
Abstract
Purpose:
To prospectively evaluate whether time to debridement has any correlation with union, infection, and quality of life in high-grade lower limb fractures in a tropical setting.
Methods:
A prospective cohort study was conducted at a tertiary care center in South India. Two hundred fifty-four adult skeletally mature patients with 301 grade 3 fractures involving the femur, tibia, or fibula were recruited. The cohort was empirically divided into two groups (early and late) based on the time to debridement (less than or more than 12 h from injury).
Outcome:
The primary outcome was nonunion. Secondary outcomes were deep infection rates and patients’ quality of life. Short form-36 (SF-36) and short musculoskeletal functional assessment (SMFA) questionnaires were also used. Patients were followed up for 9 months.
Results:
The follow-up rate was 93%. The late group had a significantly higher risk of nonunion (odds ratio(OR): 6.5, 95% confidence interval (CI): 2.82–14.95) and infections (OR: 6.05, 95% CI: 2.85–12.82). There was a 4% increase in the infection risk for each hour of delay for the initial 50 h (p < 0.0001). SF-36 and SMFA scores were superior in the early group (p < 0.0001).
Conclusion:
The study contradicts findings reported in the literature from the West. Our study was in agreement with our hypothesis and proved that debridement within 12 h resulted in significantly lower rates of nonunion and infections and an overall improved quality of life in high-grade open lower limb fractures in a developing country.
Level of evidence:
Level II
Trial registration:
German Clinical Trials Register DRKS00015186
Introduction
A large part of the favorable outcomes in open fractures, in addition to better technology and understanding of pathophysiology, was believed to be due to early wound debridement. This made it possible to achieve good outcomes even in previously unsalvageable limbs. This line of thinking appears to have been challenged lately. Although there is a universal agreement that debridement should be done as soon as possible, resource management issues have tended to delay debridement at untimely hours. Recent literature from the West shows acceptable outcomes with late debridement. 1 –5 The setting appears to be different in developing countries. The number of open fractures appears to be more frequent in the developing world and are increasingly high-velocity injuries. In addition, there can be delay in transportation and absence of protective clothing. 6 –10
Most literature appears to favour surgical debridement even up to a time period of 24 h. 1 –5 We hypothesized that in a hot tropical developing country like ours, where road traffic accidents (RTAs) are rampant with grossly contaminated wounds, a delay in debridement would have detrimental consequences. One prospective study by Enninghorst et al. showed that timely debridement in open tibia fractures had good outcomes in terms of infection and union rates. 11 However, all patients underwent surgery within a mean time of 8 h. With this in mind, our study aimed to prospectively evaluate whether early debridement in our setting with a more varied time to surgery had lower nonunion and infection rates, along with a better functional outcome in high-grade long bone lower limb fractures, which included the femur as well. Further, given the large number of referrals and patients who often present late, an arbitrary time of 12 h was chosen, a cohort was designed based on the time to debridement (less than or more than 12 h from injury), and the outcome was compared in both these groups.
Materials and methods
We adhered to the STrengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline checklist.
Study design and setting
A prospective cohort study was conducted from November 20, 2015, to May 20, 2017, at a multispecialty tertiary care hospital in a tropical setting in South India. All patients provided informed written consent and were followed up for a period of 9 months. Participating surgeons included both residents and consultants. Formal approval was obtained from the institutional review board (IRB no. 9693) of the hospital before the commencement of the study. To achieve a standardized comparison, only grade 3 long bone lower limb fractures were analyzed. All patients provided informed written consent.
Inclusion and exclusion criteria
All adults, skeletally mature (as seen on radiographs) patients with grade 3 open fractures of the femur, tibia, or fibula, including intra-articular fractures, who provided informed consent were included. Patients with fractures involving the face, upper limb, trunk, spine, pelvis, patella, or foot; those who underwent primary debridement elsewhere; those with unsalvageable limbs requiring urgent amputation; and those unwilling to participate in the study were excluded.
