
Abstract
Objectives:
Hip fractures mostly require surgical treatment and are associated with increased health-care costs and mortality rates. Patients with cirrhosis have low bone marrow density and inferior immune status which contribute to a higher fracture rate and higher surgical complication rate. This population-based study evaluated the prevalence, complication, and mortality rates due to hip fractures in cirrhotic patients.
Methods:
Taiwan National Health Insurance Research Database data were used. The study group included 117,129 patients with hip fractures diagnosed from 2004 to 2010, including 4048 patients with cirrhosis. The overall prevalence, morbidity, and mortality rates of the cirrhosis group with hip fractures were compared with the rates of a general group with hip fractures.
Results:
The cirrhosis group patients were younger than the general group patients (71.2 vs. 73.96 years, p < 0.001). The annual incidence of hip fractures in the cirrhosis and general groups was 46–54 and 7–7.5 per 10,000 person-years, respectively, with an incidence rate ratio of 6.95 (95% confidence interval 6.74–7.18). The rates of infection, urinary tract infection, and peptic ulcer disease were higher in the cirrhosis group (3.46% vs. 1.91%, 9.56% vs. 9.11%, and 8.05% vs. 3.55%, respectively; all p < 0.001). The mortality rate after hip fracture was also higher in the cirrhosis group than in the general group (within 3 months: 8.76–12.64% vs. 4.96–5.30% and within 1 year: 29.72–37.99% vs. 12.84–14.57%).
Level of Evidence:
Level III, case–control study
Keywords
Introduction
Liver cirrhosis develops when the liver parenchyma undergoes a nodular form of fibrosis arising from delayed healing in chronic liver damage. Liver disease may lead to a bone disease called hepatic osteodystrophy, 1 and the most common type is osteoporosis. Many studies have investigated how cirrhosis affects the bone tissue microstructure. 1 –5 In a previous study, loss of bone mineral density per year was associated with an increased risk of death. 6 The association between cirrhosis and osteoporosis has been well studied, and the prevalence of osteoporosis has been reported to be up to 37% in cirrhotic patients. 2,5,7,8 However, the incidence of fractures in cirrhotic patients has not been well studied. Several studies have reported an approximately twofold relative increase in the risk of fractures among patients with cirrhosis, regardless of the etiology of the liver disease, and the prevalence of overall fractures in patients with chronic liver diseases ranged from 3% to 22%. 9,10 One cohort study based on a nationwide health insurance system investigated orthopedic fractures between cirrhotic patients and the general population, and the incidence was found to be higher in cirrhotic patients. 11
Among the fracture sites, the hip (femoral neck and trochanteric area) is the most critical area that needs to be treated surgically in most cases, and hip fractures are associated with increased mortality within the first year after fractures. 12,13 Hip fractures also affect the patients’ families and community and lead to high economic and social burdens. 14 –16 In addition, increased morbidities have been reported in cirrhotic patients receiving surgery, including abdominal surgery, 17 hip and pelvic fracture surgery, 18 and knee and hip arthroplasty. 19,20 However, the association between hip fractures, morbidity, and mortality between cirrhotic patients and the general population is not well understood.
To better understand the difference between cirrhotic patients and the general population with regard to demographic data, incidence of hip fractures, and morbidity and mortality after hip fractures, we conducted this population-based study using the data from the National Health Insurance (NHI) Research Database (NHIRD) in Taiwan from 2004 to 2010. We hypothesized that the incidence of hip fractures, morbidity, and mortality would be higher in cirrhotic patients than in the general population and that clinicians should pay particular attention to cirrhotic patients with osteoporosis.
Patients and methods
Experimental procedures
The NHI program, a single-payer public insurance system for the entire population of Taiwan, was established in March 1995. The NHI program provides health care for all citizens, with a coverage rate of up to 99.8%. The program includes coverage for outpatient, inpatient, emergency, and dental care in addition to traditional Chinese medicine services and prescription drugs.
