
Abstract
Introduction:
We undertook a retrospective study to stratify the effect of patient’s age, delay in surgical drainage, and Staphylococcus aureus (SA) virulence on expected clinicoradiological outcomes following suppurative arthritis of hip joint in a walking child.
Materials and methods:
The study was conducted in 18 children over 2 years of age who suffered from joint fluid culture-positive SA arthritis of hip joint and treated with open arthrotomy. Outcomes were defined on the following criteria: age of child (≥5 years or <5 years), duration of symptoms elapsed before surgical intervention (≥5 days or <5 days), and virulence of SA (methicillin-resistant Staphylococcus aureus (MRSA)/methicillin-sensitive Staphylococcus aureus)). The final clinical results were graded according to Moon’s clinical criteria and radiologically by types described by Choi et al.
Results:
The mean patient age was 6.22 years at the time of index procedure. The average delay in surgery was 17.06 days. Follow-up averaged 15.28 months. Five patients had associated with osteomyelitis femur in preoperative radiographs. MRSA culture was grown in 8 hips (44.4%) of 18 hips. Unsatisfactory clinical results according to Moon’s criteria were obtained in 55.6% patients with 38.9% being MRSA infected. Unsatisfactory Choi’s radiological results were present in 33.3% patients, 27.8% under MRSA category. Our study did not find age to be a significant factor either in clinical or radiological outcome. The clinical results were unsatisfactory in 81.8% patients with surgical delays when compared to early surgery (p < 0.05).
Conclusions:
The clinicoradiological outcome in suppurative hip arthritis of walking children was unsatisfactory when there was delay in treatment beyond 5 days, and the causative organism was virulent (MRSA). The presence of preoperative joint incongruency or osteomyelitis of proximal femur was another risk factor.
Introduction
Hip is the second commonest joint after knee to be affected by suppurative arthritis. Several characteristics of hip joint in childhood make it prone to infection and subsequent damage thereof. The intra-articular metaphysis, tenacious end arterial blood supply, deep intramuscular location masking external manifestations of inflammation, its weight-bearing responsibilities and presence of several physeal plates in the region are some of the features unique to the hip joint. The products of inflammatory and bacterial toxins that develop during suppurative arthritis can rapidly destroy the articular cartilage of the hip and acetabulum. There may as well be concomitant osteomyelitis of femur. Raised intracapsular pressure and vascular insults can result in further devascularization of the femoral head. 1 An established suppurative collection in the joint requires drainage either through open arthrotomy or arthroscopically. 2
The occurrence of suppurative arthritis in children is gradually decreasing in high income countries because of better nutrition, living conditions, and advanced diagnostics. 1 However, suppurative arthritis still remains one of the most dreaded problems in low-income countries, despite progress in health-care facilities and therapeutic measures. 3 –5
The clinicoradiological outcome following suppurative arthritis of hip joint in children has been described previously, but most reports appear outdated looking at the current health-care perspective. 6 –10 Methicillin-resistant Staphylococcus aureus (MRSA) infection has emerged in a big way following extensive use of antibiotics and changed the clinical and complication profile of osteoarticular infections. 11 –13 Several other reports in the literature have emphasis on hip involvement in neonates and infancy, where disease progression is probably quite different from an older child. 14 –18 Exclusive pediatric series focusing on affection of hip joint in a walking child and resulting morbidity of suppurative arthritis are scanty. 19 We, therefore, undertook this retrospective study to stratify some of the risk factors to guide clinicians on management and expected clinical outcomes following suppurative arthritis in this particular age group.
Materials and methods
This retrospective chart review (2015–2017) was conducted at a tertiary care pediatric super specialty health care center located in the suburb of a low-income country. It included 18 previously healthy and immunocompetent walking children over 2 years of age diagnosed with joint fluid culture-positive Staphylococcus aureus (SA) (both MRSA and methicillin-sensitive Staphylococcus aureus (MSSA)) arthritis of the hip joint. Informed written consent from the patients and guardians was obtained for publication of results and photographs.