A flowchart of the patient enrolment is shown in Figure 1. All patients underwent standardized wound debridement, antibiotic coverage, fracture fixation, elective debridement when required, and early wound coverage. 12 Postoperatively, most patients underwent standard wound care and negative pressure wound management only for those specifically implicated by the operating surgeon. Immediate, early, and delayed wound cover was purely the surgeon’s discretion. 12,13 The cohort was empirically divided into two groups (early and late) based on the time to debridement (less than or more than 12 h from injury).

Flowchart of the patients recruited.
Data collection
Data were obtained prospectively from all grade 3 lower limb fractures presenting to the emergency department and entered in a data entry proforma. Demographic variables such as age, sex, comorbid conditions (smoking, alcohol consumption, diabetes, low hematocrit, malnutrition, obesity, anemia, and respiratory disorders, such as asthma and chronic obstructive pulmonary disease), mechanism of injury, fracture location (femur and tibia/fibula), Gustilo and Anderson grade (3A, 3B, or 3C), 14 –16 contamination (mild/moderate or gross), American Society of Anesthesiology (ASA) grade, injury severity score (ISS), time to antibiotic prophylaxis, time from injury to surgical debridement, type of primary soft tissue coverage, and operating surgeon’s years of experience were recorded at the time of initial debridement. All patients were followed up for a period of 9 months.
Outcome measures
The primary outcome measure was nonunion. All patients were assessed both clinically and radiologically at 9 months for union, which is the maximum accepted waiting time period, as defined by the Food and Drug Administration (FDA) in 1986. Radiologically, a nonunion was defined as the absence of bone trabeculae crossing the fracture site, sclerotic fracture edges, persistent fracture lines, healing of less than three of four cortices, and lack of progressive change toward union on serial radiographs. 13,17,18 Clinically, persistent pain, tenderness, and abnormal mobility at the fracture site, along with the inability to hop on one leg, aided in the diagnosis. 19
The secondary outcome measure was the infection rate and patients’ quality of life. We followed the criterion of deep infections, defined as “wounds requiring an unplanned surgical debridement and/or sustained antibiotic therapy following definitive wound closure, excluding any pin tract infections or cellulitis.” 2 –4 At 1-month postinjury, wound healing was assessed clinically and by measuring C-reactive protein (CRP) values. 20 –23 Quality of life was assessed by evaluating the functional outcomes, readmissions, duration of hospital stay, number of secondary surgical procedures, direct cost analysis of inpatient bills, and major complications recorded over 9 months. Functional outcome was assessed by determining whether patients had returned to work at 9 months and by using health-based questionnaire scoring systems (short musculoskeletal functional assessment (SMFA) and short form-36 (SF-36) scores). 8,24 –26
Sample size
The sample size was calculated on the basis of retrospective data collected from the medical records of 50 patients with 50 open fractures of the lower limb. A ratio of 1:4 was obtained for the number of fractures debrided within and more than 12 h. The study was powered to detect a 20% difference in union rates.
With a power of 0.80 and the level of significance of 0.05, the number of fractures in the early and late group required was 62 and 155, respectively. 27
Analysis
Data were entered using Microsoft Excel 2013. Discrete variables, such as age, sex, comorbidities, and fracture grade, were evaluated using the independent two-sample t-test, and continuous quantitative variables, such as time, were examined using χ 2 test. Multivariable logistic regression was performed with a probability of nonunion as the primary outcome. Variable reduction was performed using the method described by Harrell et al., 28 with time to debridement as the predictor of primary interest. Time was also primarily analyzed as a continuous variable in the model to determine the additive effect of delay without arbitrary cut-off thresholds. A p value less than 0.05 was considered significant. Patients with missing data, including those with no clinical follow-up at 9 months, were excluded from the analysis.
Patient and public involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for or implementation of the study. This was a purely observational study with no influence from any source (internal or external) in the management plan or outcome.