We conducted a nationwide survey of hip fractures, including femoral neck fracture and trochanteric fracture, in Taiwan from January 2004 to December 2010 using NHIRD data. This health-care database enabled the epidemiological analysis of hip fractures, because almost all patients with hip fractures in Taiwan are hospitalized to receive treatment. Data confidentiality is in accordance with the data regulations specified by the NHI Administration and National Health Research Institutes.
The inclusion criteria were patients aged 20 years or older with the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) code 820.X (hip fracture) who had received surgical treatment with certain treatment codes (78.55, 79.25, 79.35, 79.95, 81.52, 81.53, and 81.554). Information on gender, age, morbidity, and overall mortality after surgery was also recorded. The study group included patients with liver cirrhosis and was identified based on ICD-9-CM codes 571.2, 571.5, and 571.6 (alcoholic cirrhosis of the liver, cirrhosis of the liver without mention of alcohol, and biliary cirrhosis, respectively) according to diagnostic codes in outpatient and inpatient records within 3 months of fracture events. The exclusion criteria were patients with hip fracture diagnosed at age <20 years, patients who did not receive surgical treatment, and patients with pathological fractures (ICD-9-CM codes 733.14 and 733.15).
The overall and gender-specific annual hip fracture incidence rates in the general population and cirrhosis group were calculated. Overall information on cirrhotic patients was derived from the analysis of annual statistical outpatient data in NHIRD. Postoperative morbidities were identified within 3 months of surgery and included infection/sepsis/osteomyelitis, pneumonia, urinary tract infection, peptic ulcer disease, cerebral vascular accidents, and wound complications (ICD-9-CM codes 038, 730, 486, 599, 531, 434, and 998, respectively). We collected data on the diagnoses of infection, sepsis, and the surgical site deep infection of osteomyelitis according to routine codes at discharge. The total mortality rates after surgery were calculated at 3 months and 1 year as the number of patients who had died divided by the total number of hip fractures. Patient mortality was identified based on discharge codes indicating patient expiry, discharge against medical advice, and withdrawal from the NHI program. The relative frequencies of proximal femur fractures were calculated for different age groups to examine the difference between the general population and the cirrhosis group. This study was approved by the institutional review board.
Data analysis
The incidence of fractures is expressed as the number of fractures per 10,000 persons per year and was computed for each age-group (7 age groups from 20–29 years to ≥80 years with 10-year intervals). The Student’s t-test and χ2 test were used to analyze the data. Incidence rate ratios (IRRs) and confidence intervals (CIs) were computed using Poisson distribution and Student’s t-test methods. A p value less than 0.05 was considered statistically significant. All data were analyzed using SPSS (version 17.0; SPSS Inc., Chicago, Illinois, USA).
Results
Clinical characteristics of the study population
In total, 117,129 patients with hip fractures were identified from 2004 to 2010. After excluding patients based on the exclusion criteria (n = 863), the data of 112,218 patients were analyzed, of whom 4048 had cirrhosis according to ICD-9-CM codes. The average age was 71.2 years in the cirrhosis group and 73.96 years in the general group (p < 0.001). The study group included more male cirrhotic patients (50.7%), and the general group included more women (57.96%). Table 1 presents the demographic data of each group.
The demographic data of two groups.

Hip fracture incidence rates
Figure 1 shows a comparison of annual hip fracture incidence rates between the cirrhosis and general groups, which were 46–54 and 7–7.5 per 10,000 person-years in the cirrhosis and general groups, respectively. The IRR was 6.95 (95% CI 6.74–7.18) in the cirrhosis group compared with the general group. The annual hip fracture incidence rates in cirrhosis groups were much high than the general group.
