
Abstract
Purpose:
Bilateral total knee arthroplasty (TKA) can be performed in patients with bilateral knee arthritis. Outside of nationwide database studies, which have limitations, few studies have compared outcomes for same-day versus staged TKA. We sought to compare patient outcomes at a single tertiary referral center.
Methods:
The institutional database was queried from March 2014 to December 2017 for primary TKA. Patients undergoing bilateral procedures were stratified by same-day versus staged; length of stay (LOS), disposition, 90-day emergency department (ED) visits, and 90-day readmissions were examined through univariable and multivariable analyses.
Results:
A total of 676 patients were evaluated (113 same-day and 563 staged bilateral TKA patients) with mean age 66.0 (8.5) at first surgery and 292.1 (241.6) days between staged procedures. Same-day bilateral TKA patients were younger (p < 0.001), had lower body mass index (BMI) (p = 0.010), and had lower American Society of Anesthesiologists (ASA) scores (p = 0.030). They were more likely to have a prolonged LOS (p < 0.001) and be discharged to skilled nursing facility or rehab facility (p < 0.001). Total LOS for separate hospitalizations in staged procedures was greater than LOS for same-day bilateral TKAs (p < 0.001). There was no difference in 90-day ED visits (p = 0.623) or readmission (p = 0.286). In a multivariable model controlling for age, BMI, and ASA score, same-day bilateral TKA was not significantly associated with ED visits or readmissions.
Conclusions:
Patients undergoing same-day bilateral TKAs were more likely to be discharged to post-acute care facilities, however they did not have increased 90-day readmissions.
Introduction
Bilateral total knee arthroplasty (TKA) is a good option for patients who have failed conservative management for end-stage arthritis of bilateral knees. 1 Bilateral TKA can be performed either same-day or staged. During same-day bilateral TKA, both TKAs are performed under the same anesthetic. With staged bilateral TKA, the procedures are performed under separate anesthetics and typically months apart. There is still debate as to whether same-day TKA is safe when compared to staged TKA. 2 –10
Many studies have compared the results of staged versus same-day TKA. 2,3,5 –7,9,10 Studies have shown higher need for blood transfusion, increased rates of pulmonary embolism, cardiac complications, and mortality with same-day compared to staged TKA. 3,5,9 Other studies have shown that same-day bilateral TKA has an acceptable risk, especially in appropriately selected patients. 2,4,7,8,10 Therefore, the purpose of this study was to determine hospital length of stay (LOS), disposition, 90-day emergency department (ED) visits, and 90-day readmissions in patients receiving same-day or staged bilateral TKA. We hypothesized that patients undergoing same-day bilateral TKAs would have a longer LOS, a higher rate of ED visits and readmissions, and more discharges to a skilled nursing facility (SNF) or rehab facility (rehab).
Methods
Following institutional review board approval, the institutional database was retrospectively queried from March 2014 to December 2017 for primary TKA. Patient demographic data including age, gender, body mass index (BMI), and American Society of Anesthesiologists (ASA) score were collected, in addition to LOS (h), discharge disposition to SNF or rehab, 90-day ED visits, and 90-day readmissions. Patients undergoing bilateral procedures during the study period were then identified, and those undergoing unilateral TKA or unicompartmental knee replacement were excluded. The study cohort was then stratified by same-day bilateral versus staged bilateral TKA (Figure 1).

Flowchart of patients included.
Statistical analysis
Continuous variables including age and LOS are presented as median (lower quartile, upper quartile) and were evaluated with a Wilcoxon rank-sum test in light of their nonparametric distribution. Categorical variables including gender, ASA score (categorized as
Results
A total of 676 patients were evaluated, including 113 same-day bilateral TKAs and 563 patients undergoing staged bilateral TKA (1126 procedures) with mean age 66.0 (8.5) at the first surgery and an average of 292.1 (241.6) days between the first and second procedure. Patient demographic data between groups are shown in Table 1. Patients undergoing same-day bilateral TKAs were significantly younger (p < 0.001), had lower BMI (p = 0.010), and had lower ASA scores (p = 0.030).
