
Abstract
Purpose:
The actual incidence of deep vein thrombosis (DVT) in femoral neck fractures is underestimated. This study aimed to investigate the incidence of DVT in the lower extremities after femoral neck fracture before and after operation.
Methods:
The clinical data of patients with femoral neck fractures treated at Xi’an Honghui Hospital between July 1, 2016, and December 31, 2018, were collected. The patients were examined with ultrasonography before and after operation and divided into thrombosis and non-thrombosis groups according to their ultrasonographic results. The incidence of DVT was reported as a percentage.
Results:
The incidence rates of preoperative and postoperative DVT were 32% and 56%, respectively. DVT on the uninjured side constituted 45% of all preoperative DVT and 43% of all postoperative DVT. Peripheral DVT constituted 90% and 84% of all preoperative and postoperative DVT, respectively. Diabetes was an independent risk factor of preoperative DVT. Blood loss was an independent risk factor of postoperative DVT, and open reduction and internal fixation surgical procedure was independent protective factor of postoperative DVT as compared with hemiarthroplasty and total hip replacement.
Conclusions:
The incidence rates of preoperative and postoperative DVT in the patients with femoral neck fracture were high, and orthopedists should pay more attention to DVT as a complication.
Keywords
Introduction
In recent years, the incidence of femoral neck fractures has significantly increased with the growth of the aging population. 1 Owing to trauma itself, immobilization, advanced age, and comorbidity, some patients experience perioperative complications. Deep vein thrombosis (DVT) of the lower extremities is one of the common complications in these patients, 2 which is a high risk of fatal pulmonary embolism in some patients. 3 Traditionally, chemical 4 and mechanical thromboprophylaxes 5 are well-established routines in the prevent and treatment of DVT.
The incidence of DVT has been considered low in Asia, 6 but the data are based on the general population, not the patients suffered fractures. As for femoral neck fractures, the incidence of DVT is reported to range from 2.6% 2 to 19.5%. 7 However, we consider the actual incidence of DVT after femoral neck fracture is underestimated.
Firstly, asymptomatic DVT is often ignored in previous studies, which carries a similar risk of symptomatic DVT but not enough to be paid more attention. Sun et al. reported that asymptomatic DVT accounts for approximately 75% of all DVT cases. 8 Other studies have reported that all DVT were clinically asymptomatic. 9,10 Secondly, other studies did not examine the uninjured extremity, 11 thereby possibly missing DVT on the uninjured side, which has been shown to occur. 12 Decker and Weaver demonstrated that DVT could occur in both the injured and uninjured legs with a trend for higher incidence rates in the injured leg. 12 Thirdly, because of the risk for these elderly patients of complications, it should be striving for hip fracture patients to the operating room in modern fracture units by 24–36 h. However, that is not the norm in China where it takes several days to get a hip fracture patient to operating room so the incidence of DVT may be much higher.
On the basis of these factors, this study aimed to investigate the incidences rates of DVT in the lower extremities after femoral neck fracture before and after operation in this retrospective observational study conducted at a single institution.
Methods
Ethical statement
This study retrospectively analyzed the data of patients with femoral neck fractures who were admitted between July 1, 2016, and December 31, 2018, in Xi’an Honghui Hospital. The study was approved by the ethics review board of Xi’an Jiaotong University (no. 2014026).
Patient inclusion and exclusion criteria
The inclusion criteria were as follows: (a) age of ≥16 years, (b) fresh isolated femoral neck fractures that require surgical treatment, and (c) availability of preoperative and postoperative ultrasonography results. We excluded patients with femoral neck fractures with delayed treatment, serious medical problems that make surgery intolerable, and poor compliance.
Treatment
All the patients with femoral neck fractures were assessed for thromboembolism risk using the Risk Assessment Profile for Thromboembolism score upon hospital admission. For the patients without contraindications, low-molecular-weight heparin (LMWH; 3800 IU/0.4 mL, once per day; Fraxiparine, Glaxo Wellcome Production, GlaxoSmithKline) was subcutaneously injected to prevent DVT, according to the guidelines. 13 The anticoagulant therapy was discontinued 12 h before operation and resumed 24 h after operation. In addition, a mechanical pressure pump (20 min, twice per day) was used to promote blood reflux. Doppler ultrasonography was used to diagnose DVT, and vascular ultrasonography with a bedside machine was performed by three trained operators. The diagnostic criterion of fresh thrombosis was the presence of a constant intraluminal filling defect. 14 All the patients received an examination in both lower limbs 1 day before the planned surgery and on the third to fifth day after the operation.
