
Abstract
Introduction:
Mortality rates and causes of death after total knee arthroplasty (TKA) are of great interest to surgeons. However, there is a shortage of studies regarding those of the Asian population. The aim of this study was to compare the mortality rate and causes of death in patients after TKA to the general population.
Methods:
National sample cohort data from the Korean Health Insurance Review and Assessment Service were used. In this study, 1:4 matched patients after TKA (TKA group: 5072) and general participants (control group: 20,288) were selected as subjects. Their average follow-up duration was 57.2 months ranging from a year up to 12 years. The matches were processed for age, gender, income, region of residence, and past medical history. Mortality rates and causes of death were compared between groups. Regarding the mortality rates, we also performed subgroup analyses according to age.
Results:
Adjusted hazard ratio (HR) of the TKA group for mortality rate was less than 1 with significance (adjusted HR = 0.61 (95% confidence interval = 0.54–0.70, p < 0.001)). The ratios were less than 1 for both age groups (<70 and ≥70 years), respectively; however, for patients under 70, they were insignificant. Among the 11 major causes of death, the circulatory disease showed the most significantly reduced mortality rate for the TKA group compared to the control group. The neoplasm was the only other cause with a significantly reduced mortality rate for the TKA group.
Conclusion:
The mortality rate in the TKA group was significantly lower than in the control group up to 12 years after the surgery in Korea. Among the major causes of death, circulatory disease and neoplasm showed a significant reduction in the mortality rate of the TKA group compared with the control group.
Introduction
Total knee arthroplasty (TKA) is considered a very successful treatment for patients with end-stage knee arthritis. 1,2 However, because it is a major operation, life-threatening complications such as myocardial infarction, pulmonary embolism, and infection can occur after TKA. Numerous early mortality studies regarding these postoperative complications and comorbidities have been published. 3 –6 Even without these severe complications, immediate postoperative mortality rates usually increase due to surgical stress. 4,7 –9
Meanwhile, because TKA relieves knee pain, patients can increase their activities of daily living after recovering from TKA. Increased activity benefits the elderly and could affect their long-term mortality. Walking disability is a known major risk factor of death in knee osteoarthritis patients. 8,10 Long-term mortality of patients after TKA compared to the general population is of great interest to surgeons. Because data spanning 10 years or more are difficult to collect, there is a shortage of studies regarding this matter, which report inconsistent results. 11,12 Almost all such studies are from Western countries, most notably English and Scandinavian registries. Severe osteoarthritis is also prevalent in Asian populations, especially in women. Large population-based Asian cohort data would be beneficial and necessary to evaluate the long-term mortality after TKA in an Asian population.
Another topic of interest is the causes of death of patients after TKA compared to the general population. There are reports comparing mortality by each cause. 13,14 Cardiovascular disease (CVD) is a well-known problem associated with osteoarthritis due to impaired mobility. Because TKA relieves pain and improves walking ability, CVD-related events are reduced in TKA patients. 15,16 Furthermore, there are also reports that mortality due to CVD is reduced in TKA patients compared to the general population. 8 Additionally, whether the causes of death of patients after TKA differ from those of the general population has not been widely studied, especially in Asian populations.
The primary purpose of this study was to compare the long-term mortality rate of patients who underwent TKA to that of the general population (controls). The secondary purpose was to compare the causes of death of the two groups. In addition, regarding the mortality rate, we conducted subgroup analyses by dividing participants according to age (<70 vs. ≥70 years). The hypotheses were that the mortality rate in patients after TKA would be reduced compared to the general population and also CVD as the cause of death in patients after TKA would be less compared to the general population.
