
Abstract
Hip abductor deficiency is most commonly encountered in the context of degeneration of the hip, and techniques for reconstruction pioneered by arthroplasty surgeons. We adopted a local muscle transfer technique utilizing the anterior half of the gluteus maximus for abductor reconstruction following soft tissue tumour excision in a young female patient. The patient of concern had a solitary fibrous tumour located between the right gluteus medius and minimus detected as an incidental finding. Marginal excision of the mass resulted in removal of the gluteus medius. The anterior half of the gluteus maximus was transferred and attached to the decorticated lateral greater trochanter by means of suture anchors and transosseous sutures. The patient initially demonstrated a Trendelenburg gait and limited abduction against gravity. By 1-year post-operation, there was return of normal gait and recovery of hip abductor power. This is the first report of anterior gluteus maximus transfer being successfully applied for soft tissue reconstruction around the hip subsequent to tumour excision.
Case presentation
The patient was a 43-year-old female initially presenting in September 2016 to the general practitioner with menorrhagia and dysmenorrhoea associated with abdominal pain for 2 weeks. She worked as a helper at an elderly home and enjoyed running and hiking for recreation. An abdominal mass was palpable over the lower abdomen, and the patient was subsequently referred to the gynaecologist for further workup. Clinical examination by the gynaecologist demonstrated a mobile pelvic mass corresponding to 18-weeks gestation in size, more palpable towards the right of the abdomen.
Transabdominal and transvaginal ultrasound performed at the clinic demonstrated bilateral adnexal masses, measuring 8.6 × 8.0 cm over the left side, and 7.3 × 5.6 cm on the right side with hyperechoic spots and a tramline appearance. A subsequent contrast computed tomography scan of the bilateral adnexal masses demonstrated soft tissue densities together with calcifications, which was suggestive of bilateral dermoid cysts. Additionally, there was an incidental finding of an elliptical mass measuring 2.5 × 4.4 × 5.7 cm over the right buttock, appearing to arise in the intermuscular plane between the right gluteus minimus and gluteus medius, with peripheral contrast enhancement (Figure 1).

Contrast CT at level of hip, axial cuts proceeding from cranial to caudal, demonstrating contrast-enhancing tumour (white arrow) over right gluteal region. CT: computed tomography.
In regards to the patient’s bilateral adnexal masses, she received laparotomy together with right sided salphigoophorectomy and left sided ovarian cystectomy in June 2017. Definitive histology was that of bilateral dermoid cysts without features of malignancy. For the buttock mass, she was referred to orthopaedics for evaluation, with a contrast magnetic resonance imaging (MRI) performed during the interim period for further soft tissue evaluation. The mass was T1 hypointense and heterogeneously hyperintense on T2 imaging together with contrast enhancement, with both axial (Figure 2) and coronal (Figure 3) T1 contrast images shown. Again it appeared to arise between the gluteus medius and minimus, with compression of the overlying gluteus medius. Upon history taking, she was unaware of a mass over her right buttock and the area was asymptomatic without pain or tenderness. She did not exhibit any constitutional signs or symptoms. On physical exam, no palpable mass was detected over the right buttock and there were no enlarged inguinal lymph nodes.