The patients were divided into thrombosis and non-thrombosis groups according to their ultrasonography results. In addition, DVT was classified into central (femoral and iliac veins), peripheral (calf muscle, fibular, and anterior/posterior tibial veins), and mixed thrombosis (both central and peripheral thromboses). 15 For the patients without thrombosis, LMWH was continuously subcutaneously injected. For the patients with thrombosis, physicians from the department of vascular surgery prescribed the DVT treatment, and LMWH (3800 IU/0.4 mL, twice per day; Fraxiparine, Glaxo Wellcome Production, GlaxoSmithKline) was subcutaneously injected. If needed, an inferior vena cava (IVC) filter was used to prevent fatal pulmonary embolism when there was preoperatively central or proximal mixed thrombosis.
Statistics analysis
Statistical analysis was performed using SPSS Version 19.0 (SPSS Inc., Chicago, Illinois, USA). The incidence was reported as a percentage. An independent sample t-test and the χ 2 test were used in the statistical analysis. If the p of a factor was <0.05 in the univariate analysis, the variable was selected for the multivariate analysis. A multivariate analysis was used to detect the risk or protective factors. The difference was statistically significant (p < 0.05).
Results
Patient characteristics
A total of 228 patients with femoral neck fractures who were admitted to our hospital were included. The patients’ mean (SD) age was 71.3 (13.5) years. One hundred fifty patients (66%) were female, and 78 (34%) were male. Open reduction and internal fixations (ORIFs) were performed in 48 (21%) patients, hemiarthroplasty was performed in 152 (67%) patients, and total hip replacement (THR) was performed in 28 (12%) patients. The average days of preoperative screening DVT was 3.6 days postfracture. Of all the patients, only six patients had placement of an IVC filter before operation, and the IVC filters were removed after operation. No fatal bleeding events or pulmonary embolism was found in this study. No death was recorded.
Incidence of DVT on preoperative ultrasonography
Seventy-three patients (32%) had thrombosis and 155 (68%) had no thrombosis (Table 1). Of the cases, 66 (29%) were peripheral DVT, 1 (0.4%) was central DVT, and 6 (2.6%) were mixed DVT. Peripheral DVTs occurred in 63 (90%) of all patients with DVTs. Symptomatic DVTs occurred in 7 (9.6%) patients.
Patient characteristics according to preoperative ultrasound.

BMI: body mass index; ASA: American Society of Anesthesiologists; CRP: C-reactive protein.
The incidence of preoperative DVT on the uninjured side was 14%, accounting for 45% of all preoperative DVT cases. Of the patients, 15 (20%) had uninjured lower extremity DVT and 18 (25%) had DVT in the both lower extremities. There were three (4.1%) central DVTs on the uninjured side. Forty (55%) patients had a single DVT in the injured lower extremity.
Univariate analysis of preoperative DVT
No statistical differences were observed in the unilateral or bilateral limb, medical morbidity (excluding diabetes and coronary heart disease), body mass index (BMI), American Society of Anesthesiologists (ASA) classification, D-dimer level at admission and before operation, and C-reactive protein (CRP) level at admission between the two groups (Table 1). However, the thrombosis group had a higher proportion of females (p = 0.02), were older (p = 0.01), and had a longer interval between injury onset and surgery (p = 0.04).
Multivariate analysis of preoperative DVT
A multivariate analysis was used to detect the risk factors by entering age, sex, diabetes, coronary heart disease, and number of days between fracture and operation. The results showed that diabetes (odds ratio (OR), 2.72; 95% confidence interval (CI), 1.23–6.01; p = 0.01) was an independent risk factor of preoperative DVT (Table 2).
Multivariate analysis of preoperative and postoperative DVT.