Materials and methods
Study population and data collection
This national cohort study relies on data from the Korean Health Insurance Review and Assessment Service (HIRA)–National Patient Sample. The Korean National Health Insurance Service (NHIS) selects samples directly from the entire population database to prevent nonsampling errors. Approximately 2% of the samples were selected from the entire Korean population (50 million). These selected data can be classified at 1476 levels (age (18 categories), gender (2 categories), and income level (41 categories)) using randomized stratified systematic sampling methods via proportional allocation to represent the entire population. After data selection, the appropriateness of the sample was verified by a statistician, who compared the data from the entire Korean population to the sample data. The details of the methods used to perform these procedures are provided by the National Health Insurance Sharing Service. This cohort database included (i) personal information, (ii) health insurance claim codes (procedures and prescriptions), (iii) diagnostic codes using the International Classification of Disease-10 (ICD-10), (iv) death records from the Korean National Statistical Office (using the Korean Standard Classification of disease), (v) socioeconomic data (residence and income), and (vi) medical examination data for each participant over a period ranging from 2002 to 2013.
Because all Korean citizens are recognized by a 13-digit resident registration number from birth to death, exact population statistics can be determined using this database. It is mandatory for all Koreans to enroll in the NHIS. All Korean hospitals and clinics use the 13-digit resident registration number to register individual patients in the medical insurance system. Therefore, the risk of overlapping medical records is minimal, even if a patient moves from one place to another. Moreover, all medical treatments in Korea can be tracked without exception using the HIRA system. In Korea, notice of death to an administrative entity is legally required before a funeral can be held. The causes of death and date are recorded by medical doctors on a death certificate.
Participant selection
Of the 1,025,340 cases with 114,369,638 medical claim codes, we included participants who underwent TKA (claim code: N0712 or N2072) for osteoarthritis of knee (ICD-10 code: (M170-M179)). From January 2002 through December 2012, 5088 participants were selected. We excluded the participants who were younger than 40 years old (n = 2). The participant who underwent TKA were matched 1:4 with the participants (control group) who never underwent arthroplasty from 2002 through 2013 among this cohort. The matches were processed for age, gender, income group, region of residence, and past medical history (hypertension, diabetes, and