. However, the difference between the two groups was not statistically significant (ICRS grade, p = 0.218, Kellgren–Lawrence grade, p = 0.689) (Table 3).
Comparison of preoperative and postoperative clinical, arthroscopic, and radiologic outcomes between MTG and LTG.

MTG: medial tunnel group; LTG: lateral tunnel group; CI: confidence interval; IKDC: International Knee Documentation Committee; ICRS: International Cartilage Repair Society.
a Paired t-test.
b Fisher’s exact test.
Comparison of MTG and LTG in clinical, arthroscopic, and radiologic outcomes between MTG and LTG.

MTG: medial tunnel group; LTG: lateral tunnel group; IKDC: International Knee Documentation Committee; ICRS: International Cartilage Repair Society.
a Student’s t-test.
b Fisher’s exact test.
For second look arthroscopic findings in MTG, re-tear occurred in two cases and stitch failure with lax healing occurred in two cases. In LTG, re-tear was observed in one case. All three re-teared cases required debridement and meniscectomy. In cured cases, there was no difference in firmness between the two groups when tested with a probe. Three patients in MTG and one patient in LTG complained of mild pain at the washer insertion site at postoperative follow-up.
Discussion
Meniscus is firmly attached to the tibial plateau by anterior and posterior insertional ligament known as meniscal root. Approximately 50–70% of body weight is transmitted through the meniscus. 11 If the root of such a meniscus is transected, the continuity of the circumferential collagen fiber is cutoff. This will cause disappearance of hoop tension of the meniscus, thus impairing the function and viability of the articular cartilage and accelerating the progression to osteoarthritis. 12 The posterior root of the medial meniscus is a rigid, less mobile structure that is more susceptible to injury than other meniscal roots. 13,14 Because the posterior horn of the meniscus conveys more load than the anterior horn, especially at 90° of flexion, 15,16 root tear of the meniscus will occur, especially in people in the Orient with sedentary lifestyles. In eastern countries, such tear accounts for 20–30% of all medial meniscus tears. 17
In the past, partial meniscectomy or total meniscectomy was the main treatment for meniscal root tear, and short-term symptom relief could be expected in meniscal root tear. However, it has been reported that MMPRT is biomechanically equivalent to total meniscectomized state. It increases peak contact pressure by 25%. However, the peak contact pressure can be restored to normal level by repair. 2 However, treatment concept of meniscal root tear has changed over the years from meniscectomy to meniscal preservation. 18 Kim et al. 12 have noted that repair of MMPRT does not recover contact mechanics to normal level, although it significantly improves or delays the progression to arthritis. Thus, MMPRT repair is important. The anatomical location of the medial meniscus posterior root (MMPR) attachment site has already been identified in a quantitative study. It was found that MMPR was approximately 9.6 mm posterior and 0.7 mm lateral to the apex of the medial tibial eminence and 8.2 mm anterior to the most superior posterior cruciate ligament (PCL) tibial attachment. And, 30 mm2 is the footprint area of the main central attachment fibers of the MMPR. 19 Packer and Rodeo 20 have reported that selection of anchoring site of meniscus posterior horn is as important as surgical technique of reinsertion of the attachment and meniscal allograft transplantation. LaPrade et al. 21 have shown that nonanatomic MMPR repair can reduce tibiofemoral contact area and increase mean contact pressures. Thus, nonanatomic MMPR repair may result in progression of osteoarthritis.
We experienced a case in which the tunnel was made medial to the anchoring site during MMPRT repair operation, resulting in anatomic repair difficulties. We first used the lateral tibial tunnel to perform MMPRT repair without interference with the medial tunnel of ACL reconstruction in patients with concurrent MMPRT and ACL rupture. Subsequently, medial and lateral tunnels were alternatively used, depending on the soft tissue condition of the patient. In the process, the medial position of the tunnel seemed to be smaller with the lateral tunnel. This was the motivation for performing the current study.
