
Abstract
Introduction:
In the United States, chronic kidney disease (CKD) affects roughly 11% of the population or 19.2 million people. As the prevalence of CKD and demand for total joint arthroplasty (TJA) continue to rise, it is critical to assess the impact of CKD on postoperative clinical and economic outcomes.
Methods:
Discharge data from 2006 to 2011 National Inpatient Sample were used for this study. A total of 851,150 TJA patients were divided into three cohorts: group 1 included no CKD, CKD stage I, and CKD stage II; group 2 included CKD stage III and stage IV; group 3 included CKD stage V. Inverse probability of treatment weighting/propensity score weighting was used to predict outcome variables as a function of age, sex, and Elixhauser comorbidities. Patients were compared against group I for in-hospital postoperative outcomes.
Results:
Stage III/IV CKD patients undergoing primary TJA had higher odds of any complication (odds ratio (OR), 2.63; p < 0.0001), longer length of stay (LOS), and higher total charge (LOS, 4.34 vs. 3.48 days; total charge, US$56,003 vs. US$46,115; p < 0.0001) when compared to patients with no CKD/stage I or II. Similarly, stage V CKD patients undergoing primary TJA had higher odds of any complication (OR, 1.64; p < 0.0001), longer LOS, and higher total charges (LOS, 5.81 vs. 3.48 days; total charge, US$59,869 vs. US$46,115) than their counterparts with no CKD/stage I or II CKD.
Discussion:
Our results indicate that stage III, IV, or V CKD, compared with those with no CKD, stage I or II patients are at a greater risk for postoperative complications and consume more resources following TJA.
Introduction
Chronic kidney disease (CKD) is defined by abnormal measurements of the glomerular filtration rate (GFR) for a minimum of 3 months. The GFR is the rate of plasma flow filtered across the glomerular basement membrane and is often estimated by the serum creatinine level as an indicator of kidney function. Although the prevalence in the United States is roughly 11%, most patients with CKD will have stable kidney function and be more likely to die with the disease than from the disease. 1 There are five stages of CKD used to stratify patients based on the degree of renal function, which act as markers to predict the development of comorbidities to CKD. 2
Primary total joint arthroplasty (TJA) is a reliable surgical intervention for patients with degenerative disease of a joint. These procedures are recognized as being very effective at improving the quality of life through pain relief and functional improvement. 3,4 Due to the relative success and increased number of TJA performed in the United States over the last decade, it is projected that the number of TJA will continue to increase over the next decade. By the year 2030, it is predicted that the rate of primary total knee arthroplasty will increase by 85% to 1.26 million procedures, while the demand for total hip arthroplasty will grow by 71% to 635,000 procedures yearly based on data from 2000 to 2014. 5 As such, and with the skyrocketing rates, the assessment of preoperative risk factors that might impact postoperative clinical and economic outcomes has become more critical. 6
CKD most often presents in patients with diabetes and hypertension, while age itself is a key predictor. 1,2,7 While the disease process is specific to the kidneys, patients with CKD often present with a plethora of medical comorbidities, such as anemia, hyperlipidemia, osteodystrophy, and cardiovascular risk. This combination of comorbidities may manifest itself in a patient needing TJA, making it extremely important for orthopedic surgeons to understand the impact that CKD may have on postoperative outcomes. 8
Previous research has shown the impact of CKD on surgical outcomes in the setting of coronary bypass, abdominal surgery, and pancreatic resections. For these procedures, the researchers concluded that greater impairment in renal function showed a marked increase in postoperative mortality. As such, the assessment of renal function should be part of the preoperative risk assessment and prediction models when selecting suitable candidates for these surgeries. 9 –11
The recommendations from coronary bypass, abdominal surgery, and pancreatic resections suggest the importance of investigating the effect that CKD will have on postoperative outcomes following TJA. Currently, research looking at this topic focuses on the impact that end-stage renal disease (ESRD; stages IV and V) will have on postoperative outcomes while negating those with less advanced renal disease. 12,13 In each of these studies, similar results were found: patients with CKD undergoing elective orthopedic procedures are at increased risk of prolonged morbidity and hospital stay.
All of this information point to the need to investigate CKD across all of the stages and not just focus on a small subset of individuals with advanced CKD (ESRD). By conducting a retrospective observational study based off a national dataset, this article aims at further understanding the clinical and economic impact of preoperative CKD on postoperative outcomes following TJA.
