
Abstract
Purpose:
The purpose of this study was to assess the effectiveness of periarticular multidrug infiltration (PMDI) and compare it with that of epidural catheter use.
Methods:
Fifty-eight patients (58 joints) who underwent total knee arthroplasty were included in this single-center, prospective, parallel, randomized, controlled trial. Preoperatively, patients were randomly categorized into the PMDI and epidural catheter groups. We evaluated postoperative pain (visual analog scale (VAS) and narcotic consumption), functional outcomes (range of motion (ROM) of knee flexion, the day patients could perform the straight-leg raising (SLR) test, and day of starting cane use), and laboratory data (white blood cell (WBC) and C-reactive protein (CRP)).
Results:
There was no significant difference in the VAS score, ROM of knee flexion, the day patients could do SLR, and the day of starting cane use between the PMDI and epidural catheter groups. However, the PMDI group could perform SLR on a postoperative day (POD) 1 (p < 0.05). WBC level on POD 1 was significantly higher in the PMDI group (p < 0.05), whereas the CRP levels on POD 1 (p < 0.01), 3 (p < 0.01), and 5 (p < 0.01) were significantly lower in the PMDI group than in the epidural catheter group. The frequency of side effects was not significantly different between the groups.
Conclusion:
PMDI was as effective as epidural catheter use for pain control. A higher percentage of patients who underwent PMDI could perform SLR on POD 1; therefore, the functional recovery was earlier in the PMDI group than in the epidural catheter group. PMDI may suppress inflammation in the whole body because of steroids.
Keywords
Introduction
The number of patients undergoing total knee arthroplasty (TKA) has been increasing worldwide. Given that TKA is known as the most common invasive procedure, postoperative pain can interfere with rehabilitation and extend the hospital stay; hence, pain control after TKA is essential. Although epidural catheter reduces postoperative pain, it also induces postoperative nausea and vomiting (PONV), urinary retention, hypotension, pruritus, and motor block. 1 –3 In particular, female patients with a body mass index ≤20 kg/m2 were more likely to suffer from PONV. 4 These side effects not only affect rehabilitation and hospital stay but also can lead to pulmonary thromboembolism, urinary tract infection, and pneumonia. 5 –8 Periarticular multidrug infiltration (PMDI) in arthroplasty has been reported. This method reduces narcotic consumption and improves functional outcomes in patients undergoing total knee and total hip surgeries. 9,10
Although PMDI was frequently reported in TKA, there are only a few reports focused on not only pain evaluation but also functional and laboratory evaluations simultaneously. Therefore, we aimed to compare PMDI to the epidural catheter in TKA to evaluate the effectiveness of PMDI. We hypothesized that PMDI would result in better pain control, faster functional recovery, and lesser side effects than the epidural catheter.
Materials and methods
Participants
Expecting a moderate effect size (d = 0.5) for the t-test analysis between two dependent means and a requirement of 80% power to detect an existing difference, the required sample size was 27 participants for each of the PMDI and epidural catheter groups. Participants were recruited between May 2017 and March 2019. This study included 58 patients (58 joints: 30 in the PMDI group and 28 in the epidural catheter group). Inclusion criteria were patients diagnosed with osteoarthritis and underwent primary TKA from May 2017 to March 2019. Exclusion criteria were as follows: minors aged <20 years, patients with prior ipsilateral knee surgery, those with postlumbar operation, and those with rheumatoid arthritis, renal failure, dementia, or mental impairment. Screening was carried out for 82 patients, and 58 patients (30 in PMDI group and 28 in the epidural catheter group) were enrolled in the study. The enrollment process is further detailed in Figure 1. All procedures used in this research were approved by the Ethical Committee of the author’s institution (approval no. 16R-289). The study was undertaken in accordance with the Declaration of Helsinki.

CONSORT flow diagram of patient enrolment.
Randomization and intervention
The Consolidated Standards of Reporting Trials statement guidelines were followed for this single-center, prospective, parallel, randomized (1:1), controlled trial. The study and data collection were performed at the author’s institution. All patients signed written informed consent. After obtaining consent, patients who received TKA from May 2017 to March 2019 were divided into the following two groups using a computer-generated randomization table: PMDI and epidural catheter groups. The randomization table consisted of numbers (from 1 to 10) and alphabets (from A to J). All participants chose each number and alphabet. A participating orthopedic surgeon who assessed the patient eligibility was not involved in randomization, thereby securing allocation concealment. The other orthopedic surgeons took charge of assigning the patients.