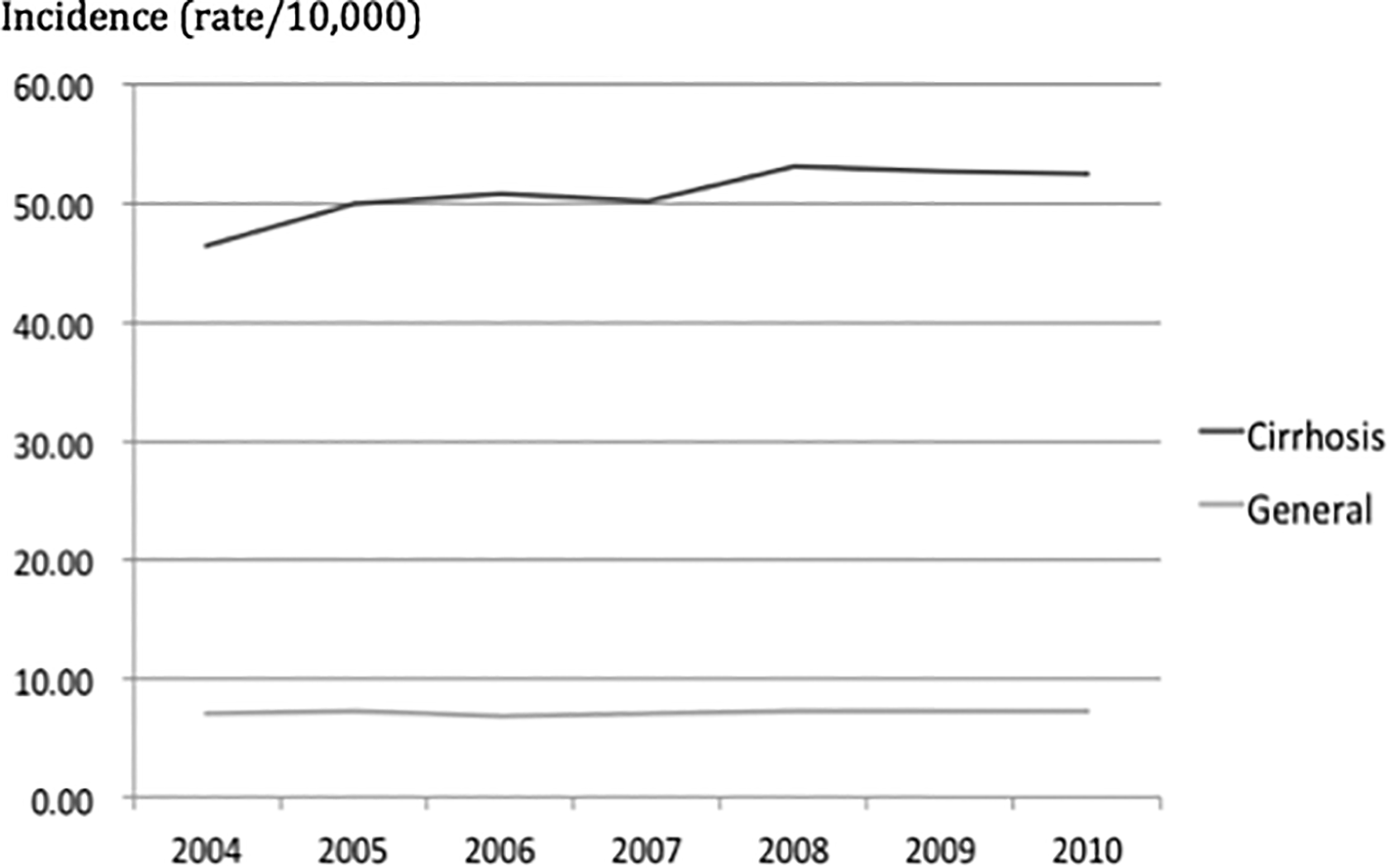
Annual hip fracture incidence rates, per 10,000 person-years. Comparison of annual hip fracture incidence rates between the general group and the cirrhosis group. Annual hip fracture incidence rates in the general and cirrhosis groups were 46–54 and 7–7.5 per 10,000 person-years, respectively. The IRR was 6.95 (95% CI 6.74–7.18) in the cirrhosis group compared with the general group. IRR: incidence rate ratio; CI: confidence interval.