Methods
Materials
Discharge data from 2006 to 2011 National Inpatient Sample (NIS) were used for this study. The NIS is a database developed by the Health care Cost and Utilization Project and offers a stratified representation that approximates 20% of all community hospitals. Discharges are recorded annually, and the data can be weighted to produce statistically valid national estimates. This tool allows researchers to investigate health care-related costs, medical practice trends, and perioperative outcomes at a national level. The NIS database uses the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) codes to standardize the reporting of diagnoses, procedures, and complications. 14
Data collection
ICD-9-CM codes were used to identify 851,150 patients aged over 55 who underwent primary TJA of either the knee (81.51) or hip (81.54). The TJA group was further stratified into three groups: group 1 included no CKD, stage I, and stage II; group 2 included CKD stage III and stage IV; and group 3 included CKD stage V.
Methodology
The methodology utilized was inverse probability of treatment weighting (IPTW)/propensity score weighting. This technique is nearly identical to standard matching methodologies but had a few key advantages for our study design. Because this study had three levels to the outcome variable, matching would be complicated. In addition, IPTW prevents the removal of patients who do not match, as the removal of these patients can negatively impact the generalizability of results in the United States population as a whole.
Data analysis
A logistic regression model was built to predict the outcome variable as a function of age, sex, and Elixhauser comorbidities. The predicted probabilities were obtained from the multinomial logistic regression. From these predicted probabilities, propensity scores were calculated. The discharge weight and the IPTW were combined into a final weight. The final weight was calculated as discharge weight × IPTW. An IPTW-weighted model was run, and the outcome was predicted as a function of the three computed levels of CKD.
Results
A total 851,150 patients met inclusion criteria for comparative analysis. No significant difference was noted in baseline characteristics between cohorts (Table 1). Our analysis showed that CKD, stage III and above, is associated with a variety of postoperative complications when compared with CKD stage I/II or no CKD. All patients with CKD stage III and above have increased risk of postoperative genitourinary complications and anemia, as well as longer LOS, greater total charge, and greater odds of being discharged to a rehab facility rather than discharged home following a TJA. Patients with CKD stage III/IV have a 2.20-fold greater odds of a genitourinary complication and a 2.85-fold greater odds of postoperative anemia when compared to patients with CKD stage I/II or no CKD. In addition, patients with CKD stage III/IV stay on average 0.86 days longer and have a total charge of US$9,888 more. This leads to a 15% lower odds of being discharged home and a 17% greater odds of being discharged to a rehab facility compared to their CKD stage I/II and no CKD counterparts. Similarly, CKD stage V confers greater postoperative risk as patients are at a 2.53-fold greater odds of a genitourinary complication and a 1.51-fold greater odds of postoperative anemia compared to stage I/II and no CKD patients (Table 2, Figures 1 and 2).
Primary TJA demographics and comorbidities.a

a Demographics and comorbidities for each of the three groups. No significant difference was noted in the baseline characteristics between groups.
In-hospital postoperative outcomes after primary TJA.a

OR: odds ratio; TJA: total joint arthroplasty.
a A comparison of the in-hospital postoperative outcomes for each of the three groups is found in the first three columns. Then, the stage III/IV and stage V were compared to group I and an OR was calculated. Statistical significance at p < 0.05.
