
Abstract
Purpose:
Hamstrings surgical lengthening (HSL) has been frequently used for the treatment of flexed knee gait in cerebral palsy; however, recurrence of knee flexion deformity (KFD) and increase of anterior pelvic tilt (APT) were reported in a long-term follow-up.
Research question:
The aim of this study was to compare semitendinosus transfer to distal femur (STTX) and semitendinosus surgical lengthening (STL) regarding the reduction of KFD and the increase of APT after flexed knee gait treatment.
Methods:
One hundred and eleven patients were evaluated and they were divided into two groups according to surgical procedures at knees: group A (65 patients/130 knees), including patients who received medial HSL as part of multilevel approach; group B (46 patients/92 knees), represented by patients who underwent orthopedic surgery including an STTX instead of STL.
Results:
Fixed knee flexion deformity (FKFD) decreased only in group B (from 6.79° to 2.96°, p < 0.001) after intervention. In kinematics, APT increased from 16.38° to 19.03° in group A (p = 0.003), while group B also increased from 15.26° to 20.59° (p < 0.001). The minimum knee flexion in stance phase (MKFS) reduced from 25.34° to 21.65° (p = 0.016) in group A and from 31° to 19.57° (p < 0.001) in group B. In the comparison between groups A and B, the increase of APT (p = 0.028) and reduction of FKFD (p < 0.001), popliteal angle (p = 0.001), bilateral popliteal angle (p = 0.003) and MKFS (p = 0.006) were higher after STTX than STL.
Conclusion:
In the present study, patients who received STTX exhibited more improvement of knee extension at clinical examination and during gait than those who underwent to STL; however, STTX was not effective to prevent the increase of APT after flexed knee gait treatment.
Introduction
The knee flexion deformity (KFD) is frequently observed in patients with spastic cerebral palsy (CP) and it can compromise standing and gait. 1 The spasticity and progressive contracture of hamstrings are one of the causes of KFD and crouch gait in CP. 2,3
Consequently, surgical lengthening of the hamstrings is the present standard procedure for the correction of KFD in CP, with satisfactory short-term outcomes. However, previous reports showed deterioration of the results in a long-term follow-up and resultantly, the weakness of hamstrings as hip extensors were implicated in it. 2
In addition to this, Zwick et al. described, in 2002, an increase of anterior pelvic tilt (APT) after this procedure, as a result of the loss of hip extensors strength. 4 Moreover, hamstrings weakness has been considered a potential cause of the increase in APT by many authors. 5 –8
Ma et al. (2006) described the semitendinosus transfer to distal femur (STTX) to preserve hip extensor power after the correction of KFD in CP. They reported an improvement of knee extension in the stance after STTX, with no deterioration of APT, in a case series composed of 19 patients with CP. 9 Nevertheless, the comparison between STTX and semitendinosus surgical lengthening (STL) was not performed.
Thus, the purpose of this study was to compare STTX and STL regarding the reduction of KFD and the increase of APT after flexed knee gait treatment in patients with CP.
Materials and methods
Subjects
This was a retrospective cohort study approved by the local ethics committee (approval number 3.353.051). A search was done at gait laboratory database considering the inclusion criteria: (1) diagnosis of spastic diplegic CP without previous hamstrings surgical lengthening (HSL), (2) Gross Motor Function Classification System (GMFCS) levels I–III, (3) fixed knee flexion deformity (FKFD) lower than 15° in the preoperative physical examination, (4) minimum knee flexion in stance phase (MKFS) greater than 10° in the preoperative gait analysis, (5) patients undergone gracilis and semimembranosus surgical lengthening with concomitant STTX or STL bilaterally, and (6) preoperative and postoperative gait analyses with minimum follow-up time of 24 months. Patients with concomitant distal femur extension osteotomy were not included in the study.