All studied patients had been managed with an institutional protocol of prompt open arthrotomy, debridement, and copious irrigation under general anesthesia. Starting with intravenous empirical broad-spectrum antibiotics, treatment was changed early in line with culture sensitivity reports. Following drainage, the hips were kept nonweight bearing in traction for 2–3 weeks to reduce pain during the acute phase of the disease. This was followed by progressive weight bearing with support as tolerated.
Outcomes were defined on the following criteria: age of the child at the time of hospital presentation, duration of symptoms elapsed before surgical intervention, virulence of SA (MRSA/MSSA), and clinical assessment at follow-up. The final clinical results were graded as excellent, good, fair, and poor according to Moon’s outcome assessment, which included clinical evaluation scales 20 (Table 1). The classification was chosen in view of squatting and cross-legged sitting practices of the region.
Modified Moon’s criteria for outcome assessment of hip function. 20

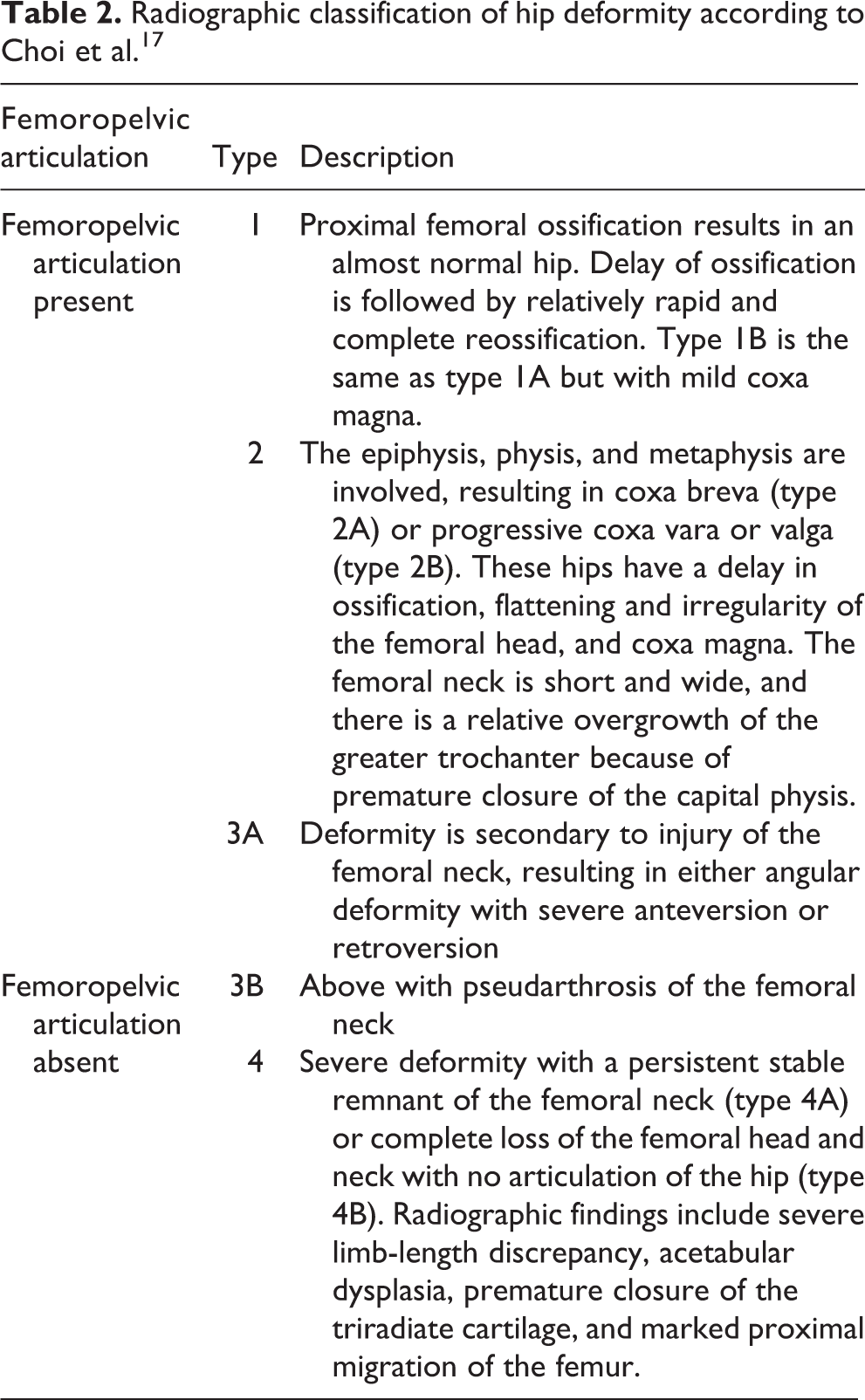
In addition, at the time of the most recent follow-up, we evaluated deformation of the proximal femur using the radiographic classification of the hip proposed by Choi et al. 17,19 (Table 2). Although this classification was designed for determination of treatment, we found it useful for description of sequelae observed as well. 19 The Choi 1, 2, and 3A grades were considered as satisfactory (femoropelvic articulation present); 3B and 4 unsatisfactory for the purpose of this study as these types had femoropelvic dissociation and always demanded major surgical reconstructive measure. The delays in surgical interventions were compared at 5 days. 2,6,9,10,21 For statistical analysis, patients with Moon’s excellent or good results were grouped as satisfactory, and patients with poor or fair results were grouped as unsatisfactory. Since no previous study guided the intragroup comparisons, the age was arbitrarily chosen above and below 5 years (preschool and primary school group). We calculated overall summary statistics in terms of means and standard deviations for continuous variables. After