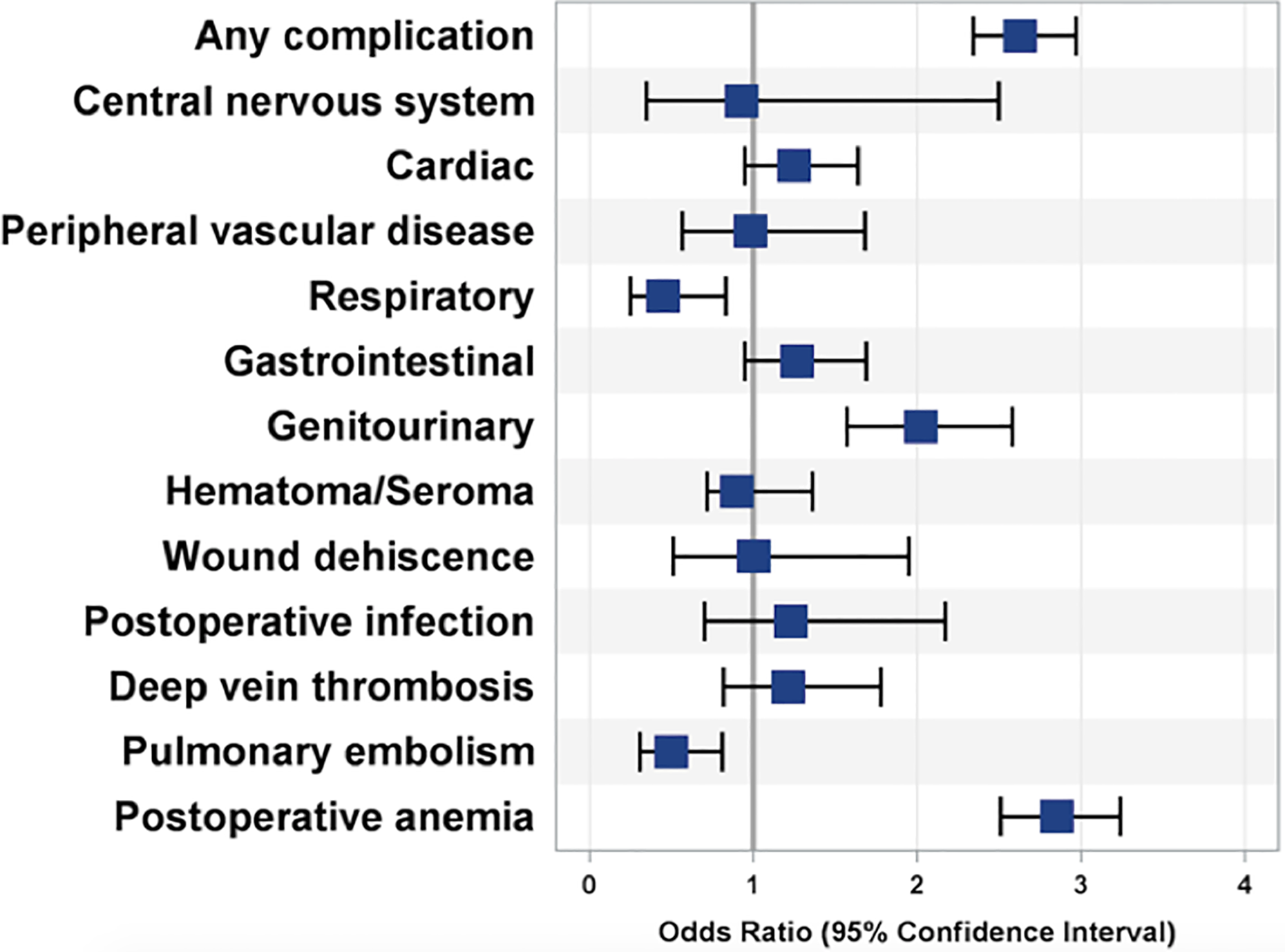
Complications for stage III/IV compared to no CKD/stage I/II CKD. OR for stage III/IV compared to no CKD/stage I/stage II CKD on a forest plot. OR >1 suggests greater odds of that complication for patients with stage III/IV, while OR <1 suggests less odds of that complication. Those that cross the line at 1 are not considered statistically significant (p < 0.05). OR: odds ratio; CKD: chronic kidney disease.

Complications for stage V compared to no CKD/stage I/II CKD. OR for stage V compared to no CKD/stage I/stage II CKD on a forest plot. OR >1 suggest greater odds of that complication for patients with Stage V, while OR <1 suggests less odds of that complication. Those that cross the line at 1 are not considered statistically significant (p < 0.05). OR: odds ratio; CKD: chronic kidney disease.
In addition, resource utilization was greater among these two groups when compared with individuals in group 1 (no CKD, stage I, and stage II). These increased risks are associated with a 2.33-day longer LOS and a total additional charge of US$13,754. Patients with CKD stage V have a 56% lower odds of being discharged home and are 2.23-fold greater odds to be discharged to a rehab facility compared to CKD stage I/II or no CKD (Table 3).
Resource outcomes after primary TJA.a

TJA: total joint arthroplasty; OR: odds ratio.
a A comparison of the absolute resource utilization for each of the three groups is found in the first three columns. Then, the stage III/IV and stage V were compared to group I and an OR was calculated. Statistical significance at p < 0.05.