We decided to not include in the study patients with the previous HSL because the soft tissue scar and fibrosis could compromise the STTX. In addition to this, Chang et al. and Rethlefsen et al. described that primary and repeated HSL do not have similar outcomes. The revision of HSL was related to the modest improvement of knee extension in stance phase and increase of APT. 10,11
A total of 111 patients were considered for the study. They were divided into two groups according to procedures performed on knees: group A (65 patients/130 knees), including patients who received STL combined to gracilis and semimembranosus surgical lengthening; group B (46 patients/92 knees), represented by patients who underwent orthopedic surgery including the STTX instead of STL.
The indications for surgical treatment did not differ between groups A and B. Four different pediatric orthopedic surgeons performed all the procedures. Two of them were in charge of group A surgical treatment and choose STL instead of STTX. Their rationale was because STL was a faster and less demanding procedure than STTX and the postoperative results were similar despite the technique applied.
Conversely, the two other pediatric orthopedic surgeons performed the surgical procedures at patients from group B. Their preference for STTX was justified on the hypothesis that the procedure could preserve some power of hip extensors. The described scenario was very convenient for a retrospective study comparing these two different approaches at semitendinosus.
Surgical technique
Surgical procedures were performed with patients in prone position. Subjects from group A received an intramuscular tenotomy on gracilis, a Z lengthening on semitendinosus, and fractional lengthening on semimembranosus. The approach in group B was similar to group A regarding gracilis and semimembranosus; however, the semitendinosus was transferred to adductor tubercle at distal femur. STTX was carried out after the release of semitendinosus close to its insertion at tibia and the mobilization of it proximally. The insertion of adductor magnus at distal femur was identified by palpation. A right-angle clamp was used to pass the distal extremity of the released semitendinosus under the insertion of adductor magnus at adductor tubercle and number 1 Ethibond (Ethicon Inc., Sumerville, New Jersey, USA) sutures were applied under slight tension. The semitendinosus was sutured to adductors magnus tendon and to itself.
The postoperative protocol was the same for the two groups and the correction goal was to reach full knee passive extension at the time of cast removal. After surgery, a longleg cast was used for 4 weeks with knees in full extension in patients who did not exhibit residual FKFD after surgery. For those with residual FKFD after surgical procedures, a serial casting was applied 1 week after hospital discharge to achieve full extension and after that the immobilization was used for more 3 weeks. At the time of cast removal, all patients analyzed had full passive knee extension. Subsequently, knee immobilizers were prescribed for night use for 12 months. The rehabilitation started after cast removal and discharged when patients have attained functional and independence levels as present before surgical intervention.
Clinical assessment and gait analysis
Clinical assessments included the examination of lower limbs passive joint range of motion of using a calibrated goniometer. All of the patients were evaluated by a senior physical therapist and a pediatric orthopedic surgeon, who both have had more than 10 years of experience in gait analysis and management of neuromuscular conditions.
Kinematic data had previously been collected using reflective markers that are strategically placed on specific anatomical landmarks on each participant, as described by Kadaba et al. 12 An eight-camera Qualisys OQUS300 system (500 Hz) [Qualisys AB, Gothenburg Sweden] was utilized for movement capture. Patients were instructed to walk barefooted in a self-selected speed through an 8-m walkway (26 feet). A minimum of six gait cycles for each assessed lower limb was collected; for consistency in evaluation, a representative trial was also selected for analysis. The data were processed using the software Vicon Clinical Manager (VCM, Oxford Metrics, Oxford, UK), according to the technique described by Davis. 13
Parameters analyzed and statistics
Demographic, clinical, and dynamic parameters were analyzed, and the results compared between groups A and B, before and after intervention. For comparison of age at surgery, follow-up time, and clinical and kinematic data changes between groups A and B, the Mann–Witney test was applied. The χ2 test was used to compare the gender-level and GMFCS-level distributions. Two proportions equality test was applied for the comparison of surgical procedures performed at the same session of KFD correction between both groups. Finally, the comparison between quantitative preoperative and postoperative variables intragroups was done using the Wilcoxon test. The level of significance was set at p < 0.05 for all statistical tests. 14
Results
Gender and GMFCS distribution, and surgical procedures performed in the same surgical session of KFD correction did not exhibit difference between groups A and B. Mean age at surgery was 9.4 years (from 4.7 to 14.6 years) in group A and 10.6 years (from 4.7 to 18.7 years) in group B (p = 0.008; Tables 1 and 2).