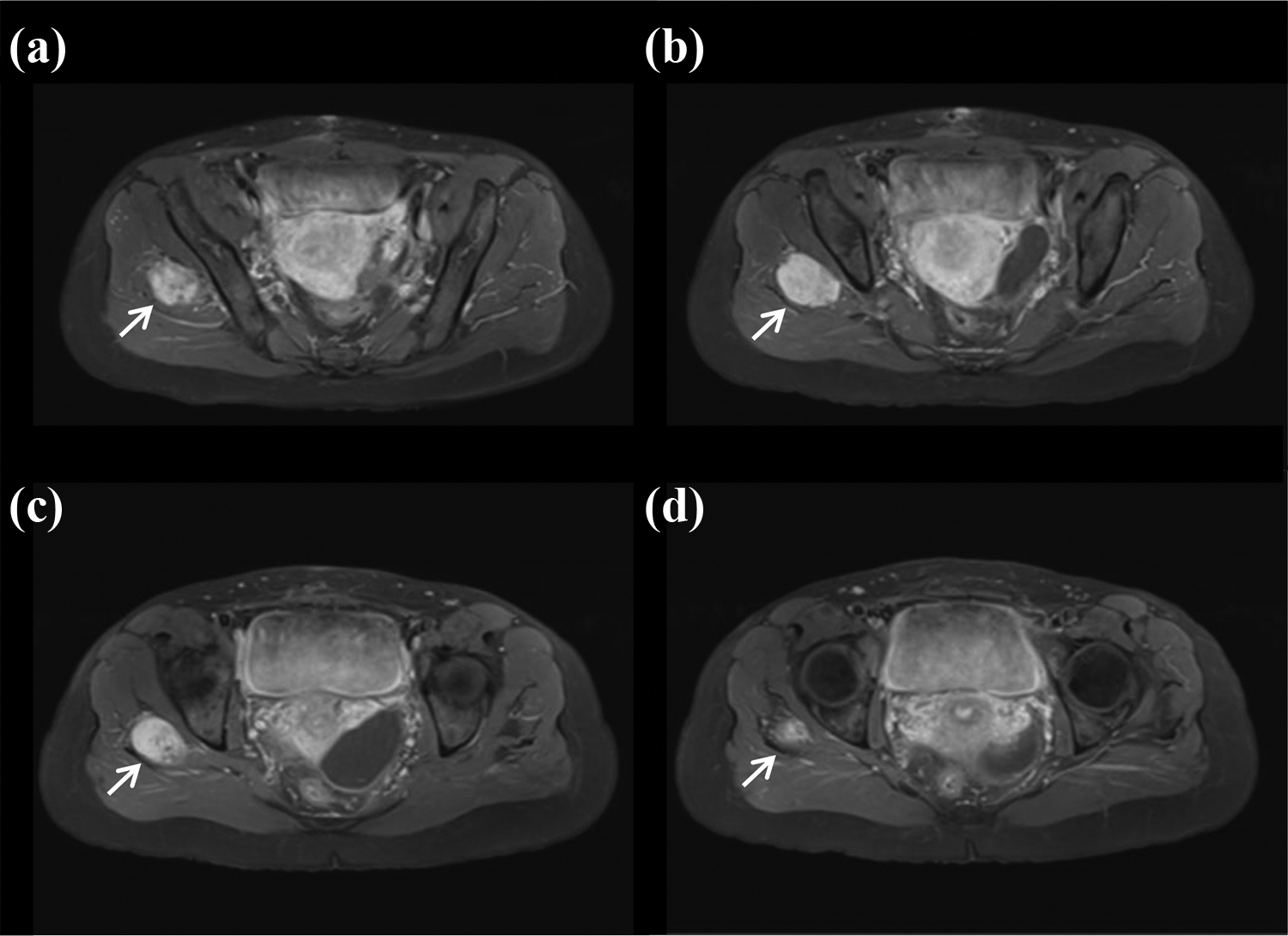
T1 contrast MRI at level of hip, axial cuts proceeding from cranial to caudal. There is displacement of the overlying gluteus medius as a result of compression by the soft tissue tumour (white arrow). MRI: magnetic resonance imaging.

T1 contrast MRI at level of hip, coronal cuts proceeding from anterior to posterior with tumour highlighted (white arrow). MRI: magnetic resonance imaging.
Due to the uncertain diagnosis of the soft tissue mass, an ultrasound-guided trucut biopsy of the right buttock mass was performed. The histopathology section demonstrated alternating hypercellular and hypocellular fibrous areas. The hypercellular areas comprised a patternless arrangement of spindle cells with uniform ovoid nuclei, vesicular chromatin and occasional small distinct nucleoli. Mitotic figures were inconspicuous. Immunohistochemical staining showed that tumour cells were positive for CD34, CD99 and Bcl2 while S100, SMA, desmin, MNF116, EMA and ALK were negative. These findings were consistent with the diagnosis of a solitary fibrous tumour. The patient was counselled and expressed her desire to return to work at the old age home, which involved moderate manual labour. The management plan was for mass excision together with abductor reconstruction.