Discussion
CKD is a chronic condition with continual worsening of kidney function leading to kidney failure and eventually end-stage renal disease (ESRD). However, the progression of the disease is also associated with numerous comorbidities, such as anemia, hyperlipidemia, and increased cardiovascular risk. This combination of worsening kidney function and other comorbidities is extremely important for orthopedic surgeons as it is predictive of prolonged hospital stay and increased mortality following TJA surgery. Based on our study, patient with stage III/IV and stage V CKD undergoing primary TJA had higher odds of any complications, longer LOS, and higher total charges when compared to their counterparts with no CKD/stage I or II CKD. As such, it is vital that orthopedic surgeons include the assessment of kidney function and other comorbidities as part of the preoperative risk assessment when selecting suitable candidates for TJA surgeries to optimize postoperative outcomes.
Our study design provides a unique approach to assessing the impact of CKD on TJA. Many studies have previously investigated the outcomes of patients on dialysis and the impact of ESRD on postoperative outcomes. Patients with ESRD infrequently undergo elective TJA due to their multiple preoperative comorbidities that causes them to experience more postoperative complications and lower functional outcomes. 12,15 In addition to an increase in-hospital mortality, these patients are at greater risk of surgical site infections and wound complications, increased risk of transfusions due to postoperative anemia, and deep vein thrombosis (DVT). Although our study did not focus solely on ESRD, we were able to see the increased odds of postoperative anemia and genitourinary complications, as have been noted in other studies of CKD stage V patients.
Several studies analyzed particular subsets within the CKD spectrum, and many found that patients with CKD stage III or worse had worse postoperative outcomes, and increased LOS and total cost. Ackland et al. noted that reduced GFR led to increased cardiovascular risk and delayed discharge from the hospital, especially with a GFR of <50. 13 These conclusions are supported by the results of our study.
When examining postoperative complications in patients with CKD, Li et al. found an increased risk in DVT for patients undergoing TJA. 16 This finding was supported by Tan et al. who further stratified CKD patients according to stage and still noted a significant risk of DVT. 17 However, Miric et al. reported a nonsignificant risk of DVT in patients with CKD. 18 In our study, the incidence of DVT following TJA in patients with CKD stage III, IV, or V was not significantly higher compared to group I. Interestingly, we noted a statistically significant lower incidence of pulmonary embolism (PE) in cohort 2 when compared to cohort 1. As this study utilizes a data set that strictly includes data points from the in-patient encounter and lacks follow-up data, the aforementioned findings might be misrepresented, as DVT and PE might occur at a later stage, when the patients are discharged home. In addition, the study used data from a plethora of institutions across the nation from 2006 to 2011. Although this allows for a better understanding of outcomes at a national level, the lack of standardization when it comes to postoperative anticoagulation prophylaxis might in part contribute to the DVT and PE findings.
One of the limitations of this study was our utilization of the NIS database. Although this database offers an immense amount of information about clinical and economic outcomes, it is important to remember that it is a sample of 20% of community hospitals within the United States. 14 Therefore, the data analysis may not be generalizable to the entire population of patients in the United States with CKD. In addition, the database does not allow for assessment of postoperative outcomes at a longer follow-up duration, as the data point for a specific encounter ends at the time of discharge from the in-hospital setting. This could lead to misrepresentation of postoperative complications, as patients being readmitted for the collected complications will not be included in the database. Although limited by its technical and inherent flaws, the NIS is a great tool for observational epidemiologic studies and can provide several general trends to guide future research.
As the number of TJA procedures performed annually continues to rise, it is critical to understand risks for postoperative complications associated with various preoperative comorbidities and to design standardized clinical pathways to optimize patients preoperatively to ensure optimal outcomes following the procedure. In conducting this study, it is clear that patients with CKD, especially stages III, IV, and V are at an increased risk of developing in-hospital postoperative complications, while also utilizing more resources and staying in the hospital for longer periods of time. To improve postoperative outcomes in this patient population, it will become critical for orthopedic surgeons and others recommending these individuals for TJA surgeries to focus on medically optimizing these patients preoperatively. Future studies should not only consider looking at a more representative population sample but also looking at the impact of specific preoperative optimization measures on postoperative outcomes. Together, these studies may help to reduce the health-care utilization that this patient population requires as well as confirm or dispute the results generated in this study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.