Demographic data in groups A and B.a
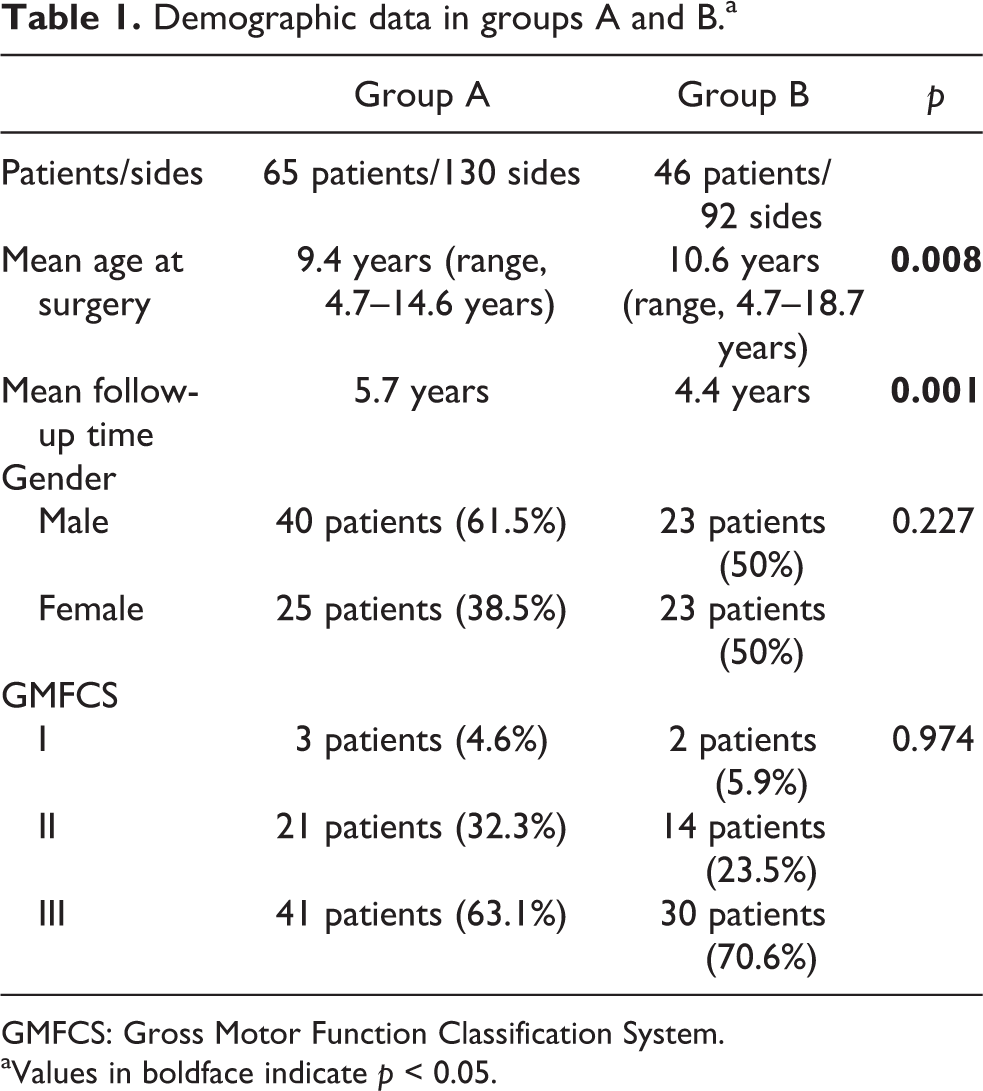
GMFCS: Gross Motor Function Classification System.
aValues in boldface indicate p < 0.05.