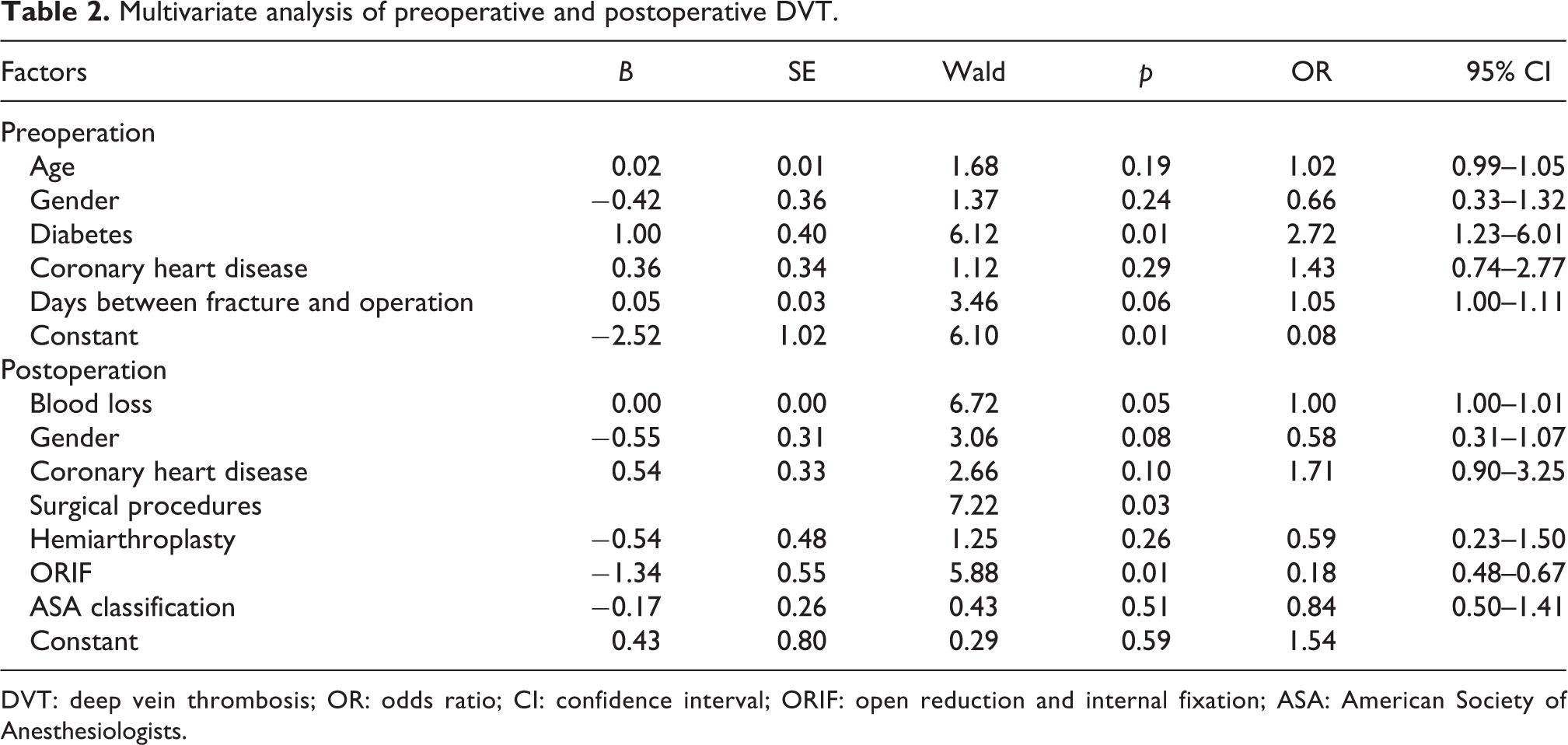
DVT: deep vein thrombosis; OR: odds ratio; CI: confidence interval; ORIF: open reduction and internal fixation; ASA: American Society of Anesthesiologists.
Incidence of DVT on postoperative ultrasonography
After operation, 128 (56%) patients developed a thrombosis and 100 (44%) did not. Of the cases, 107 (47%) were peripheral DVT, 1 (0.4%) was central DVT, and 20 (8.8%) were mixed DVT. Peripheral DVT was 107 (84%) of all DVT cases (Table 3). Symptomatic DVT was found in 31 (24%) patients of all DVT cases.