dyslipidemia). To prevent selection bias when selecting the matched participants, the control group participants were sorted using a random number order, and they were then selected from top to bottom. It was assumed that the matched control participants were involved at the same time of each matched TKA participants (index date). Therefore, the control participants who died before the involvement time of the matched index date were excluded. TKA participants for whom we could not identify enough matching participants were excluded (n = 14). Finally, 1:4 matching resulted in the inclusion of 5072 of TKA participants and 20,288 control participants (Figure 1).
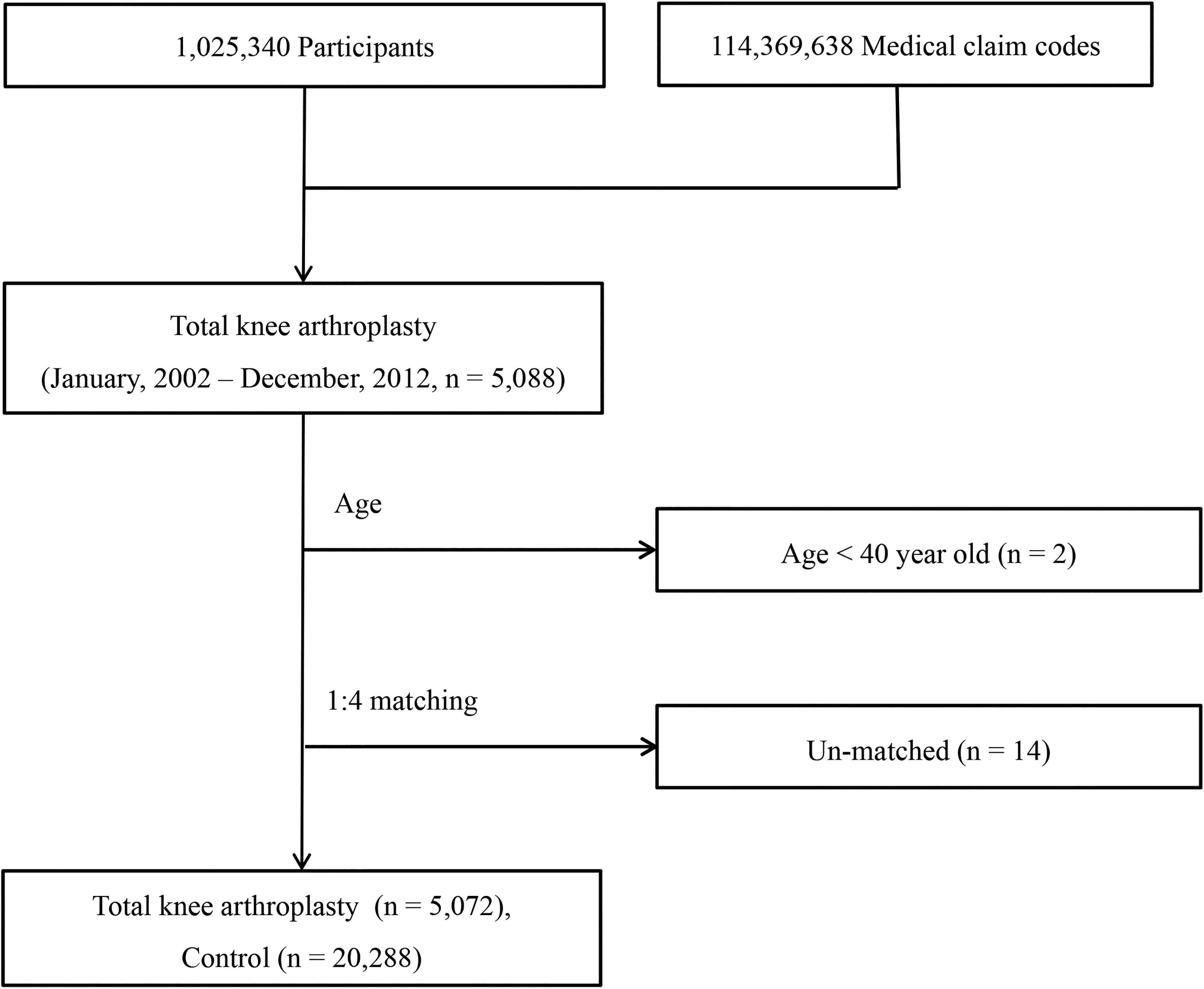
A schematic illustration of the participant selection process.
Variables
Age groups were stratified using 5-year intervals. We selected 10 age groups (40–44, 45–49,…, and 85 and above). The income groups were initially divided into 41 classes (one health aid class, 20 self-employment health insurance classes, and 20 employment health insurance classes). These groups were recategorized into 11 classes (class 1 (lowest income)–11 (highest income)). Region of residence was divided into 16 areas according to administrative district. These regions were regrouped into urban (Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, and Ulsan) and rural (Gyeonggi, Gangwon, Chungcheongbuk, Chungcheongnam, Jeollabuk, Jeollanam, Gyeongsangbuk, Gyeongsangnam, and Jeju) areas.
The causes of death were classified following Korean standard classification of diseases (KCD), which was developed based on the International Statistical Classification of Diseases and Related Health Problems (ICD) by the World Health Organization.
17
Therefore, the causes of death were categorized into 11 classifications. We added one extra (others), which had limited number of participants: infection (certain infections and parasitic diseases, A00–B99); neoplasm (neoplasm, C00–D48); metabolic disease (endocrine, nutritional, and metabolic diseases, E00–E90); mental disease (mental and behavioral disorders, F00–F99); neurological disease (diseases of the nervous system, G00–G99); circulatory disease (diseases of the circulatory system, I00–I99); respiratory disease (diseases of the respiratory system, J00–J99); digestive disease (diseases of the digestive system, K00–K93); muscular disease (diseases of the musculoskeletal system and connective tissue, M00–M99); genitourinary disease (diseases of the genitourinary system, N00–N99); trauma (injury, poisoning, and certain other consequences of external causes, S00–T98); others (diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism, D50–D89; diseases of the skin and subcutaneous tissue, L00–L99; abnormal finding symptoms, signs, and abnormal clinical and laboratory findings, NEC, R00–R99).