Figure 2 shows a comparison of hip fracture incidence rates between the two groups by gender and age-group. The hip fracture incidence in each group increased with age. The highest incidence was found in female cirrhotic patients, followed by male cirrhotic patients, and the incidence of hip fractures was higher in male cirrhotic patients than in female patients in the general group. The IRR was 2.27 (95% CI 2.14–2.42) in female cirrhotic patients compared with male cirrhotic patients. The IRR was 9.76 (95% CI 9.33–10.20) in female cirrhotic patients compared with female patients in the general group. The IRR was 6.06 (95% CI 5.80–6.34) in male cirrhotic patients compared with male patients in the general group. Generally speaking, cirrhotic patients have a higher incidence of hip fracture than the general group, and within group, female patients have a higher incidence than male patients.

Annual hip fracture incidence rates between cirrhosis and general population by gender and age-group, per 10,000 person-years. Comparison of hip fracture incidence rates between the two groups by gender and age-group. The IRR was 2.27 (95% CI 2.14–2.42) in female cirrhotic patients compared with male cirrhotic patients. The IRR was 9.76 (95% CI 9.33–10.20) in female cirrhotic patients compared with female patients in the general group. The IRR was 6.06 (95% CI 5.80–6.34) in male cirrhotic patients compared with male patients in the general group. IRR: incidence rate ratio; CI: confidence interval.
Morbidity and mortality rates
Figure 3 shows the comparisons of postoperative morbidities between the general and cirrhosis groups within 3 months postoperatively. The incidence rates of infection/sepsis/osteomyelitis, urinary tract infection, and peptic ulcer disease were significantly higher in the cirrhosis group (3.46% vs. 1.91%, 9.56% vs. 9.11%, and 8.05% vs. 3.55%, respectively; all p < 0.001). The incidence rates of pneumonia and superficial wound complications were slightly higher in the cirrhosis group, but without statistical significance (3.66% vs. 3.00%, p = 0.448 and 0.74% vs. 0.57%, p = 0.432, respectively). The incidence of cerebral vascular accidents was significantly lower in the cirrhosis group (5.31% vs. 6.77%, p < 0.001).

Morbidities between general and cirrhosis groups within 3 months (the error bars represent the standard variation values, asterisk (*) represent significance). Comparison of morbidities between the general and cirrhosis groups within 3 months postoperatively. The incidence rates of infection/sepsis/osteomyelitis, urinary tract infection, and peptic ulcer disease were significantly higher in the cirrhosis group (3.46% vs. 1.91%, 9.56% vs. 9.11%, and 8.05% vs. 3.55%, respectively; all p < 0.001). The incidence rates of pneumonia and wound complications were slightly higher in the cirrhosis group but without statistical significance (3.66% vs. 3.00%, p = 0.448 and 0.74% vs. 0.57%, p = 0.432, respectively). The incidence of cerebral vascular accidents was significantly lower in the cirrhosis group (5.31% vs. 6.77%; p < 0.001).
Figure 4 shows the comparisons of mortality rates between the general and cirrhosis groups within 3 months postoperatively. The mortality rate within 3 months ranged from 8.76% to 12.64% in the cirrhosis group were much higher than that in the general group, from 4.96% to 5.30%, and the difference was significant (p < 0.001).