Results
The demographics and fracture characteristics of the patients are listed in Table 1. The follow-up rate was 93% at the end of 9 months. A total of 231 patients with 274 open fractures were analyzed, of which 60 patients (75 fractures) were included in the early group and 171 patients (199 fractures) in the late group. The mean age of the patients was 41.5 (range 17–77) years, and the majority of patients were men (84% of all fractures). Of the risk factors, smoking was prevalent in 43% of patients, followed by the consumption of alcohol (40%), anemia (19%), and diabetes mellitus (11%). Most of the mechanism of accidents were due to RTAs (95%), of which 90% were motorcycle accidents. The remaining injuries resulted from crush injuries or falls. Furthermore, 73% of the wounds were grossly contaminated on arrival. The median ASA and ISS scores were 2 (range 1–5) and 14 (range 6–34), respectively. The overall median time to debridement was 15.7 (range 4.5–164) h. The mean time to antibiotic administration was 9.6 (range 1.4–122.4) h. Furthermore, 65%, 31%, and 4% of the fractures were of grade 3B, 3A, and 3C, respectively. Fractures involving the tibia/fibula and femur accounted for 65% and 35% of the total fractures, respectively. Only five patients had isolated fibula fractures, and this did not seem to influence the results. Debridement was performed by a consultant in 73% of the fractures and by residents under supervision in the remaining fractures. Primary internal fixation was performed in 72% of the fractures, primary external fixation in 25%, and debridement without any fixation device in 3% of the fractures, which were essentially stable.
All patients (n = 231) and fracture (n = 274) characteristics.
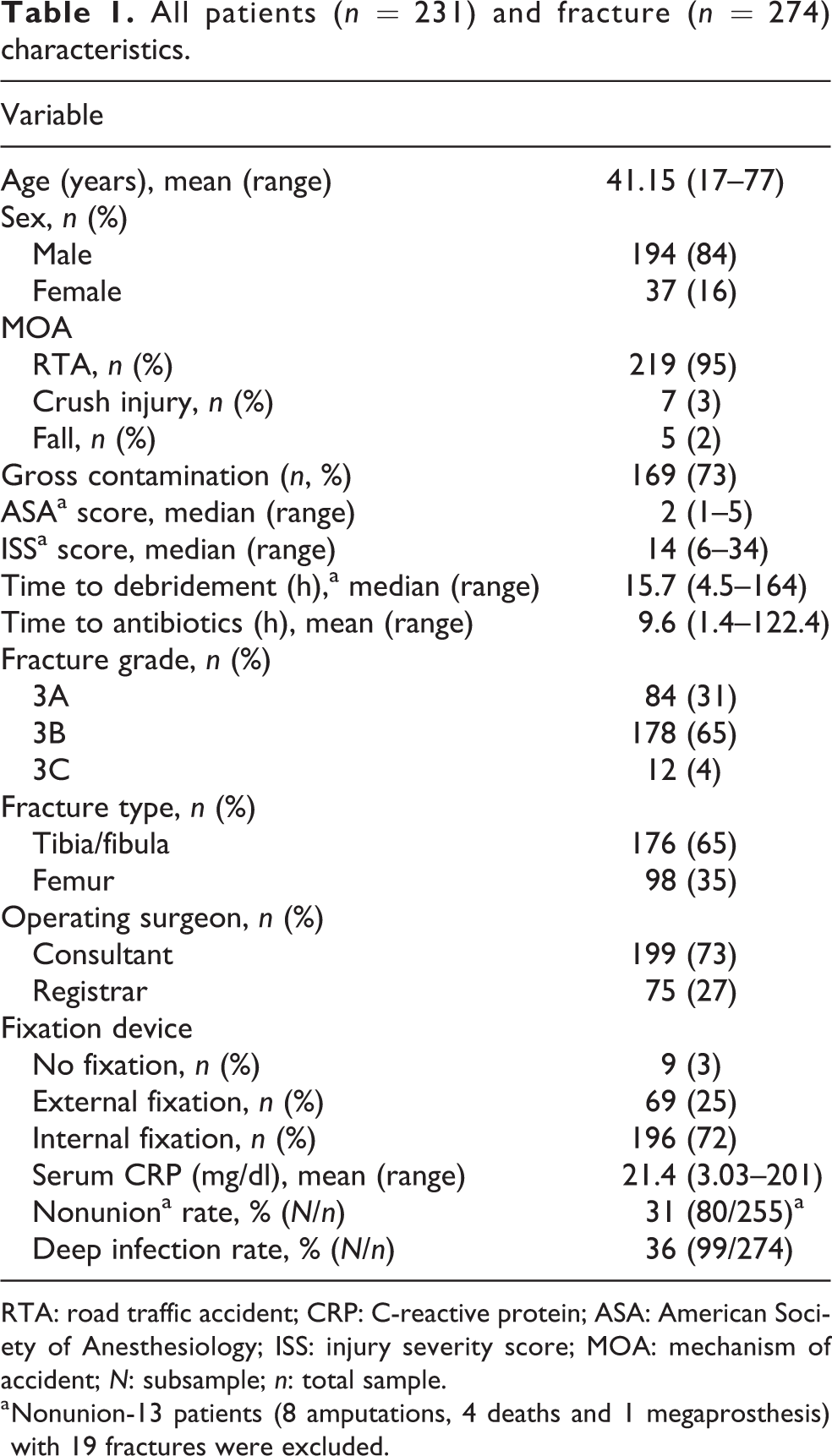
RTA: road traffic accident; CRP: C-reactive protein; ASA: American Society of Anesthesiology; ISS: injury severity score; MOA: mechanism of accident; N: subsample; n: total sample.
a Nonunion-13 patients (8 amputations, 4 deaths and 1 megaprosthesis) with 19 fractures were excluded.
Primary outcome measure: Nonunion
The overall nonunion rate at 9 months was 31%. Nonunion was observed in 80 patients. Thirteen patients with 19 fractures were excluded from the nonunion analysis. This included four patients who expired, eight that underwent an amputation before 9 months due to deep infections, and one who underwent reconstruction with a knee megaprosthesis in view of a femoral bone loss of 10 cm.