The patients who received PMDI were injected a liquid solution containing 150 mg of 0.2% ropivacaine, 0.2 mg of adrenaline, 40 mg of methylprednisolone, and 10 mL of saline into the capsule of the knee after setting the components. Moreover, 150 mg of 0.2% ropivacaine, 0.2 mg of adrenaline, and 10 mL of saline were injected into the muscles and subcutaneous tissues before wound closure (Table 1).
Details of the intervention groups.

PMDI: periarticular multidrug infiltration.
Epidural catheter was inserted at the L1-2 or L2-3 level. The epidural space was identified by loss of resistance to air, and test dose (1% lidocaine) was administered. Patients received an epidural bolus of 0.2% ropivacaine (8 mL) during wound closure. At the same time, epidural infusion was started (0.2% ropivacaine 296 mL and fentanyl 4 mL). Analgesics were continuously infused at a rate of 4 mL/h through the epidural catheter, which was removed 2 days after the operation (Table 1).
Anesthesia
All patients underwent TKA under general anesthesia. Anesthesia was induced by rocuronium bromide and remifentanil hydrochloride. As there was a possibility that light anesthesia might affect PONV, general anesthesia was maintained with total intravenous propofol. Acetaminophen (1000 mg) and metoclopramide (10 mg) were administered at the end of the operation. For postoperative analgesia, oral acetaminophen was administered at a dose of 1800 mg/day starting on the day after surgery. Postoperative pain was assessed by a Likert-type scale ranging from 0 to 6 (0, no pain; 1, very mild; 2, mild; 3, moderate; 4, severe; 5, very severe; 6, intolerable), and severe pain was defined as >4 in the Likert-type scale. Severe pain was treated with intravenous infusion of acetaminophen (500 mg), pentazocine (15 mg), or flurbiprofen (50 mg).
Surgical procedure
In all patients, the surgery was performed with a parapatellar approach by three surgeons. After cutting the distal femur, proximal tibia, and patella, cement components were placed (femur: NexGen®, LPS flex, Zimmer-Biomet, Warsaw, IN, USA, tibia: NexGen®, MIS tibia component, Warsaw, IN, USA, patella: NexGen®, all poly patella, Warsaw, IN, USA). Tourniquets were used in all patients during implantation. All patients were allowed to do weight-bearing as tolerated on the day after surgery.
Outcomes
We set the primary outcome as pain evaluation and the secondary outcome as the functional outcome and laboratory data. We evaluated pain using the visual analog pain scale (VAS; 0 mm = no pain, 100 mm = worst imaginable pain) and narcotic consumption. VAS was recorded while patients were resting in the morning. VAS was assessed from the day of the surgery (1 h after surgery) to 7 days after surgery. Narcotic consumption was recorded until postoperative day (POD) 3. We also recorded the active range of motion (ROM) of knee flexion, and the day patients could perform straight leg raising (SLR) test, the ratio of the patients who could perform SLR on POD 1, and the day of starting cane use as the functional outcomes. ROM and SLR were performed in the morning. Patients tried to flex their operated knees by themselves in a supine position. The SLR test was also conducted in a supine position, and patients were considered to be able to perform SLR when they could elevate their limbs and maintained the position for at least 3 s. Furthermore, we also evaluated the patients’ laboratory data (white blood cell (WBC), C-reactive protein (CRP), and side effects (PONV, numbness, infection, and itch)). A blood test was conducted on PODs 1, 3, 5, and 7.
Statistical analysis
Statistics analysis was performed using SPSS statistical software version 25. Patient demographics and baseline characteristics were described and compared between groups according to their distributions. The paired t-test was used to evaluate VAS, narcotic consumption, ROM, laboratory data, and the day of starting cane use. Fisher’s exact test was used to evaluate the ratio of the patients who could perform SLR on POD 1 and the side effects. All tests were performed at the significance level of p < 0.05.
Result
Patient population
All patients followed up in both groups. A total of 82 patients were enrolled; of these, only 58 patients were analyzed and allocated to the PMDI group (n = 30) and epidural catheter group (n = 28). The baseline characteristics of the patients are presented in Table 2. There were no significant differences between the groups in sex, age, body mass index, and preoperative ROM of knee flexion.
Patients’ demographic data.

ROM: range of motion; PMDI: periarticular multidrug infiltration.