Patient characteristics according to postoperative ultrasound.

BMI: body mass index; ASA: American Society of Anesthesiologists; ORIF: open reduction and internal fixation; THR: total hip replacement; CRP: C-reactive protein.
The incidence of postoperative DVT on the uninjured side was 24%, accounting for 43% of all postoperative DVT cases. Of the 128 patients, 13 (10%) had uninjured lower extremity DVT and 42 (33%) had a DVT in both lower extremities. There were one (0.7%) central DVT on the uninjured side. Seventy-three (57%) patients had a single DVT in the injured lower extremity.
Univariate analysis of postoperative DVT
No statistically significant differences in age, unilateral or bilateral limbs, fracture type, medical morbidity (excluding coronary heart disease), BMI, length of hospital stay, interval (days) between fracture onset and hospitalization, interval (days) between fracture onset and hospitalization, operation duration, transfusion, liquid transfusion, drainage, D-dimer level at admission and before operation, and CRP level at admission and at postoperative day 5 were found between the two groups. However, the thrombosis group had more female patients (p = 0.01) than the non-thrombosis group. In addition, coronary heart disease (p = 0.03), ASA classification (p = 0.02), surgical procedures (p < 0.01), and blood loss (p = 0.00) were significantly associated contributing factors to postoperative thrombosis. Among the serum markers, the D-dimer levels on postoperative days 1 and 5 were higher in the thrombosis group (Table 3).
Multivariate analysis of postoperative DVT
The multivariate analysis results showed that blood loss (OR, 1.00; 95% CI, 1.00–1.01; p = 0.05) was an independent risk factor of postoperative DVT, and ORIF surgical procedure (OR, 0.18; 95% CI, 0.48–0.67; p = 0.01) was an independent protective factor of postoperative DVT, as compared with hemiarthroplasty and THR (Table 2).
Dynamic changes of DVT before and after operation