The past medical history of participants was evaluated using ICD-10 codes. For accurate diagnosis, hypertension (I10 and I15), diabetes mellitus (E10–E14), and dyslipidemia (E78) were searched if the participants were dealt with ≥2 times.
Statistical analysis
The χ 2 test (categories with a value number ≥5) or Fisher’s exact test (categories with a value number <5) was used to compare the mortality rate between the TKA group and the control group (all of death, and each of causes of death). Odd ratios and 95% confidence intervals were calculated. In this analysis, because we compared the multiple causes of death, we adjusted the threshold of p value using the false discovery rate to avoid type I error.
To analyze the cumulative survival rate of the TKA and control groups, Kaplan–Meier survival analysis was used. To analyze the hazard ratio (HR) of TKA on mortality, Cox-proportional hazard model was used. In this analysis, adjusted (age, gender, income, region of residence, hypertension, diabetes, and dyslipidemia) model was used. Two-tailed analyses were conducted, and p values <0.05 were considered to indicate significance. The results were statistically analyzed using SPSS v. 21.0 (IBM, Armonk, New York, USA).
Results
Baseline characteristics
Age, gender, income, region of residence, and past medical history (hypertension, diabetes, and dyslipidemia) were matched between the groups (Table 1).
General characteristics of participants.a

TKA: total knee arthroplasty.
a χ 2 test, significance at p < 0.05.
Mortality rate
The mortality rate in the TKA group was significantly lower than the control group with a 12-year maximum and a 1-year minimum follow-up (follow-up: TKA group—mean 58.1 months, median 52.0 months; control group—mean 57.0 months, median 50.0 months; Figure 2 and Table 2). In the subgroup analyses, although the HRs were less than 1 for both under 70 and 70 or above participants, only the 70 or above participants group showed significance (Table 3).

Kaplan–Meier survival curves according to the group.
Adjusted hazard ratios (95% confidence interval) of total knee arthroplasty for mortality.

a Adjusted model for age, sex, income, region of residence, hypertension, diabetes, and dyslipidemia history.
bCox-proportional hazard regression model, significance at p < 0.05.
Adjusted hazard ratios (95% confidence interval) of total knee arthroplasty for mortality according to age group.
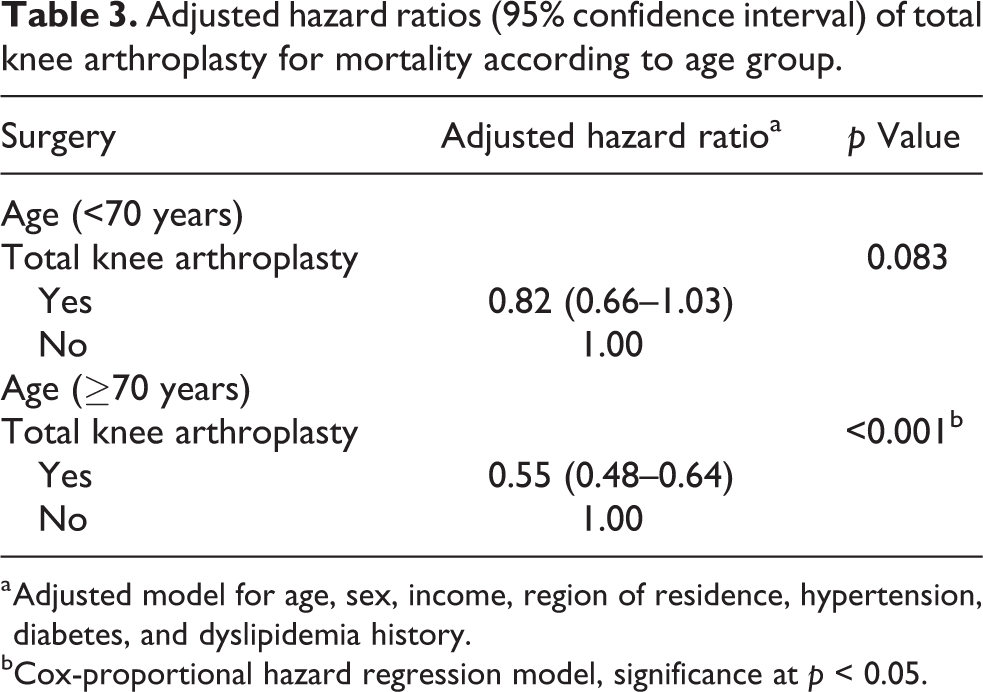
a Adjusted model for age, sex, income, region of residence, hypertension, diabetes, and dyslipidemia history.