The odds ratio (OR) for nonunion in the late group is listed in Table 2. The nonunion rate in the late group was 4.4 times higher than that in the early group (40.5% vs. 9.3%).
Nonunion and infection rates for all fractures—odds ratio risk for debridement >12 h (n = 274).

a Statistically significant.
The adjusted multivariate regression analysis for nonunion in the early and late debridement groups is depicted in Table 3. The analysis was performed in three parts. First, we assessed whether the nonunion rate was significantly different between the two study groups. After adjusting for the correlation among fractures within the patients, we found this difference to be significant (crude OR: 6.5, P < 0.0001 in the late group, Table 2). Second, we tested for differences in baseline sociodemographic and clinical characteristics between the two study groups. This included variables, such as age, male gender, comorbidities (smoking, alcohol consumption, anemia [hemoglobin level < 10 g/dl], diabetes mellitus, and hypertension), ASA, ISS scoring, time to antibiotics, fracture grade, location, healing, fixation type, gross degree of contamination, CRP level at 1 month, and additional surgeries performed. Of these variables, a low hematocrit level, ASA score >2, grade 3B/3C, tibial fractures, presence of contamination, delayed wound cover at initial presentation and problems with wound healing, CRP level >6 mg/dl, and the total number of additional surgeries per patient were baseline differences between the two groups. Other variables showed no difference between both groups. Then, a multivariable logistic regression analysis was performed using the method of generalized estimating equations for the significantly different variables in both groups with the primary outcome being nonunion. After adjusting for factors found to be different in the univariate analysis, a delay of more than 12 h was found to be an independent predictor of nonunion in the multivariable analysis (adjusted OR: 5.2, p < 0.0001; Table 3). Higher fracture grade (3B/3C) over 3A type injuries (p = 0.02), prolonged wound healing (p = 0.01), and patients who had more than two surgeries (p < 0.0001) were also found to be significant predictors for nonunion (Table 3).