The patient received marginal excision together with abductor reconstruction in March 2018. She was placed in a lateral position with a posterolateral approach to the hip proceeding from the gluteus maximus down towards the tensor fascia lata centred upon the tumour mass (Figure 4(a)). The superficial biopsy tract was removed and traced from superficial to deep between the anterior and posterior halves of the gluteus maximus. The reconstruction method was based on that described by Whiteside. 1,2

Intraoperative photos. (a) Surface markings of the planned incision, prior biopsy site, and GT. (b) Exposed GMax with anterior half as well as GT demarcated. (c) Elevated anterior half of GMax with marginal excision of tumour together with GMed shown beneath. The TFL is also seen. (d) Passage of three rows of fiberwires over the GMax followed by (e) drilling of transosseous tunnels through the lateral GT. (f) Appearance of completed transfer with anterior half of GMax secured over the lateral GT. GT: greater trochanter; GMax: gluteus maximus; GMed: gluteus medius; TFL: tensor fascia lata.
The anterior half of the gluteus maximus was fashioned as a triangular flap (Figure 4(b)) for transfer as well as exposure following release from the tensor fascia lata. With the tumour exposed beneath, marginal excision was performed with the bulk of gluteus medius consequently removed while the gluteus minimus was preserved (Figure 4(c)). Course of the sciatic nerve was palpated to prevent injury but not exposed. Clinically the excised mass (Figure 5(a)) measured 6 cm in diameter and was hard on palpation. To visualize the lateral surface of the greater trochanter, 2 cm from the proximal origin of the vastus lateralis was released. Subsequently the lateral greater trochanter was decorticated, and the distal gluteus maximus flap anchored to it using G2 Mitek sutures reinforced by three rows of transosseous fibrewire sutures (Figure 4(d) to (f)). For closure, the vastus lateralis was closed over the flap and distal tensor fascia lata apposed, followed by subcutaneous and skin closure. The patient was given an abduction pillow in the early post-op period until drain removal, followed by a hip abduction spica brace for 6-weeks. In regards to the rehabilitation protocol to her right lower limb, she was prescribed 6-weeks of toe-touch-down weight bearing, then 50% partial-weight bearing without the abduction brace together with assisted active abduction exercise without gravity from 6 to 12 weeks post-op, proceeding to 75% weight bearing with elbow crutches and active abduction against gravity from 12 to 18 weeks, followed by full-weight bearing from 18 weeks onwards. This was adopted from the post-op protocol of a related case series 2 to enable sufficient time for soft tissue to bony healing before loading. Histopathology of the excised specimen was consistent with that of a solitary fibrous tumour. High cellularity, marked pleomorphism and necrosis, was not observed. All margins were free of tumour involvement. Following clinicopathological conference review, surgical excision was deemed to be definitive with no need for adjuvant therapy.