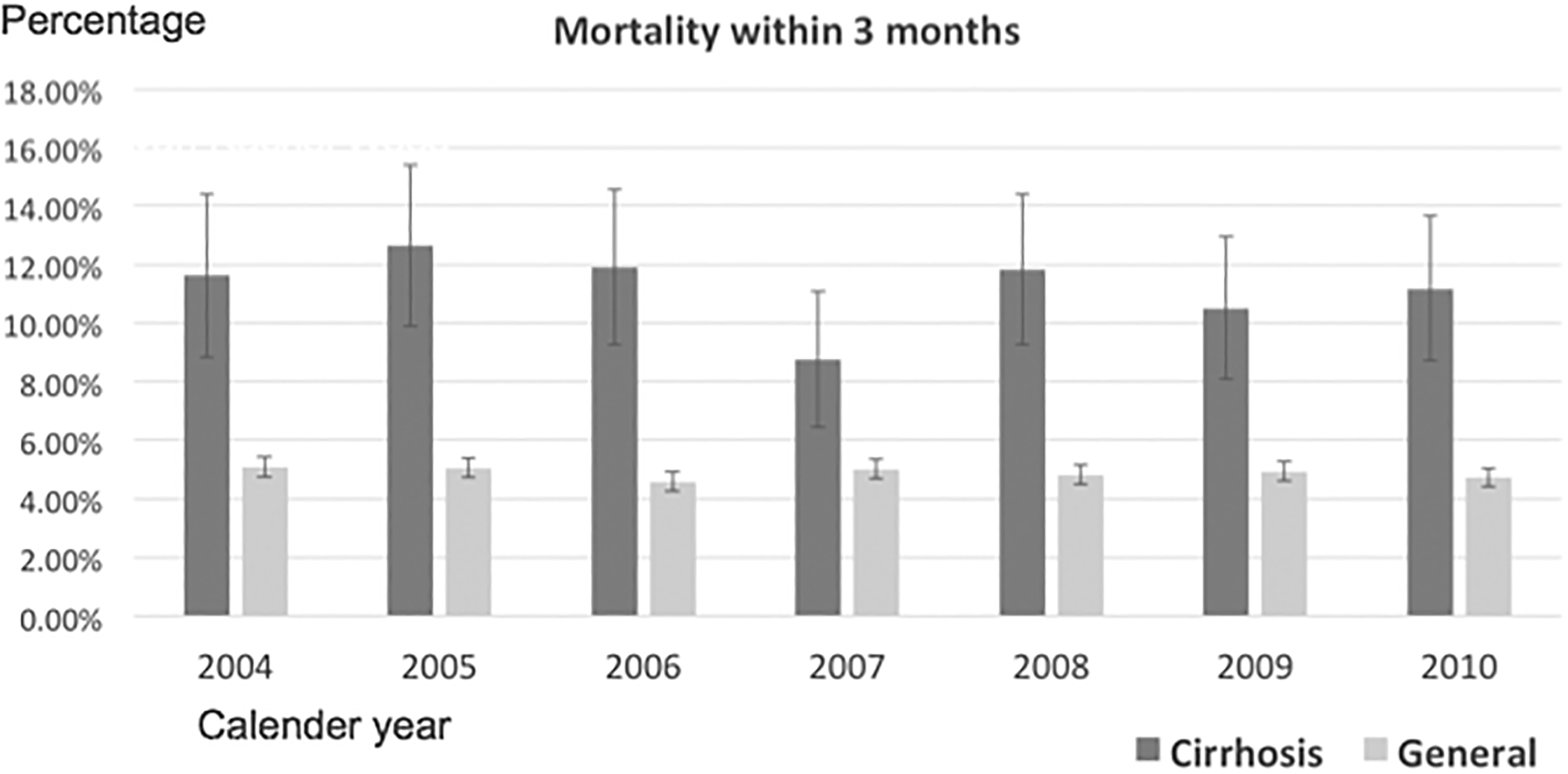
Mortality rates between the general and cirrhosis groups within 3 months. Comparison of mortality rates between the general and cirrhosis groups within 3 months postoperatively. The mortality rate within 3 months ranged from 8.76% to 12.64% in the cirrhosis group and from 4.96% to 5.30% in the general group, and the difference was significant (p < 0.001).
Figure 5 shows the comparisons of mortality rates between the general and cirrhosis groups within 1 year postoperatively. The mortality rate within 1 year ranged from 29.72% to 37.99% in the cirrhosis group were much higher than that in the general group, from 12.84% to 14.57%, and the difference was significant (p < 0.001).