the descriptive analysis, we performed comparisons using the Pearson’s χ 2 test and Fisher’s exact test for various categorical variables and the outcome of suppurative arthritis for the groups—age, delay in surgical intervention before and after 5 days, and MRSA/MSSA infection. All statistical analyses were performed with the use of two-tailed tests, and significance was considered to be indicated by a p value of <0.05. The free online statistical software (www.socscistatistics.com/tests/chisquare/) was used for statistical calculations.
Radiographic classification of hip deformity according to Choi et al. 17
Results
Infection was eradicated in all patients with no recurrence of infection or interventions for osteomyelitis of the proximal femur in the available follow-up. The mean patient age was 6.22 ± 2.44 years at the time of index procedure. There were 7 males and 11 females. Right hip was involved in 10 and left in 8 patients. The average delay in surgery was 17.06 days (range 2–60 days). MRSA culture was grown in 8 hips (44.4%) of the 18 hips. Follow-up ranged from 15.28 ± 8.53 months. Unsatisfactory clinical results according to Moon’s criteria were obtained in 10/18 patients (55.6%) with 7 of 18 (38.9%) being MRSA infected. Unsatisfactory Choi’s radiological results (3B + 4) were present in 6 of 18 (33.3%) patients, 5 of 18 (27.8%) being MRSA category.
At admission, erythrocyte sedimentation rate was elevated in (>22 mm/h) in 11 of 18 (61.1%) patients and C-reactive protein (CRP; >0.3 mg/dL) in just 7 of 18 (38.9%). None of our patients required transfers to intensive care units.
Preoperative radiographs: Changes of the hip joint in the preoperative X-rays were observed in 5 of 18 patients (27.8%) and these changes were either single or multiple (Table 3). Infecting organism was MRSA in three and MSSA in two patients. All five patients had arthritis associated with osteomyelitis femur. The average delay in surgical drainage in these patients ranged from 7 days to 60 days. Two of the above patients had concomitant joint subluxation/dislocation. The clinical outcome was unsatisfactory in all these patients. Radiologically, three patients were unsatisfactory at follow-up.