Clinical and functional outcomes
The VAS scale of the PMDI and epidural catheter groups was not significantly different (Figure 2). There was no significant difference in the narcotic consumption between the two groups (Table 3). As for the functional outcome, there was no significant difference in postoperative ROM of knee flexion (Figure 3). Although the day that the patients could perform SLR was not significantly different between the two groups, a higher percentage of the patients who underwent PMDI could perform SLR on POD 1 (p < 0.05; Table 3). The day of starting cane use was not significantly different between the PMDI and epidural catheter groups (Table 3). The WBC level on POD 1 was significantly higher in the PMDI group than in the epidural catheter group (p < 0.05) (Figure 4). In contrast, CRP level on PODs 1 (p < 0.01), 3 (p < 0.01), and 5 (p < 0.01) was significantly lower in the PMDI group than in the epidural catheter group (Figure 4). As for the side effect, two patients had lower numbness and two patients had vomiting in the epidural catheter group. On the other hand, only one patient had transient nerve palsy in the PMDI group. The side effects were not significantly different between the two groups.

Mean pain score over time for anaesthetic PMDI and epidural catheterisation groups.
Postoperative narcotic consumption and functional evaluation (SLR and cane use).a

a WBC and CRP are presented as the mean and standard deviation.
POD: postoperative day, SLR: straight leg raising; WBC: white blood cell; CRP: C-reactive protein; PMDI: periarticular multidrug infiltration.
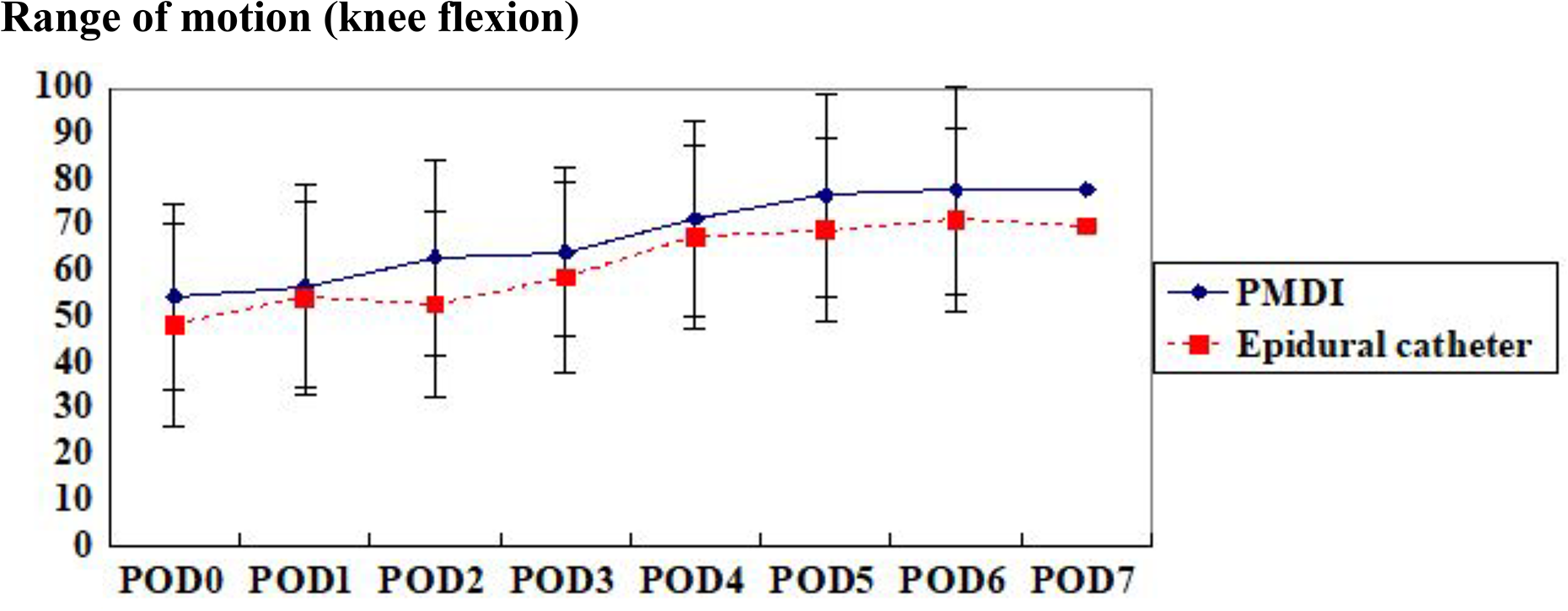
Mean Range of motion for anaesthetic PMDI and epidural catheterisation groups.