Mortality rates between the general and cirrhosis groups within 1 year. Comparison of mortality rates between the general and cirrhosis groups within 1 year postoperatively. The mortality rate within 1 year ranged from 29.72% to 37.99% in the cirrhosis group and from 12.84% to 14.57% in the general group, and the difference was significant (p < 0.001).
Discussion
Metabolic bone disease occurring in individuals with chronic liver disease, known as hepatic osteodystrophy, is a potential complication of chronic hepatic disease. 15 Hepatic osteodystrophy is associated with a broad spectrum of bone diseases; the most common type is osteoporosis. 1 Osteoporosis does not directly cause disability or death but increases fracture risk. 2 In a report from Australia, each 5% increase in bone mineral density loss per year was associated with a 1.6- and 1.8-fold increase in the risk of death in men and women, respectively. 6
Among osteoporotic fractures, the hip (femoral neck and trochanteric area) is the most critical area that requires surgery in most cases, and hip fractures can reduce life expectancy. 21,22 Center et al. estimated that life expectancy is shortened by 2 years after vertebral fracture and by 11.2 years after hip fracture. 23 The risk of death after hip fracture varies over time, with the highest risk within the first few months, and the risk then diminishes gradually while remaining significantly increased for 2 years compared with the risk in the general population. 24,25 Hip fractures have been reported to lead to an overall 12–20% reduction in expected survival, with 5–20% excess mortality within the first year after the fracture, 12,13 and the risk of mortality has been reported to be as high as 25% in some case series. 26 –28 In addition to mortality, hip fractures cause functional impairment. In some studies, more than half of the patients have been reported to lose their prior level of physical function, with many patients losing their independence and requiring long-term care. 29 –31
Although the prevalence of osteoporosis is higher in cirrhotic patients than in the general population, the incidence of fractures in cirrhotic patients has not been well studied. Only one cohort study investigated the incidence of fractures in cirrhotic patients and the general population using Taiwan NHIRD data, in which the incidence of fractures was increased in cirrhotic patients compared with that in the general population, although morbidity and mortality rates after fractures were not studied. 11
In the present study, the incidence of hip fractures was much higher in cirrhotic patients than in the general population (Figure 1), and the IRR was 6.95 in the cirrhosis group compared with the general group. In a previous cohort study, the IRR between cirrhotic patients and the general population was 1.32–1.63. 11 We calculated the overall incidence of hip fractures between the cirrhosis and general groups; the annual incidence was much higher in the cirrhosis group. In age-group analysis by gender, the incidence was much higher in female cirrhotic patients. In addition, male cirrhotic patients had a higher incidence of hip fractures than female patients in the general group. Overall, a diagnosis of cirrhosis was associated with a high risk of hip fracture.
Compared with the general population, cirrhotic patients have a relatively immunocompromised status and a higher rate of surgical complications. 18,19 The most common perioperative complications were pneumonia and infection. 32 A study conducted at Mayo Clinic focusing on orthopedic surgery included 26 patients undergoing combined hip and pelvic surgeries for fractures and reported a perioperative complication rate of 53.8%; however, no data on mortality rates were provided. In our study, an increased complication rate was also noted in cirrhotic patients. The incidence of pneumonia was higher in the cirrhosis group than in the general group, but without statistical significance (p = 0.448). The second most common perioperative complication in previous studies was infection. In our study, the rate of infection/sepsis/osteomyelitis was also higher in the cirrhosis group than in the general group, with statistical significance (p < 0.001). The same result was noted for urinary tract infection and peptic ulcer disease. The incidence of wound complications was slightly higher in the cirrhosis group, but without significance (p = 0.432). The incidence of cerebral vascular accidents was significantly lower in the cirrhosis group (p < 0.001), which may be related to coagulopathy. Coagulopathy in cirrhotic patients reduces the incidence of ischemic stroke and that of overall cerebral vascular accidents.