The dynamic preoperative and postoperative changes of DVT are shown in Figure 1. Of the 228 patients, 144 (63%) showed no changes in hospitalization duration. New DVT arose in 64 (28%) of the patients after operation, and peripheral DVT constituted 56 (88%) of all new DVT cases. Of the DVT cases, nine (3.9%) disappeared after operation (Figure 1).
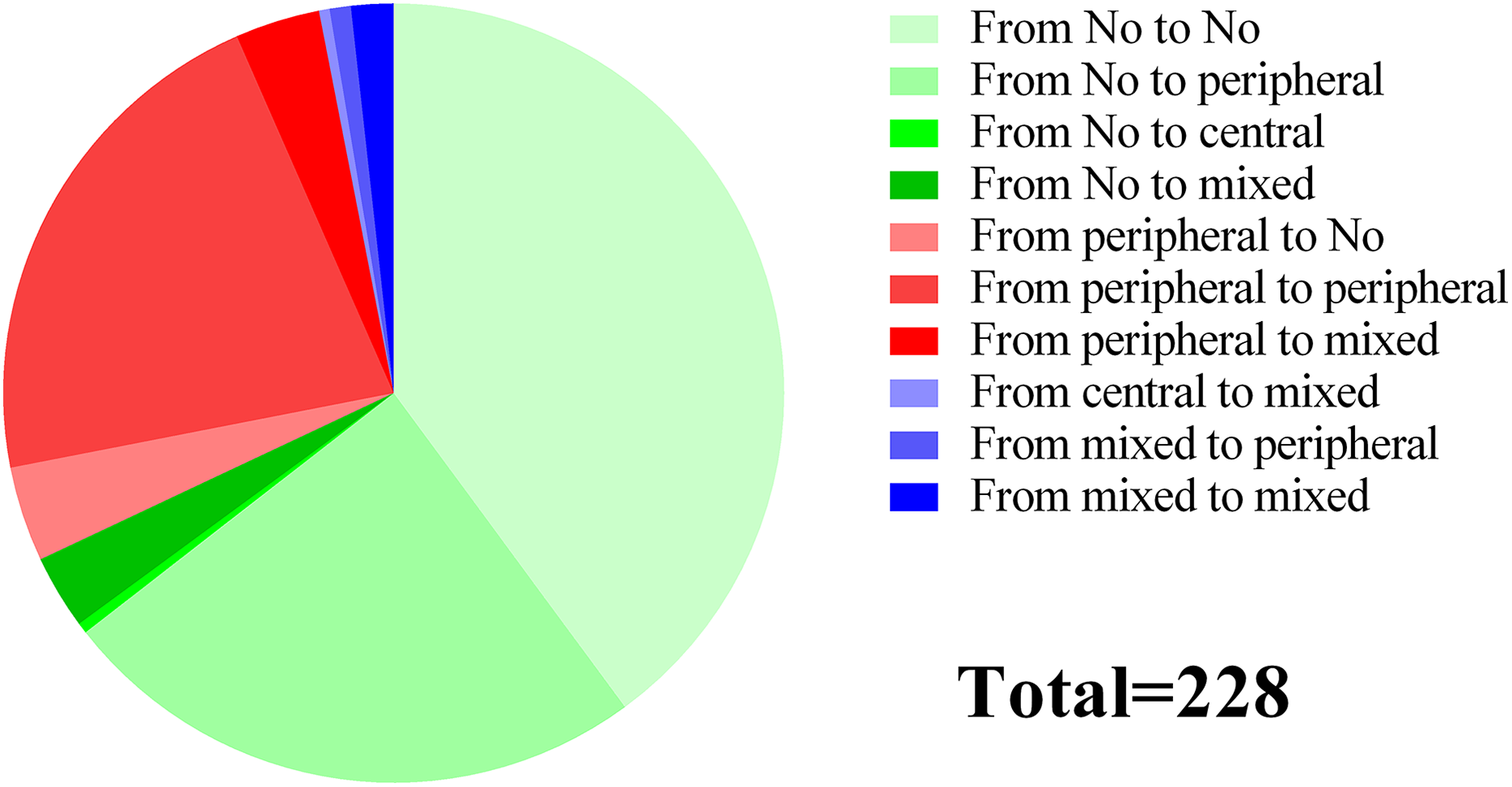
Dynamic changes of DVT before and after operation. DVT: deep vein thrombosis.
Discussion
This retrospective study has the following findings: (a) the incidence of preoperative and postoperative DVT was 32% and 56%, respectively; (b) the incidence of preoperative DVT on the uninjured side was 14%, accounting for 45% of all preoperative DVT cases; the incidence of postoperative DVT on the uninjured side was 24%, accounting for 43% of all postoperative DVT cases; (c) diabetes was the independent risk factor of preoperative DVT; (d) blood loss was an independent risk factor, and ORIF surgical procedures were an independent protective factor of postoperative DVT; (e) peripheral DVT constituted 90% and 84% of all preoperative and postoperative DVT cases, respectively; and (f) the changes of DVT obviously increased from before to after operation. Little is known regarding DVT before fracture onset in the general population. We assumed that DVT develops after injury, not before a fall or fracture. Kniffin et al. reported that the annual incidence rate of DVT per 10,000 persons was 18 at age 65–69 years, and this rate increased steadily to 31 by age 85–89 years. 16 The incidence rates were low. Thus, most of the DVT cases in our study were not preceded by injury.
In this study, ultrasonography was used to diagnose DVT. We chose ultrasonography based on its high accuracy and widespread acceptance. Ultrasonography is a simple, robust and noninvasive diagnostic tool and serves as a first choice in the diagnostic workup of DVT in lower extremities. Although the sensitivity and specificity of venography and magnetic resonance imaging are within the range of ultrasonography, they may serve as an alternative or complementary imaging tool to ultrasonography. 17 In addition, when there was no DVT under ultrasonography, the thromboelastography could be tested to assess the DVT risk.