Patient profile in patients with preoperative radiological changes of joint subluxation/dislocation and osteomyelitis of proximal femur.

MRSA: methicillin-resistant Staphylococcus aureus; MSSA: methicillin-sensitive Staphylococcus aureus.
Follow-up assessment: The Moon’s score was excellent in 4, good in 4, fair in 3, and poor in 7 at follow-up evaluation. A limb length discrepancy greater than 2.5 cm was seen in three patients. The follow-up radiological assessment had six patients in 1A, one in 1B, none in 2A, two in 2B, two in 3A, two in 3B, two in 4A, and two in 4B category.
Statistical analysis and the risk factors (Figures 1
to 4): Age and outcome (Table 4)—Our study did not find age (5 years) to be a significant factor either in clinical or in radiological outcome. Delay in surgery from the onset of symptoms and clinical outcome (Table 5)—With delays beyond 5 days, the results were unsatisfactory in 9 of 11 patients (81.8%) when compared to early surgery (p < 0.05). Delay in surgery from the onset of symptoms and radiological outcome (Table 5)—Similar to clinical outcome, a delay in surgical drainage beyond 5 days resulted in unsatisfactory radiological types in 6 of 11 patients (54.5%; p < 0.05). Organism virulence and clinical outcome (Table 6)—The patients with MSSA had satisfactory outcome in 7 of 10 (70%), whereas the MRSA group had unsatisfactory results in 7 of 8 (87.5%). The clinical outcome was statistically different between the two groups (p < 0.05). The only case with satisfactory clinical outcome in the MRSA group was one with surgical drainage occurring within 3 days. Organism virulence and radiological outcome (Table 6)—The patients with MSSA had favorable outcome in 9/10 (90%), whereas the MRSA group had unsatisfactory results in 5 of 8 (62.5%). The results were statistically significant (p < 0.05). The three cases where there was satisfactory radiological outcome with MRSA were drained within 15 days of symptom onset.

The risk factors for satisfactory and unsatisfactory outcome for suppurative hip arthritis in walking child.

(a) Patient aged 5 years infected with MSSA drained at 15 days. (b) There were preoperative radiological changes of osteomyelitis and joint subluxation. (c) Outcome was unsatisfactory both clinically and radiologically. MSSA: methicillin-sensitive Staphylococcus aureus.

(a and b) Patient aged 7 years infected with MRSA drained at 6 days. (c and d) Outcome was unsatisfactory both clinically and radiologically. MRSA: methicillin-resistant Staphylococcus aureus.

(a and b) Patient aged 5 years drained at 30 days. The child’s hip joint was infected with MRSA and presented with preoperative osteomyelitis and joint subluxation. (c to f) Sequential radiological changes at 6 weeks, 2, 4, and 6 months, respectively. Outcome was unsatisfactory both clinically and radiologically.
Outcome analysis based on age of the patient.

a χ 2 test.
Outcome analysis based on delay in surgery.
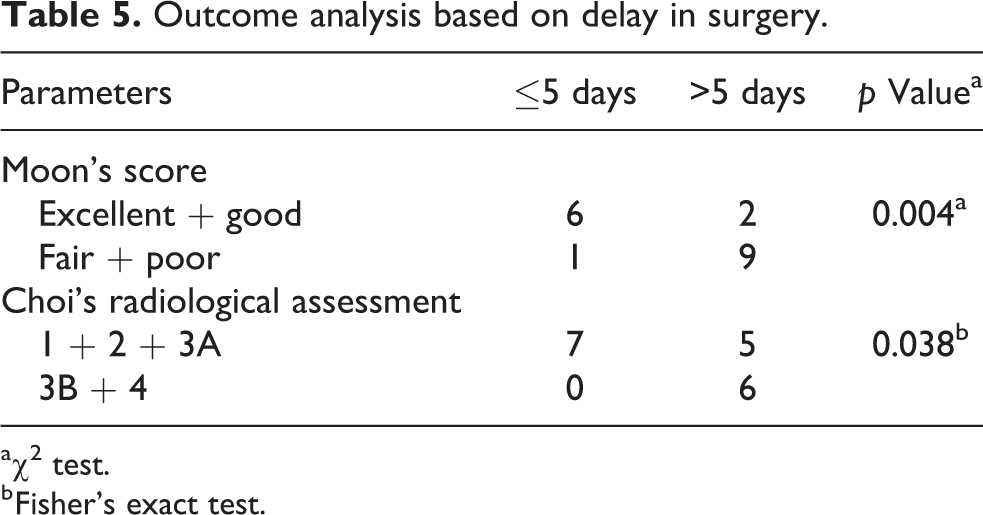
a χ 2 test.