bCox-proportional hazard regression model, significance at p < 0.05.
Cause of death
Among the 11 major causes of death classified following the KCD, circulatory disease showed the most significant difference between the TKA group and the control group. The only other cause that showed significantly lower rate in the TKA group was neoplasm. These two causes were also two of the most common causes of death in both the TKA group (1.3% and 1.7%, respectively) and the control group (2.6% and 2.3%, respectively) (Table 4).
The difference of mortality rates between the TKA group and the control group according to the cause of death.

TKA: total knee arthroplasty; CI: confidence interval; SMR: standardized mortality ratio.
a χ 2 test (categories with a value number ≥5).
b Significance at false discovery rate adjusted: p < 0.05.
c Fisher’s exact test (categories with a value number <5).
Discussion
This study showed that after the adjustment for age, gender, income, regions of residence, and past medical history (hypertension, diabetes, and dyslipidemia), the mortality rate of patients after TKA was significantly reduced compared to that of the general population with a 12-year maximum and a 1-year minimum follow-up. Regarding age, while the mortality rate of TKA group was significantly reduced in the older population (≥70 years), the association was insignificant in the younger population (<70 years). Among the major causes of death, circulatory disease and neoplasm showed significant reductions in mortality of patients after TKA compared to the general population.
There have been some mid- to long-term large cohort studies from Western countries regarding mortality rates after TKA. Some of these studies reported lower mortality rates of patients after TKA compared to the general population, 8,11,18,19 while other studies reported higher mortality rates of patients after TKA. 3 In terms of Asian population, there is a recent article that reported no significant difference in long-term mortality rates between the TKA group and the general population with a mean follow-up period of 95 months. However, it was not a large cohort study. 20 Our study resulted in a lower mortality rate of patients after TKA up to a 12-year follow-up period, siding with the first group of studies. One previous study reported that younger patients aged <55 years had higher mortality and older patients aged >70 years had lower mortality rates than the general population up to 28-year follow-up. 21 Here, we had somewhat similar results that although both age groups (<70 and ≥70 years) showed lower mortality rates than the general population, only the older participants aged ≥70 years showed significantly reduced mortality rates than the general population.
CVD is a major cause of death. 8 The risk factors for CVD and knee osteoarthritis are similar. 10,22,23 Because TKA improves patient osteoarthritic status and walking ability, it is expected to possibly reduce long-term CVD-related mortality in patients after TKA. Nonetheless, controversy persists about whether there is really a protective effect of TKA against CVD-related mortality and how long it will last. 13,15 Lovald et al. reported that there was a reduction of newly diagnosed heart failure in the TKA group compared to the non-TKA group. 19 Here, we found that circulatory disease as the cause of death was significantly reduced in patients after TKA compared to the general population in up to a 12-year follow-up.
There are reports that TKA does not increase cancer risk. 8,24 Regarding cancer-related mortality, because advanced cancer would be a contraindication for TKA, there is a report of reduced cancer-related mortality after TKA. 13 In this study, although we did not have data about whether TKA reduces the incidence of cancer, cancer-related mortality was lower in patients after TKA than the general population. The preoperative screening and regular health supervision at follow-up could have eliminated cancer patients preoperatively and detected early cancers in these patients.