Many factors contribute to the development of thrombosis after trauma. 18,19 In this study, we found that diabetes was an independent risk factor of preoperative DVT in patients with femoral neck fracture. The result is similar to those of the studies from Yang et al. 20 and Su et al., 21 and diabetes increases the risk of DVT and pulmonary embolism. 22 The possible pathophysiological mechanisms included increased platelet and procoagulant protein activities together with the compromised function of the fibrinolytic system in diabetes with enhanced thrombotic milieu. 23
In the multivariate analysis, blood loss and surgical treatment method were independent risk or protective factors of postoperative DVT. Riha et al. also reported that blood loss was an independent factor that promotes postoperative hypercoagulability states. 24 In additional, Selby et al. and Meissner et al. proved that the hypercoagulability state persists for a long time after fractures. 25,26 Thus, blood loss is a contributing factor to postoperative DVT. Blood loss in the thrombosis group (276 ± 152 mL) was greater than that in the non-thrombosis group (218 ± 100 mL). We also observed that the surgical treatment method influenced the formation of DVT. The patients who underwent an internal fixation had a lower incidence of DVT than those who underwent hemiarthroplasty or THR. The reasons should be as follows: First, most of the patients who underwent internal fixation were younger, 15,27 with mean ages of 55 ± 14, 68 ± 6, and 77 ± 9 years in the ORIF, THR, and hemiarthroplasty group, respectively, and had a relatively low incidence of thrombosis. Second, the injury was relatively mild in the ORIF group, and the patients who underwent an ORIF had less pain and were more active than those who underwent hemiarthroplasty or THR. Third, the mean blood loss was lower in the ORIF group (215 ± 190 mL) than in the THR (329 ± 108 mL) and hemiarthroplasty groups (247 ± 111 mL), so the hypercoagulability state may be milder with ORIF than with the latter two treatment methods.
In the subgroup analysis, the DVT cases were classified into central, peripheral, and mixed groups. Owing to the small number of patients with only central DVT, we compared the postoperative results between the peripheral and mixed groups. The results showed that the D-dimer level on postoperative day 1 was higher in the mixed group than in the peripheral group (15 ± 11 vs. 9 ± 8 mg/L, p = 0.02).
In femoral neck fractures, the incidence of DVT was reported to be up to 19.5%. 7 In our study, the incidence was higher than in other studies. The reasons include the following aspects. As we described in the introduction section, previous studies focused on symptomatic DVT and some studies ignored DVT in uninjured extremities. First, in this study, preoperative and postoperative symptomatic DVT accounted for only 9.6% and 24% of all DVT cases, respectively. Second, after removing the data on DVT on the uninjured side only, the incidence rate of DVT decreased to 25% preoperatively and 50% postoperatively. The preoperative and postoperative incidence rates of DVT on the uninjured side were 14% and 24%, respectively. Thus, owing to the high incidence of asymptomatic DVT involving the uninjured limb, we recommend routine DVT ultrasonography screening.
Even though the study has included the large cohort of patients, analyzed preoperative and postoperative DVT respectively, there were some limitations should be clarified. At first, the design was retrospective study, which was introduced confounding factors easily. Secondly, the mean interval between fracture onset and operation was 6 ± 5 days in all the patients. The more delayed, the more thrombosis. The reason of the delayed treatment was mainly transportation from other hospitals to our trauma center and the poor comorbidity of elderly patients, which needs more time for preoperative preparation. In fact, one of the few things that saves lives in the elderly population is the early surgery. Therefore, fast track pathway should be considered for elderly population.
Conclusions
In conclusion, the incidence rates of preoperative and postoperative DVT in the patients with femoral neck fracture were high, and orthopedists should pay more attention to DVT as a complication.
Footnotes
Acknowledgements
We thank all our colleagues in the Department of Orthopedic Trauma, Honghui Hospital, Xi’an Jiaotong University.
Author contributions
ZBF, ZY, and ZK helped in conceptualization. FC, WPF, XX, SK, YK, and KC performed data curation. ZBF and FYH were in charge of formal analysis. FYH and LP discussed the roles, writing, and original drafting.
Availability of data and materials
The survey was conducted by Xi’an Honghui Hospital. According to relevant regulations, the data could not be shared.
Ethics approval and consent to participate
The study was approved by the ethics review board of Xi’an JiaoTong University (no. 2014026).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the financial support for the research, authorship, and/or publication of this article: This study was supported by the Social Development Foundation of Shaanxi Province (grant number 2017ZDXM-SF-009).