Mean laboratory data over time for anaesthetic PMDI and epidural catheterisation groups.
Discussion
In this study, we compared the effectiveness of PMDI and epidural catheter among patients who underwent TKA. Regarding postoperative pain, VAS score and narcotic consumption were not significantly different between the PMDI and the epidural catheter groups. In terms of functional outcome, there was no significant difference in ROM and the day that the patients could perform SLR between the PMDI and epidural catheter groups. However, the PMDI group could perform SLR earlier than the epidural catheter group on POD 1. Regarding laboratory data, the PMDI group had significantly higher levels of WBC on POD 1 and significantly lower levels of CRP on PODs 1, 3, and 5 than the epidural catheter group.
Since Ranawat et al. reported PMDI for the first time in 2007, 11 PMDI has been widely performed for TKA. 9,10,12,13 Although these reports were prospective studies, they did not evaluate the functional outcome (ROM, SLR, and cane use) and laboratory data of the patients at the same time.
The content of PMDI varies in different studies. In this study, we used ropivacaine and methylprednisolone for PMDI. Ropivacaine is a pharmacokinetically similar local anesthesia but it has a more prolonged duration of action and a lower toxicity profile than bupivacaine. 12,14,15 Therefore, while other reports mostly used 300–400 mg bupivacaine, 14,16 –18 we used 300 mg of ropivacaine in this study. Salerno and Hermann 19 reported that local injection of corticosteroids could be used in musculoskeletal tissues and joints without major complications and that pain and functional recovery were improved. Furthermore, Tsukuda et al. 20 compared PMDI with corticosteroid with PMDI without corticosteroid and reported that the pain score of patients who underwent PMDI with corticosteroid was significantly lower than that of patients who underwent PMDI without corticosteroid. These reports recommended the addition of corticosteroid in PMDI because it was safe and effective for postoperative pain.
As for the VAS score, there was no significant difference observed between the PMDI and the epidural catheter groups. Tsukuda et al. 21 also compared PMDI with epidural catheter and reported that the postoperative VAS score at 4 and 24 h of PMDI was significantly lower than that of the epidural catheter. However, no particular effectiveness was observed in PMDI after POD 1. The contents of PMDI differed in the previous studies. We did not use opioids because they may cause nausea, vomiting, and itchiness. We also avoided the use of ketoprofen because it may worsen kidney dysfunction and may lead to gastric ulceration. There is a possibility that these factors may affect the result.
There are only a few reports that have evaluated the relation between PMDI and laboratory data. Although we did not consider that PMDI did not affect the laboratory data, because PMDI was injected only in local tissues, the WBC level was significantly higher on POD 1, whereas the CRP level on PODs 1, 3, and 5 was significantly lower in the PMDI group than in the epidural catheter group (Figure 4). Similarly, Ishida et al. 22 reported that the CRP level of PMDI from PODs 1–7 was significantly lower than that of the continuous femoral nerve block. We predicted that neutrophil was released from the bone marrow to the blood, and inflammation was suppressed by injecting corticosteroid. Based on the laboratory data, the corticosteroids might have suppressed the general inflammation by decreasing the CRP level.
Regarding functional evaluation, Parvataneni et al. 13 reported that 63% of the patients in the injection group could perform SLR on POD 1. Similarly, we revealed that 67% (20 of 30 patients) of the PMDI group could perform SLR on POD 1 (p = 0.02). In contrast, only 32% (9 of 28 patients) of the epidural catheter group could perform SLR on POD 1 (Table 3). PMDI provided good pain control similar to the epidural catheter, whereas the functional outcome (SLR) was better by PMDI than by epidural catheter. Thus, PMDI was better for TKA than the epidural catheter.
This study has several limitations. The operations were performed by three surgeons, which may have affected the results of this study. However, all surgeons have sufficient years of experience (>10 years) in performing orthopedic procedures, and the surgical technique is unified. Second, this study was not blinded; thus, we knew which treatment the patients were receiving, which could have led to a bias.
Conclusion
Our data showed that PMDI was as effective as epidural catheter use for patients undergoing TKA for pain control and showed better functional outcome improvement (a higher percentage of the patients who underwent PMDI could perform SLR on POD 1). Moreover, PMDI led to lesser inflammation than epidural catheterization because of steroid use.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.