Multivariable regression analysis, for all fractures; primary outcome: nonunion (n = 274).

OR: odds ratio; CI: confidence interval; CRP: C-reactive protein; ASA: American Society of Anesthesiology.
a Statistically significant.
Secondary outcome measures: Infections and quality of life
As secondary outcome measures, we evaluated whether late debridement increased the risk of infections and its effect on patients’ quality of life. The overall infection rate was 36% and the mean serum CRP was 21.4 (Table 1).
We found that the infection rate in the late group was nearly four times higher than that in the early group (45% vs. 12%). The OR for the development of infections in the late group was 6.05 (Table 2). The association between time to debridement as a continuous variable and the overall infection risk is shown in Figure 2. We found that there was a 4% increase in the infection risk for each hour of surgical delay from the time of injury. This had a linear relationship for the initial 50 h (OR: 1.04, 95% CI: 1.02–1.06, p < 0.0001). A comparison between CRP levels and wound healing in the early and late groups is provided in Table 4. The patients who underwent debridement early had significantly lower serum CRP levels (p = 0.0004) and better wound healing at 1 month (p < 0.0001).
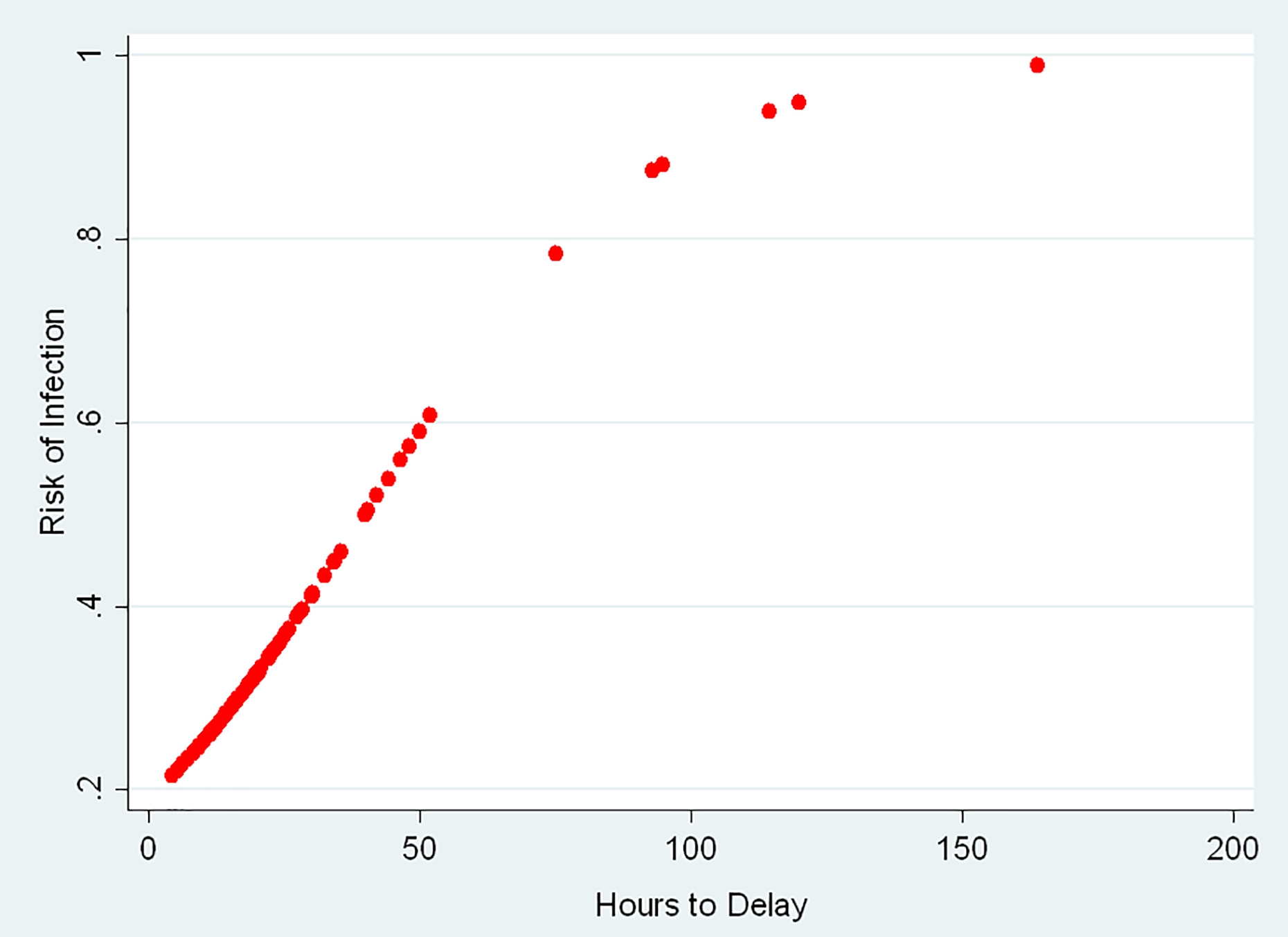
Odds of increase in infection risk for each hour of debridement (OR: 1.04, 95% CI: 1.02–1.06, p < 0.0001). OR: odds ratio; CI: confidence interval.
Mean CRP and wound healing for fractures at 1 month (n = 274).
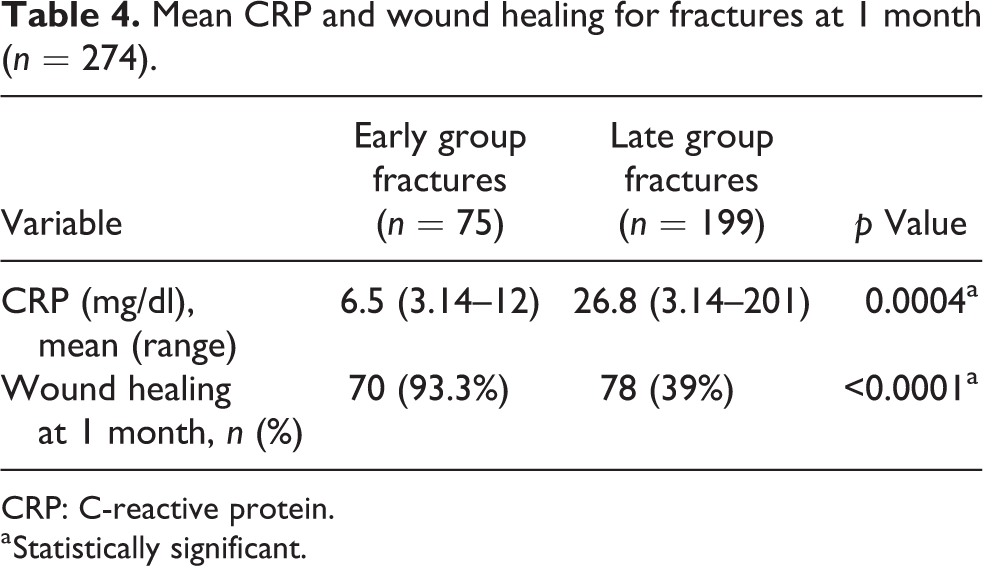
CRP: C-reactive protein.
a Statistically significant.