The repair method of MMPRT has been developed through years of research. From 2008 to 2017, 173 papers were searched by PubMed with terms “medial meniscus root tear” and “technique.” We randomly extracted 12 articles describing the surgical procedure for pullout repair of MMPRT. Except for one study that did not mention the location of the tunnel, four studies used lateral tunnel while seven studies used medial tunnel. In early days, methods mainly introduced the lateral tunnel. However, in recent years, the medial tunnel tended to be preferred (Table 4).
Overview of surgical techniques of medial meniscus posterior root tear.

N/D: Not described; ACL: Anterior cruciate ligament; PL: Posterior lateral; MCL: Medial collateral ligament.
Post/original CRORA measured in this study indicated that repair was in an anatomical position when the value was closer to 1. In LTG, average post/original CRORA was 1.02 ± 0.06 which was relatively close to 1. However, in MTG, the average post/original CRORA was 0.86 ± 0.11, which was about 14% medialized. This means a medialization of about 9.1 mm calculated by mean ML width (65.1 ± 4.68 mm). The guide should theoretically be responsible for inserting the pin into the exact location where the guide was placed. However, there is a very small clearance between the guide and the pin because the pin must rotate without resistance in the cylindrical guide. As a result, it is often impossible to insert the guide pin in the exact position expected. To reduce this error, the guide needs to be firmly fixed, the guide tip should be sharp enough, and it should not be pushed with excessive force during the pin insertion process. Despite these efforts, there may still be a slight discrepancy between the position of the guide point and the position of the resulting pin. The reason we think for this medialization of the tunnel in MTG is as follows. First, it can be a medial slip in the slope of the tibial eminence that places the guide in place. Second, the CT angle is acute in MTG. The slip that occurs in the proximal direction during pin penetration through the tibial cortex might have resulted in the medialization of the tunnel (Figure 5).
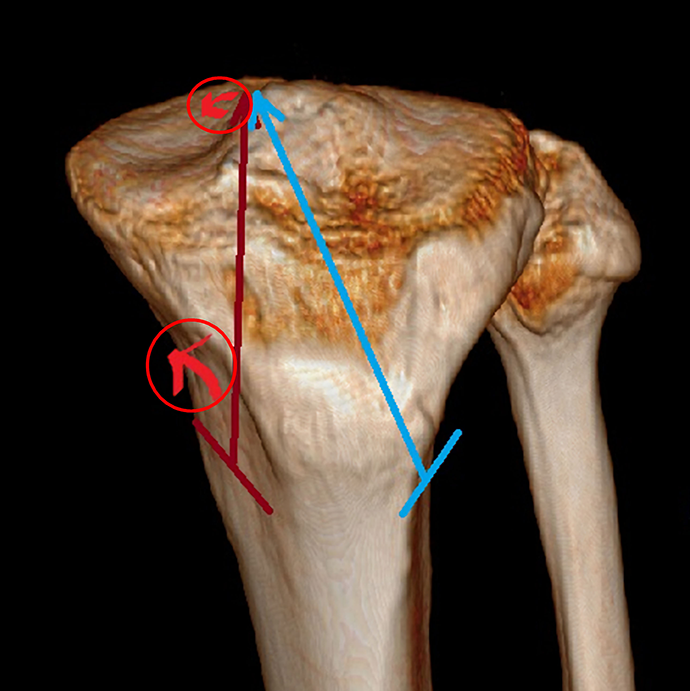
3-D CT scan image showing the reason for medialization of the tunnel in MTG. (a) Medial slip in the slope of the tibial eminence that places the guide in place. (b) The slip that occurs in the proximal direction during pin penetration through the tibial cortex, because the CT angle is acute in MTG. CT: computed tomography; MTG: medial tunnel group; CT angle: cortex-tunnel angle.
On the contrary, the reason for the low medialization in LTG is that the direction of pointing the guide is against the medial tibial eminence. Thus, a slip by the slope of eminence is small. Average CT angle was 91.31 ± 7.68° which was close to 90°. Thus, the chance of slip at the cortical entrance is small.