Surgical procedures performed in the same session of KFD correction in groups A and B.

n: number of procedures; FDO: femoral derotation osteotomy; PTS: patellar tendon shortening; RFTX: rectus femoris distal transfer; RFL: rectus femoris intramuscular lengthening; VARUS FOOT: varus foot surgical correction; MFP: Majestro–Frost procedure; POB: psoas lengthening over the pelvic brim; HAL: hip adductors surgical lengthening; GSL: gastrocnemius and soleous intramuscular lengthening; LCL: foot lateral column lengthening; TO: tibial derotation osteotomy; KFD: knee flexion deformity.
During analysis of the clinical parameters, it was observed that unilateral and bilateral popliteal angles showed a significant decrease in both groups after surgery, while reduction of FKFD occurred only in group B (from 6.79° to 2.96°, p < 0.001; Table 3).
Clinical parameters before and after intervention in groups A and B.a

A: group A; B: group B; Pre: preoperative; Post: postoperative; SD: standard deviation; N: number of lower limbs.
aValues in boldface indicate p < 0.05.
In the kinematics, the mean APT increased from 16.38° to 19.03° for group A (p = 0.003), while group B also increased from 15.26° to 20.59° (p < 0.001). The minimum hip flexion in stance (MHFS) and peak ankle dorsiflexion in stance (PADS) also increased in the two groups after intervention; however, MKFS reduced from 25.34° to 21.65° (p = 0.016) in group A and from 31° to 19.57° (p < 0.001) in group B (Table 4).
Kinematic parameters before and after intervention in groups A and B.a

A: group A; B: group B; Pre: preoperative; Post: postoperative; SD: standard deviation; N: number of lower limbs.
aValues in boldface indicate p < 0.05.
The comparison of the results of treatment between groups showed that the reduction of FKFD (p < 0.001), unilateral popliteal angle (p = 0.001), bilateral popliteal angle (p = 0.003), and MKFS (p = 0.006) were more significant in group B rather than group A. On the other hand, the increase in APT was also significantly higher in group B (p = 0.028; Table 5).
Comparison of the changes at clinical and kinematic parameters intergroups A and B after treatment.a

A: group A; B: group B; −: decrease; SD: standard deviation; N: number of lower limbs.
aValues in boldface indicate p < 0.05.
Discussion
HSL has been considered the standard procedure for the correction of KFD in CP. However, the outcomes can deteriorate in a long-term follow-up. 2 Zwick et al. described an increase of APT after HSL. This result could be explained by the loss of hip extensors strength. 4 The weakness of hip extensors combined with an increase of APT and lumbar lordosis are potential causes for recurrence of knee flexion during stance phase in gait and deterioration of the early outcomes of HSL. 2
One of the purposes of STTX is to preserve the strength of semitendinosus as a hip extensor and to prevent the increase of APT postoperatively. In 2006, Ma et al. reported an improvement at knee extension during physical examination and stance phase in gait in a series of cases: out of which 19 patients with CP had undergone gracilis and semimembranosus surgical lengthening, combined with STTX. In addition, they mentioned no deterioration of APT after a mean follow-up time of 25 months. 9
In another report by Sung et al., they analyzed a group of patients who had received single event multilevel surgery in lower limbs, including STTX; after a long-term follow-up, there was no increase in APT observed. 15 However, the comparison between STTX and STL regarding its effects at clinical and kinematic parameters was not done in these studies.