Finally, the patients’ quality of life was assessed. The functional outcome was assessed using the SMFA and SF-36 physical component score and mental component score in only the patients whose fractures had united at the end of 9 months. There were a total of 148 patients with 175 fractures that had united at the end of 9 months. We excluded 12 patients who had severe head injuries (4 in the early and 8 in the late group). The results for functional outcomes in 136 patients are listed in Table 5. The early group had a higher functional outcome score than the late group, which was statistically significant. The differences in the mean number of readmissions per patient, duration of hospital stay, number of additional surgeries required per patient, in-patient bill per patient, major complications, and return to work percentile of patients at the end of 9 months for the early and late debridement group are provided in Table 6. The number of readmissions per patient was significantly higher in the late group (p = 0.001). Although there was no statistically significant difference in the overall number of additional surgeries per patient in both groups, the number of patients who underwent at least two or more surgeries was significantly higher in the late group (p = 0.01). The incidence of major complications (amputations and deaths) was 7% in the late group. None of the patients in the early debridement group had any major complications. Further, the overall return to work percentile of patients was higher in the early group (p < 0.0001). No statistical difference was noted in the duration of hospital stay and mean total cost expenditure per patient between the early and late groups.
Comparison of the mean SMFA (DI and BI) and SF-36 PCS and MCS between the early and late groups for 136 patients at 9 months (n = 136).

DI: dysfunction index; BI: bothersome index; SF-36: short form-36; PCS: physical component score; MCS: mental component score.
a Statistically significant.
Readmissions, duration of stay, additional surgeries, cost, major complications, and return to work (early vs. late group patients; n = 231).
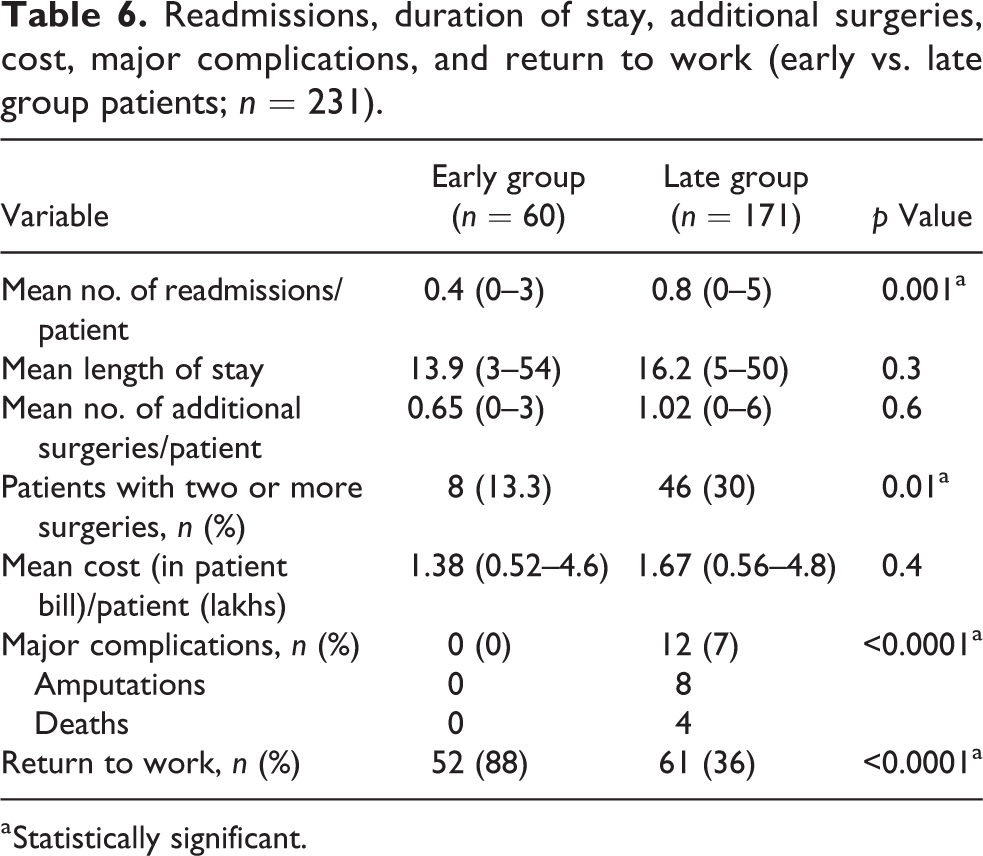
a Statistically significant.