A study reported a 30-day perioperative mortality rate of 11.6%. 18 Several studies have reported that the causes of mortality after osteoporotic fractures are cardiovascular disease, cancer, and respiratory disease; this finding is not different from that for the general population and is consistent with our findings. 23,33 –36 We analyzed the mortality rate after surgery and found that it was much higher in the cirrhosis group than in the general group within 3 months (Figure 4) and 1 year (Figure 5). Elevated incidence, morbidity, and mortality rates suggest that after patients are diagnosed with liver cirrhosis, their bone mineral density should be monitored regularly because of degraded bone mineral density and geometry at the proximal femur. 37,38 Aggressive treatment for osteoporosis should be conducted if osteoporosis is found. Antiosteoporotic drugs such as bisphosphonate could maintain bone mineral density. 39
Comorbidities such as congestive heart failure, hypertension, and diabetes mellitus may interfere with the results for cirrhotic patients and the general population. Heart disease and cirrhosis may interact during disease progression. 40,41 However, the relationship is not well understood. Cirrhosis status could cause vasodilatation with low systemic vascular resistance and high arterial compliance. However, hypertension may become normotensive during cirrhosis progression. 42 Obesity-related diabetes may worsen cirrhosis, and alcoholic cirrhosis and chronic hepatitis C may be more associated with diabetes. 43,44 However, further clinical study is required to provide a clear relationship between cirrhosis and diabetes.
In this study, we identified almost all hip fracture cases from Taiwan NHIRD. We also identified almost all mortality cases based on discharge codes indicating expiry, discharge against medical advice, and withdrawal from the NHI program. However, this study has some limitations. First, the incidence of hip fractures was unknown in 0.2% of the population not enrolled in the NHI program, which may underestimate the true hip fracture incidence. Second, for studying perioperative morbidity and mortality, the study population was included based on treatment codes, and this study excluded patients for whom surgical treatment was not needed or could not be performed. Thus, the incidence of hip fractures was likely to be underestimated. However, under the coverage of insurance, we assume that almost all patients who needed and could receive operation would be surgically treated. Third, patients in the cirrhosis group were included according to ICD-9-CM diagnosis codes in outpatient and inpatient records within 3 months of surgery, which may have excluded patients with early or mild cirrhosis. In addition, due to the coding system and daily practice, the etiology of cirrhosis was not coded after the cirrhosis diagnosis was made; the majority of cirrhosis diagnoses were provided the ICD-9-CM code 571.5 (cirrhosis of the liver without mention of alcohol). Thus, cirrhosis type could not be analyzed. However, as Taiwan is a viral hepatitis hyperendemic area, we assume that the majority of cirrhosis is caused by viral hepatitis. 45 Fourth, comorbidities within the cohort were not analyzed, including diabetes, alcohol use, and smoking. However, we believed that comorbidities were independent of cirrhosis, which would not confound the final results. Additional clinical studies providing a clear relationship between cirrhosis and comorbidity are required. As NHI data were used for analysis, alcohol use, smoking, and betel nut chewing were not identified. Fifth, the database is not generated for academic research, and coding errors may exist.
In conclusion, cirrhotic patients had higher hip fracture risks compared with the general population. Significant differences were observed in morbidities, including infections, urinary tract infection, peptic ulcer disease, and cerebral vascular accidents, between the cirrhosis and general groups. The mortality rate was higher in cirrhotic patients with hip fractures than in the general population, and the rate was up to 30% within 1 year of surgery. This result suggests that after patients are diagnosed with liver cirrhosis, their bone mineral density should be monitored regularly because of the high incidence of osteoporosis. Aggressive treatment for osteoporosis should be conducted if osteoporosis is found due to high perioperative morbidity and mortality. More attention should be paid perioperatively to cirrhotic patients with osteoporosis.
Footnotes
Authors’ note
This study is based in part on data from the National Health Insurance Research Database provided by the National Health Insurance Administration, Department of Health, and managed by the National Health Research Institutes, Taiwan. The interpretation and conclusions contained herein do not represent those of the National Health Insurance Administration, the Department of Health, or the National Health Research Institutes, Taiwan.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a research grant (CIRPD1D0032) from Chang Gung Memorial Hospital (![]() ). The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
). The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.