Starke et al. 22 have performed a biomechanical study using porcine meniscus and reported that 3-mm displacement of the meniscal attachment could cause cartilage deformation by loss of function of the meniscus that converts axial tibiofemoral load to hoop stresses. In a cadaveric study, Sekaran et al. 23 have shown that nonanatomic location of a meniscal transplant 5-mm medial to the anatomic medial meniscal posterior attachment can significantly increase the maximum pressure over all flexion angles and shift the centroid of contract area posteriorly. Thus, anatomic placement of the MMPR attachment should be considered as a top priority in restoring meniscal function. 24 The operator should be alert to medialization of the posterior root attachment.
Many efforts have been continuously made for anatomic repair of MMPRT. 24,25 Furumatsu et al. 26 have recently announced that it is possible to create a tibial tunnel at a favorite position using a new aiming guide. Our clinic performed the operation mainly using retrograde reaming device (FlipCutter; Arthrex Inc, Naples, Florida, USA). In the future, it will be interesting to compare the results of medial and lateral tunnel using this new aiming device.
Many patients complained of washer site pain in MTG because there was almost no soft tissue at the position of tibia medial border. Direct irritation might be relatively higher in MTG than that in LTG due to less muscle coverage. In LTG, patients with discomfort of leg muscles expected to dissect the muscle and locate the washer have not been observed yet.
Medial tunnel in MMPRT repair has been more widely used compared to lateral tunnel because medial procedure such as ACL reconstruction is familiar to knee arthroscopic surgeon and easy to perform. It also has an advantage in helping visualization with superficial medial collateral ligament (MCL) release through medial incision if needed. A pie-crusting release using spinal needle can provide a good working space without a medial open approach. 5 Thus, this technique can be considered for the lateral tunnel group. The lateral tunnel technique has the burden of dissecting the anterior muscle of the tibialis. However, its postoperative irritation by washer is less than the medial approach due to muscle coverage. Results of this study suggest that lateral tunnel technique can be used to make an anatomic site with fewer medial slips (Figure 6). Additionally, procedures such as medial open wedge high tibial osteotomy and ACL reconstruction can be performed without interfering with tunnel position. 27

Arthroscopic images using medial tunnel technique ((a) preoperative finding and (b) after repair) and lateral tunnel technique ((d) preoperative finding and (e) after repair). (c) In the medial tunnel technique, the tunnel was medialized (white arrow). (f) In the lateral tunnel technique, the tunnel was created in anatomic location (red arrow).
The limitation of this study was that it was non-randomized retrospective study, and it was a two-dimensional study considering only the coronal plane. In addition, it had a short-term follow-up to assess the progression of osteoarthritis. In the future, randomized controlled trial with a long-term follow-up is needed.
Conclusion
In patients with MMPRT, CRORA may provide a basis for coronal assessment of root repair position before and after surgery. And, lateral tibial tunnel technique can help anatomical repair by reducing technical error due to guide pin slip medially compared to medial tibial tunnel.
Supplemental Material
Supplemental Material, IRB_Certification_2018-06-025-002_V4.0 - Comparison of medial and lateral tibial tunnel in pullout repair of posterior root tear of medial meniscus: Radiologic, clinical, and arthroscopic outcomes
Supplemental Material, IRB_Certification_2018-06-025-002_V4.0 for Comparison of medial and lateral tibial tunnel in pullout repair of posterior root tear of medial meniscus: Radiologic, clinical, and arthroscopic outcomes by Sai-Won Kwon, Jun Bum Kim, Chang Hyun Kim, Si John Hong, Yong Cheol Hong and Byung-Woong Jang in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This retrospective study through chart review was approved by the institutional review board (SCHCA 2018-06-025-002).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Soonchunhyang University Research Fund.
Informed consent
All patients have provided informed consent for publication of the cases.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.