Demographic data for staged versus same-day bilateral TKA.
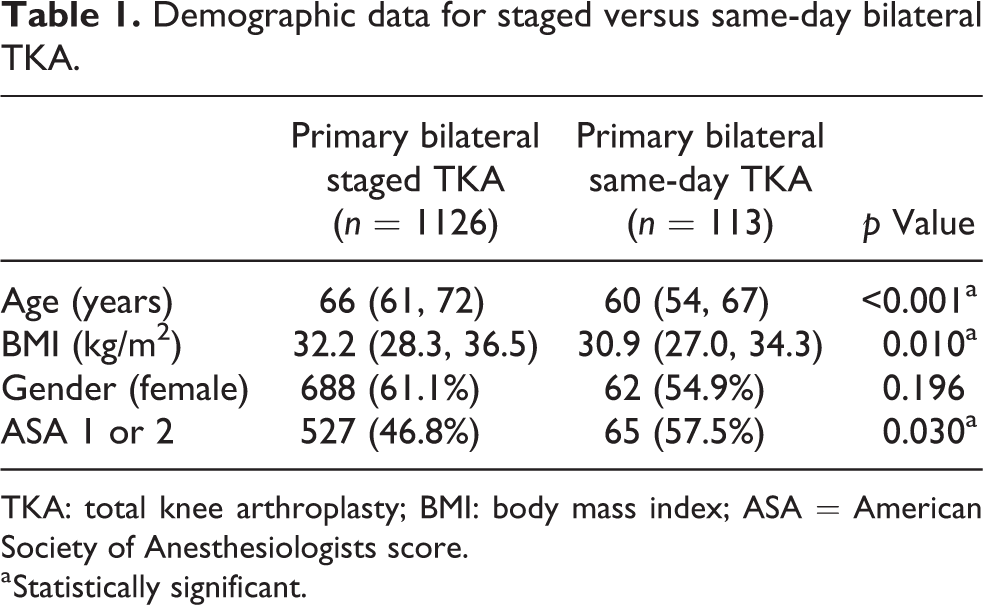
TKA: total knee arthroplasty; BMI: body mass index; ASA = American Society of Anesthesiologists score.
a Statistically significant.
Despite this, patients undergoing same-day bilateral TKA were more likely to have a prolonged LOS (p < 0.001) and be discharged to SNF or rehab (p < 0.001). Importantly, when comparing total LOS and accounting for two separate hospitalizations in staged procedures, the LOS was shorter for same-day bilateral TKAs (p < 0.001) (Table 2). Postoperatively, there was no significant difference in 90-day ED visits (p = 0.623) or readmission (p = 0.286) in univariable analysis. In a multivariable model controlling for age, BMI, and ASA score, same-day bilateral TKA was not significantly associated with 90-day return to the ED (OR 0.905, 95% CI 0.401–2.043; p = 0.810) or readmission (OR 0.453, 95% CI 0.06–3.43; p = 0.444). However, same-day bilateral surgery was significantly associated with discharge to SNF or rehab (OR 8.748, 95% CI 5.477–13.974; p < 0.001) (Figure 2).
Postoperative outcomes of same-day versus staged bilateral TKAs.

TKA: total knee arthroplasty; SNF: skilled nursing facility; LOS: length of stay; ED: emergency department.
a Statistically significant.