b Fisher’s exact test.
Outcome analysis in MRSA and MSSA groups.

MRSA: methicillin-resistant Staphylococcus aureus; MSSA: methicillin-sensitive Staphylococcus aureus.
a χ 2 test.
Discussion
Hip suppurative affection in neonates and infants is quite different from a walking child. 22 Presence of transphyseal vessels and intracapsular metaphysis in infants allow early spread of infection into the joint. Thus, there is rapid joint destruction and high potential for osteonecrosis in immature children. 1 Early diagnosis is a problem in small kids as there is inability to report symptoms, minimal systemic signs, and often normal laboratory and radiographic findings as well. Prematurity, because of immature immune system and low levels of passively transferred maternal immunoglobulins, is another contributing factor.
Unlike the younger age group, the older child is potentially immunocompetent and many of the above considerations do not apply here. Yet joint infections do occur in this age group as well. 3 –5,19 Additionally, even in this age group, a delay in diagnosis is frequently encountered. The possible reasons are not including infection as a possible differential for hip pathology or a delay in obtaining timely and adequate medical treatment. 4 It is well established that the prognosis of suppurative arthritis in infants is closely associated with age, treatment delay, 9 and the organism responsible. 4,23,24 Whether the similar factors decipher the outcome in older walking children is still unknown. We tried to find out the influence of these various factors on outcome of suppurative arthritis of the hip joint in this age group through a retrospective study model.
Despite a thorough literature search, we could not find studies investigating the effect of age in suppurative arthritis of hip in older children. Therefore, we kept the criteria of predominant family (≤5 years; preschool) and community exposure (>5 years; school going) to decide the age landmark. However, age of the patient was not found to be a significant factor influencing clinical or radiological outcomes for our study (p > 0.05).
The suppurative hips were considered a surgical emergency at our institution irrespective of their duration of symptoms prior to presentation at our institution. There was a significant delay in presentation of child to our institution (17.06 ± 20.89 days). A surgical delay beyond 5 days indicated an unsatisfactory clinical and radiological outcomes (p < 0.05), as already established in the literature (Table 5). 2,6,9,10,21 This is understandable as joint destruction progresses rapidly following delayed surgical intervention.
Overall, SA is the most common pathogen that causes septic arthritis. 25 MRSA suppurative arthritis in children has been associated with an increased number of surgical interventions, longer duration of febrile days, extended courses of antibiotics, and increased sequelae. 7,8,12,17, 26 In a pediatric study based on 158 cases originating from a high income country, the authors highlighted the increasing trend of MRSA infections. 13 There was significantly increased risk for subperiosteal abscess formation, requirement of surgical procedures, and mean length of hospital stay in patients with MRSA, as compared to those with MSSA infections. In a recent pediatric study, with 148 cases of acute, community acquired musculoskeletal SA infections (MRSA, n = 37 and MSSA, n = 111), again an increasing trend of MRSA infections was seen. 27 Compared with MSSA, MRSA infections resulted in higher CRP levels at presentation, longer hospital inpatient stays, multiple surgical procedures, increased sequelae (27% vs. 6%, p < 0.01), and more frequent admissions to the intensive care unit. Experiences from low income countries involving MRSA osteoarticular infections in children are even worse. 5 In one study, of the 74 pediatric patients with culture-positive SA bone and joint infection, 41 had MRSA (55%). 5 The MRSA group had a significantly higher erythrocyte sedimentation rate (ESR), CRP, neutrophil count, and white blood cell count. The MRSA group also had longer febrile days, hospital stay, and antibiotic course compared to the MSSA group. Mortia et al. in a small Japanese study compared four neonates with MRSA infection with non-MRSA cases (mean age at infection 2.2 years). 19 The MRSA cases exhibited severe limb length discrepancy and their heads had advanced deformation according to Choi classification.