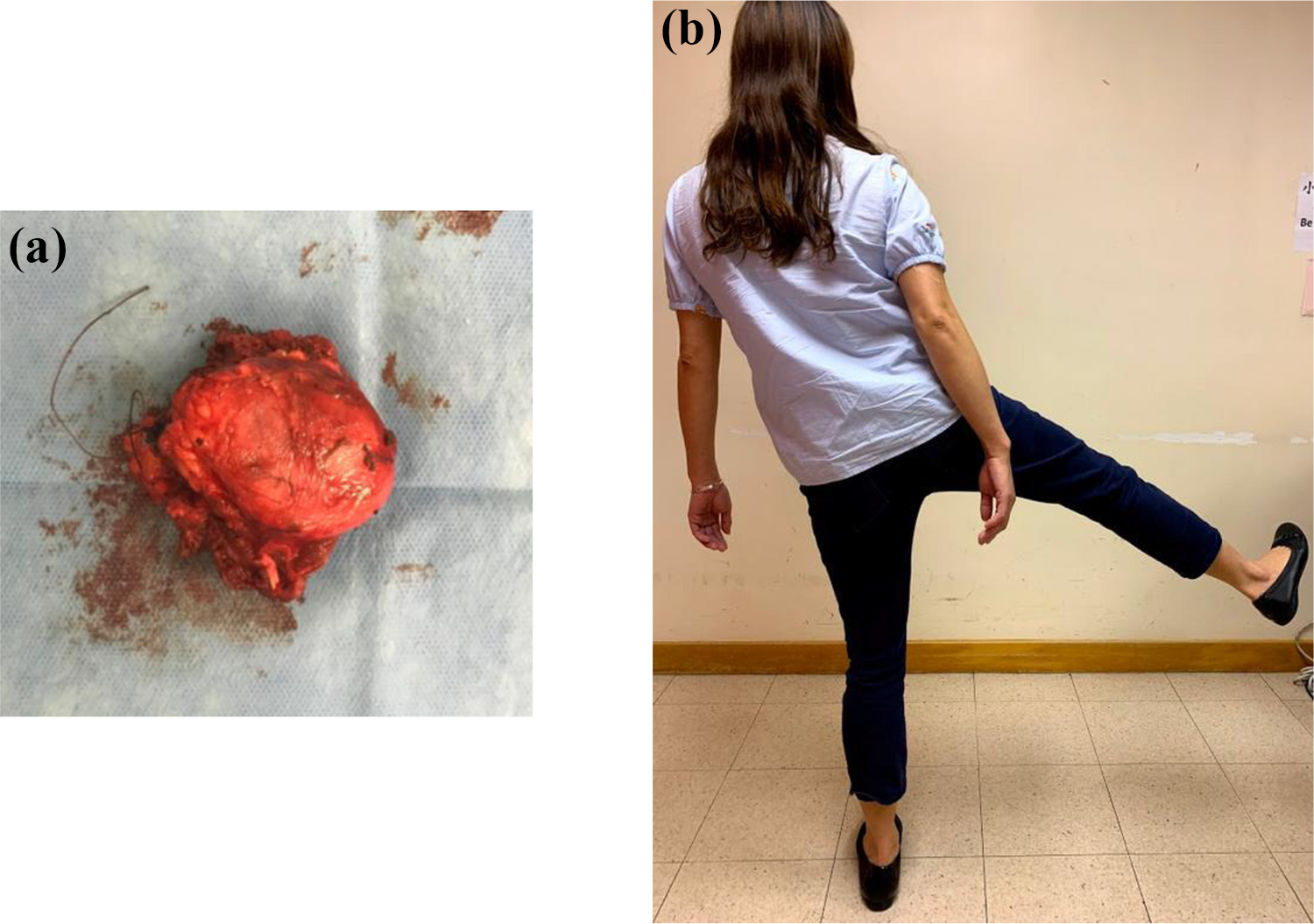
(a) Surgical specimen following marginal excision of solitary fibrous tumour. The excised mass was 6 cm in diameter, with the tumour proper measuring 5 × 5 × 2 cm on gross pathological examination. The margins were clear. (b) Active abduction against gravity of the right lower limb at 1-year post reconstruction.
The patient’s rehabilitation progress was monitored at the outpatient clinic. There were no wound-related complications. Trendelenberg gait was still noted at 5-month post-op, and she required a stick for walking. By 8 months, she could walk unaided, with post-op improvement in abductor power and a visibly less apparent Trendelenburg gait. By 1-year post-op, she was walking with a normal gait and had 5 of 5 right hip abductor power. Demonstration of active abduction against gravity is demonstrated in Figure 5(b) with the patient standing. As of her latest follow-up at 15-month post-op, she had no complaints apart from some soreness over the right buttock after prolonged walking and heavy lifting. She was regularly swimming 3–4 times per week. There were no local signs of recurrence. She will be monitored by means of clinical palpation and regular MRI imaging of the hip.
Discussion
Lachiewicz described three common clinical scenarios in which abductor deficiency is encountered, 3 which can be divided into (1) chronic non-traumatic tears affecting the anterior fibres of the gluteus medius tendon, often in the elderly and thus termed ‘rotator cuff tears of the hip’; (2) abductor tendon tears identified during hip surgery for arthroplasty or fracture; and (3) tendon avulsion after total hip arthroplasty performed through an anterolateral or transgluteal approach. Patients present with weakness and may have a pathological Trendelenburg gait. There is often associated lateral hip pain and tenderness. Prevalence of abductor compromise as determined intraoperatively was determined to be near 20% in patients receiving primary total hip arthroplasty. 4 On the contrary, there are few reports of abductor complex attenuation as result of tumour infiltration or resection. Literature in regards to the prevalence and management of abductor deficiency has therefore been spearheaded by arthroplasty surgeons, where recovery of abductor function is all the more pertinent as there is the subsequent risk of recurrent dislocation.