Pulmonary embolism is an early major complication and cause of death for patients after TKA. 25 Some reports stated that early mortality due to respiratory disease is increased in the early postoperative period. 4 However, regarding long-term mortality, reduced mortality rates were also reported, 13 and our study also showed reduced mortality rate in terms of respiratory disease after TKA, although without significance.
Some of the authors insisted that the “healthy patient” effect affects the long-term reduced mortality after TKA. Preoperatively, because patients with severe comorbidities were usually excluded from TKA, only those with acceptable comorbidities underwent TKA, which led to reduced mortality compared to the general population. 7,8,11 Furthermore, patients received increased medical care after TKA and could have been treated properly at the early stage of disease progression, which also could explain the reduced mortality after TKA. 9 Today, almost all patients after TKA receive some kind of prophylaxis for the aforementioned complications and are monitored regularly. In this study, we tried to minimize this “healthy patient effect” by matching basic past medical history between the groups.
To the best of our knowledge, this study is the first long-term large cohort study to evaluate mortality and cause of death in patients after TKA in Korea (Asian population). There were some long-term studies regarding mortality after TKA, but they were not cohort studies. 20 Since we used data from HIRA, which include data from all citizens of Korea, we did not miss any participants due to follow-up loss. Therefore, the strength of this study lies in the results accurately representing the entire Korean population. Furthermore, we matched not only age and gender but also socioeconomic status (income and regions of residence) of the two groups. Matching some of the past medical history (hypertension, diabetes, and dyslipidemia) also strengthened our results.
There were several limitations to this study. We used health insurance claim data; hence, there could be some inaccuracies within the data and results. Such inaccuracies are inevitable with large cohort databases like NHIS; however, due to the large data set, it is still meaningful if handled correctly. Second, we compared the causes of death of the two groups, not the incidences of these diseases. Therefore, we do not have data regarding the long-term effect of TKA on these diseases. Third, we did not evaluate any clinical scores after TKA in this study. The clinical results of surgery could certainly affect the mortality, but there was no way to assess those using these data. Fourth, rehabilitation after surgery is another important factor for the consequences including mortality after TKA. However, because this is a study using a very large national cohort data including every hospital and medical center in South Korea, and there is no specific national guideline for rehabilitation protocol after TKA, it was not possible to state a certain rehabilitation protocol after TKA. Fifth, the control group of this study was the general population, not knee osteoarthritis patients who did not receive TKA. There could be arguments to check the sole effect of TKA (surgery) itself to the mortality rate and cause of death, it is better to include only the knee osteoarthritis patients who did not receive TKA in the control group. However, TKA is usually performed to the knee osteoarthritis patients with severe symptoms. Knee osteoarthritis patients who did not receive TKA probably have minimal symptoms or other morbidities that prevent them from having TKA. Therefore, including only those patients in the control group could also bias the results in an unintended way. Furthermore, there have been more studies comparing the mortality rate in TKA patients to the general population than the knee osteoarthritis patients who did not receive TKA. Lastly, because most of the participants were female (at an almost 8:1 ratio to male participants), we did not differentiate between male and female data.
Conclusion
The mortality rate in the TKA group was significantly lower than in the control group with a 12-year maximum and a 1-year minimum follow-up in Korea. Regarding age, while the mortality rate in the TKA group was significantly reduced in the older population (≥70 years), the association was insignificant in the younger population (<70 years). Among the major causes of death classified following KCD, circulatory disease and neoplasm showed significant reductions in mortality of patients after TKA compared to the general population. This study supports TKA as a safe treatment option for end-stage knee arthritis. Patients can have longer life expectancy with TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a research grant [NRF-2015-R1D1A1A01060860] from the National Research Foundation (NRF) of Korea.
Informed consent
The ethics committee of Hallym University approved this study (2014-I148). Written informed consent was exempted by the Institutional Review Board.