As is obvious from the results of our study, the MRSA group had both unsatisfactory clinical and radiological outcomes compared to the MSSA group (p < 0.05; Table 6). In the past, 10–40% of patients with hip involvement have been reported to suffer significant sequelae, such as growth plate damage and loss of hip function. 22, 28 However, more recent studies have reported the incidence of long-term sequelae of appropriately treated septic arthritis of the hip to be around 3–5%. 29 For our series of 18 walking children, unsatisfactory clinical results according to Moon’s criteria were obtained in 10 of 18 patients (55.6%) and Choi’s radiological results (type 3B or 4) were present in 6 of 18 (33.3%) patients. This is significantly high compared to results described for sequelae in infants. 11,12,14 –17 Patients with poor or fair clinical outcome had delayed surgery in 9 of 10 (90%) cases. The causative organism was MRSA in 7 of 10 (70%) hips. Another finding with worsened clinical outcome was the presence of preoperative radiological changes 5 of 10 (50%).
From the results of our study, it emerges that hip joint is rapidly damaged by the virulent suppurative infection even in older walking child unless salvaged by emergent drainage. The joint characteristics of being a closed space, presence of large articular surfaces, and the precarious blood supply of bone ends probably contribute to its destruction. However, in patients where early treatment was offered, the joint recovered reasonably and good function was restored.
We acknowledge that a sample size of 18 patients is small which may not represent a complete description of the disease in the general population. The retrospective nature of our study may have affected our data collection. There was no control on initial exposure or outcome obtained for the series. The duration of symptoms was based on parent’s/guardian’s recall. Such recalls may not be exactly precise. We did not include patient’s prior treatment history before reaching our institution as it was ineffective in controlling infection (collections seen in all patients at the time of drainage). Suppurative arthritis of hip is relatively uncommon disease and outcomes are largely unfavorable. Therefore, it seemed justified to analyze outcomes even in a small series. The strength of our study was an exclusive series dealing with suppurative arthritis of hip joint in a walking child. The study had a reasonable follow-up of average 15 months at which most of the sequelae of suppurative pathology have already been manifested. 11 In view of unsatisfactory outcomes observed in a significant number of patients in our study, one can infer the requirement of an aggressive management following suppurative hip arthritis, as recommended for neonates and infants. Although the advanced diagnostic and therapeutic interventions are highly desirable, the clinicians practicing in low income regions should develop a high index of suspicion for a suppurative diagnosis. The patient should be offered appropriate medical and surgical treatment when infection is one of the possible differentials. This timely management will help a great degree in preventing the late crippling disability resulting from this pathology. Further, suppurative arthritis can have long-term sequelae and deformities related to growth plate arrest. We suggest a prospective study design and a larger series followed long term to assess these.
Conclusions
The clinical and radiological outcomes in suppurative hip arthritis of walking children were unsatisfactory when there was delay in treatment beyond 5 days and causative organism was virulent (MRSA). The presence of preoperative joint incongruency or proximal femoral osteomyelitis was another risk factor.
Footnotes
Author contributions
AA was involved in study design, statistical analysis, and manuscript preparation and VKKH performed measurements and manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.