Direct repair is an option to address abductor deficiency, 4,5 but with only half of patients demonstrating a marked reduction in limp, these results appear to be inferior to that described following grafting and muscle transfers. Direct repair is also unlikely to be feasible when there is significant retraction, atrophy, or surgical removal of the abductors as in our case. Subsequent to this, there have been reports of augmentation. Fehm described utilization of an Achilles tendon allograft to address abductor deficiency secondary to total hip arthroplasty, 6 utilizing wire cerclage to secure the allograft calcaneal bone plug inside a greater trochanter recess, while the proximal widened portion of the tendon graft was sutured to the intact portion of the gluteus medius. Similarly, Rao et al. described using allografts derived from acellular human dermal matrix to address avulsions to the abductor mechanism in patients previously receiving total hip arthroplasty. 7 In this case series, 11 of 12 patients had recovery of abductor power to 4 of 5, and all had improvement in gait.
Local muscle transfers have been described with success. Kohl described proximal mobilization of the vastus lateralis together with its neurovascular pedicle and subsequent suturing to the abductor remnant, 8 a technique which may be limited to shorter gap sizes. This was used to primarily address cases with abductor deficiency subsequently to osteoarthritis and revision arthroplasty, but also included a case of proximal femur resection subsequent to osteomyelitis, and greater trochanter resection resultant from bony metastasis. We however adapted the method described by Whiteside who described transfer of the anterior gluteus maximus alone 1 and subsequently in conjunction with the tensor fascia lata 2 followed by attachment to the greater trochanter. In regards to the latter approach, cadaveric studies determined that the anterior gluteus maximus and tensor fascia lata are biomechanically well positioned to mimic gluteus medius and gluteus minimus respectively following transfer. Subsequently five patients received transfer followed by fixation utilizing suture placement through multiple drill holes created in the decorticated lateral portion of the greater trochanter. These patients demonstrated the capacity for abduction against gravity at 3 months and resolution of the Trendelenburg gait at 1 year with the exception of one patient who fell at 10-month post-op with a subsequent greater trochanter avulsion fracture. Ries replicated Whiteside’s technique in 11 patients 9 by means of transposition alone or together with open reduction internal fixation of the greater trochanter, to tackle abductor deficiency as a result of soft tissue attenuation or together with bony avulsion respectively during revision hip arthroplasty. All 11 patients could actively abduct the hip at 3-month post-op and only 1 of 11 patients had a residual limp at 1-year post-op.
We decided upon transfer of the gluteus maximus only. Conveniently the gluteus maximus required exposure and elevation as part of the surgical exposure required for tumour excision, while the tensor fascia lata was located away from the tumour. Despite an intact gluteus minimus, utilization of the gluteus maximus for transfer alone may also be insufficient in reproducing the muscle bulk and direction of pull from the broad fan-shaped origin of the gluteus medius along the iliac crest 3 and in particular from the anterior fibres which are vertical in orientation and function as the main pelvic rotators. Therefore, in comparison to results attained in combination with tensor fascia lata transfer, return of active abduction against gravity was delayed. Nevertheless, subsequent to follow-up our patient demonstrated good functional outcome and satisfaction, being able to walk unaided by 8 months and with a normal gait by 1-year post-op. Finally, free flap reconstruction has also been described utilizing the latissimus dorsi, 10 but associated with greater technical difficulty and donor site morbidity
Our present case is the first among existing literature utilizing gluteus maximus transfer for reconstruction following primary soft tissue tumour excision. The series described by Kohl did include one case of muscle transfer following excision of the greater trochanter for the management of bony metastasis. Reconstruction in the context of proximal femur resection for primary bone tumours have used similar techniques to address soft tissue deficit to those described, such as allograft and mesh repair. 11 Solitary fibrous tumours are submesothelial in origin and have variable malignant potential, with about 10% located over the buttock area. 12 Our case illustrates that techniques for abductor complex reconstruction derived from joint arthroplasty and its associated complications can be applied following soft tissue tumour excision with good results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.