The predominant surgeries were serial wound debridement for infections in the late group and redo fixations (conversions from temporary external fixation to definitive fixation) in the early group. No difference was observed in the number of patients, who underwent bone grafting, with or without redo-fixation in both the groups. Soft tissue procedures included vascular repairs, flaps, and skin grafting, which were comparable in both groups.
Discussion
The recent literature has shown no apparent association between time to debridement and the development of complications in open fractures. 1 –3,8,23 However, these studies were all conducted in the west, where the incidence, setting, and mechanism of injuries is completely different. In developing countries, where the overall percentage of open fractures and motor vehicle accidents is considerably higher, 6,9,23,28 –31 the lack of protective clothing worn by motorcyclists combined with dirty roads predispose the injured limb to considerably higher degrees of contamination. In addition, the setting in a hot tropical climate provides a favorable medium for bacterial colonization.
Enninghorst et al. showed that a timely debridement within 8 h led to a good outcome, with an overall low infection rate of 17% in a prospective study on 89 open tibia fractures. 11 Our study is in agreement with this, however, in a different setting with a more varied time to presentation and debridement and has a larger database, which includes femoral fractures as well. Most studies have focused on infection rates rather than nonunion in open fractures. 1 –4 Westgeest reported a nonunion rate of 17% in a prospective analysis of 736 open fractures. 5 However, they collected data through telephonic interviews and from clinical records and reported a 13% discrepancy in patient- and surgeon-reported outcomes. Studies analyzing infection rates appear to be retrospective in nature, with the exception of a few. 1,4 Although the overall infection rate was lower in most of these studies, Pollak et al., in their prospective study, reported infection rates that were comparable to those observed in our study. 1 However, in their study, no association was observed between time to debridement and infections.
Our study is limited by a follow-up period of 9 months because all the patients were not followed up until fracture union. However, taking into account the FDA accepted criteria of a maximum waiting time of 9 months, this period seemed reasonable. In the direct cost analysis, only the in-patient bill was evaluated and not the individual pharmaceutical drug expenditure. Further, considering that a significantly higher number of patients in the late group had not returned to work at 9 months, an indirect cost analysis that included wages lost and transportation costs borne for hospital visits may have added to the economic impact of late debridement.
The strengths of our study included its prospective nature and the clinical follow-up of all the patients. We only included high-grade long bone lower limb fractures for a standardized comparison. Furthermore, fracture union was confirmed by a group of four senior consultants at the end of 9 months, who were blinded to the study outcomes. Our study also assessed the functional outcome of the patients. We found that even when the fractures had united, the functional scoring of the patients in the early debridement group was significantly higher. This was probably due to pain and stiffness caused by the consequences of delayed debridement. A significantly higher percentage of the patients in the early group had returned to work at 9 months compared with those in the late group. This is of particular importance in our setting, considering that the majority of the patients were daily wage laborers.
The results of this study are in agreement with our hypothesis that time to debridement can exert a profound impact on fracture union, infection rates, and the overall quality of life. The study results also showed the dangers of applying conclusions regarding time to debridement without taking local conditions into account. Therefore, formulating region-based treatment protocols for early wound management may be beneficial in saving life, limbs, and money.
Conclusion
Thus, in developing countries, where transport of the injured by air is almost nonexistent, public health policy should mandate the formation of trauma centers throughout the country, with adequate facilities, so that time to debridement is cut down. At present, highly specialized centers exist in large cities in most of the world. These may not be sufficient for the needs of a country and transport to them may sometimes even take days. Timely debridement would result in saving life, limb, and money in these potentially physically devastating injuries with far-reaching social and economic consequences. This study showed that time to debridement in open high-grade lower limb fractures had a significant effect on union and infections. It is possible that these results may be extrapolated to grade 1 and 2 fractures, however, this requires further assessment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.