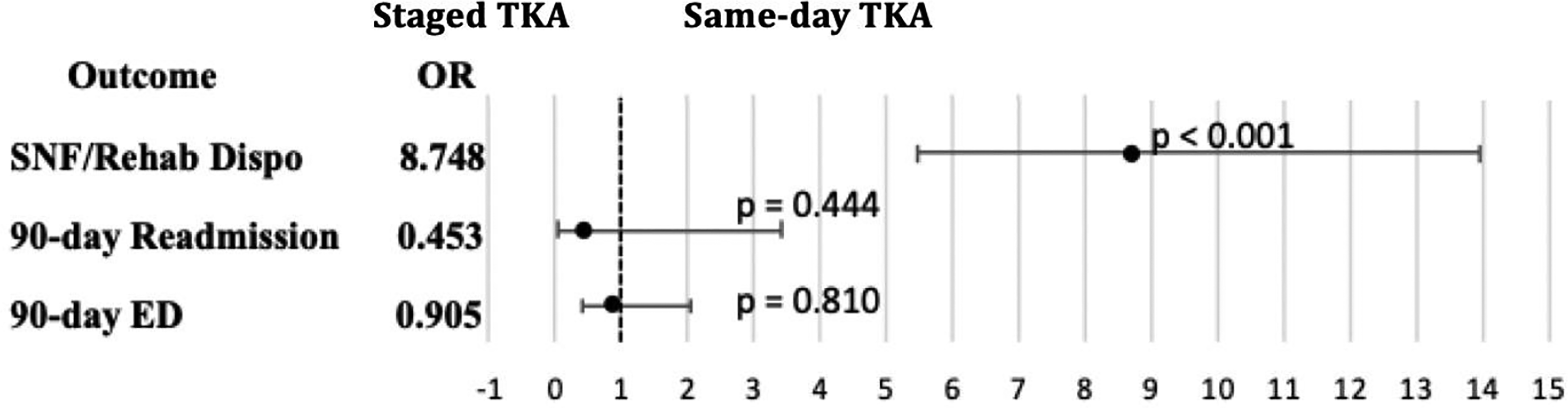
90-Day outcomes for staged versus same-day TKA. Data are presented as OR with 95% confidence intervals. TKA: total knee arthroplasty; OR: odds ratio.
Discussion
When accounting for two separate hospitalizations, we found LOS was shorter in the same-day TKA group; however, this cohort had more patients discharged to a SNF or rehab. Importantly, there was no difference between the groups in 90-day ED visits or patient readmissions. This study helps to show that same-day bilateral TKA may be safe, when compared to staged bilateral TKA.
Other studies have found that same-day bilateral TKA is associated with some increased risks compared to staged bilateral TKA. 3,5,9,11 Fu et al. 5 found that simultaneous bilateral TKA was associated with higher rates of mortality, blood transfusion, and pulmonary embolism, but lower rates of revision and infection compared to staged bilateral TKA. Bolognesi et al. 3 found in a national sample of Medicare beneficiaries that same-day TKA had a higher 90-day risk of death, myocardial infarction, and venous thromboembolism, but similar rates of revision and infection compared to staged TKA. Hart et al. 12 found that simultaneous bilateral TKA had higher odds, using a multivariable logistic regression analysis, of major complicates compared to unilateral TKA. Not all studies have found same-day bilateral TKA has an associated risk of complications.
We found that 90-day ED visits and readmissions were similar between the same-day and staged bilateral TKA groups. While the individual LOS was longer for a same-day TKA, when comparing both admissions, the LOS was longer in the staged group. Other studies have also shown that it is safe to perform same-day bilateral TKA, especially in appropriately selected patients. 2,4,7,8,10,13 It should be noted that patients in the same-day group were younger, had a lower BMI, and had a lower ASA score. Interestingly, we did perform a multivariable analysis controlling for age, BMI, and ASA score, and there was still no difference in 90-day ED visits or readmissions between the two groups. Further studies are needed to confirm our findings.
This study had several limitations. First, this was a retrospective study. There may have been events that went undetected that may be better analyzed with a prospective study. Second, this study was performed at a single academic institution with surgeons performing a high volume of joint replacements, thus these results may not be as applicable to surgeons performing a lower volume. Third, this study looked at specific outcomes. There may be complications in either group that we did not evaluate or occurred at a later point. Regardless we believe that the results provide important information for patients, surgeons, and institutions; same-day bilateral TKA may be safe to perform especially in younger, lower weight, healthier patients.
In conclusion, we found that same-day bilateral TKA did not increase 90-day ED visits or readmissions even when controlling for age, BMI, and ASA score. The combined LOS was greater in the staged group, but more patients in the same-day group were discharged to a SNF. Compared to staged bilateral TKA, same-day bilateral TKA may be safe in the short term. We still advocate that younger and healthier patients are selected for same-day bilateral TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.