On the other hand, Dreher et al. reported an increase of APT after the conversion of biarticular to monoarticular muscles and after musculotendinous lengthening in spastic diplegic CP in a long-term follow-up. 16
Feng et al. in 2012 and De Mattos et al. in 2014 compared the results of the transfer of semitendinosus and gracilis to distal femur to the lengthening of medial and lateral hamstrings. The improvement of knee extension in stance phase and the increase of APT were noted in both studies, irrespective of the techniques applied for the correction of KFD. The authors believed that the inclusion of biceps femoris in the treatment plan in majority of subjects analyzed could be a possible explanation for the raise of APT after surgery. 17,18 Feng et al. mentioned that an increase of APT is inevitable when crouch gait is corrected, since the oblique femur becomes more vertical during stance, thereby rotating the pelvis into more of an anterior tilt. 17
In the present study, comparison between STTX and STL using clinical and kinematic parameters was carried out. The increase of APT was observed in both groups after intervention. The impact of STTX in preventing an increase of APT still controversial. The determination of the position of the pelvis in sagittal plane seems to be determined by multiple factors, including posture changes after KFD correction and crouch gait treatment; since the increase of APT was described previously after distal femoral extension osteotomy and patellar tendon advancement. 19,20 In addition to this, the surgical lengthening performed at gracilis and semimembranosus in all patients of this study could be related with some degree of hip extensors weakness and also be a cause of the increase of APT in long-term follow-up.
In 2006, Arnold et al. reported that the examination of the muscle-tendon lengths and velocities allows individuals who walk with abnormally short or slow hamstrings to be distinguished from those who do not and thus may help to identify patients who are at risk for unsatisfactory postsurgical changes in knee extension or APT. 7 As a consequence of it, we believe that the use of muscle-tendon lengths modeling prior STTX or STL can be helpful in order to predict the results at APT.
Moreover, Rutz et al. described in 2010 the preoperative botulinum toxin test injections before muscle lengthening in CP to filtering out patients with risk of deterioration after soft tissue procedures. 21 The authors observed that the use of the botulinum toxin test before surgery reduced the percentage of patients with deterioration of the function after surgical muscle lengthening from 18% to 0%. We also believe that this test could be applied before medial hamstrings procedures to identify patients with higher risk of increase APT after intervention.
Secondly, we also observed in the present study a more significant improvement of knee extension at clinical examination and during stance phase in patients who received STTX. We believe that STTX can protect the knee joint from the effects of semitendinosus shortening during growth. After the transfer, the insertion of semitendinosus muscle moved from proximal tibia to distal femur, converting it to a single joint muscle. According to Graham and Selber, the development of contractures can occur during growth in patients with spastic CP and biarticular muscles are more susceptible to it. 22
However, it is important to state that the spasticity or contracture of hamstrings is just one possible reason for knee flexion recurrence and the other causes for recurrent crouch gait must be addressed, like quadriceps and triceps surae weakness, and lever arm dysfunction.
In the present study, the increase of ankle dorsiflexion in stance phase after treatment was observed in both groups and there was no difference at intergroups comparison. In addition to this, the two groups also matched regarding surgical procedures received in the same surgical session of KFD correction. None of patients received distal femur extension osteotomy and the patellar tendon shortening prevalence was also similar at both groups. Considering all of this information together, we believe that the other factors related to recurrent crouch gait (quadriceps and triceps surae weakness, and lever arm dysfunction) had similar effects in the results at both groups.
However, the study has limitations. The age at surgery was higher and the follow-up time was lower in the group composed by patients who received STTX instead of STL. These data might suggest that patients who underwent STL were more susceptible to have a recurrence of KFD because they were treated earlier and they were followed for a longer time than those who received STTX, which could deteriorate their results over the time. Although, despite the significant statistical difference between groups regarding age at surgery and follow-up time, the mean values were quite similar in both groups. The age at surgery was 9.4 years in STL group and 10.6 years in STTX groups, while follow-up time was 5.7 years and 4.4 years, respectively. According to the mean values, patients received surgery before growth spurt and they were followed until the average age of 15 years, in both groups, which makes the effects of growth on them very similar.
Conclusion
In the present study, patients who received STTX exhibited more improvement of knee extension at clinical examination and during gait than those who underwent to STL; however, STTX was not effective to prevent the increase of APT after flexed knee gait treatment.
Footnotes
Authors’ note
The study was conducted at Association for the Care of Disabled Children, São Paulo, Brazil.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.