
Abstract
Traumatic hip dislocation usually occurs in young patients, with the increasing number of high-energy injuries, and 62–93% of reported adult traumatic hip dislocations were caused by high-speed motor vehicle crashes. However, ipsilateral femoral neck fractures and intertrochanteric fractures with posterior dislocation of the hip are extremely rare, and this injury poses a challenge to orthopaedic surgeons. Here, we report two cases of simultaneous ipsilateral femoral neck fracture, intertrochanteric fracture and posterior dislocation of the hip joint in young patients who were treated with proximal femoral locking compression plate (PFLCP). The long-term follow-up (one patient was followed up for 3 years and the other for 7 years) showed that these patients had excellent functional outcomes with near-normal ranges of hip movement. The authors believe that using smaller plates with the lateral PFLCP is an acceptable method to treat this injury in young patients.
Introduction
Traumatic hip dislocation usually occurs in young patients who are at risk of sustaining high-energy injuries. High-speed motor vehicle accidents account for between 62% and 93% of adult traumatic hip dislocations. 1 However, ipsilateral femoral neck fractures and intertrochanteric fractures with posterior dislocation of the hip are extremely rare, and this injury poses a challenge to orthopaedic surgeons. 2 –4 Only two cases have been previously reported in the literature. 5,6
In this article, we report two cases of simultaneous ipsilateral femoral neck fracture, intertrochanteric fracture and posterior dislocation of the hip joint in young patients. We discuss the mechanism of injury and how to obtain an accurate diagnosis in the emergency department. Such injuries are challenging for medical professionals who must decide the internal fixation that will be used for surgery. Based on our clinical experience, we treated the two cases with proximal femoral locking compression plate (PFLCP), and the long-term follow-up results showed that these patients had excellent functional outcomes with near-normal ranges of hip movement.
Case description
Case 1
A 38-year-old unconscious woman was admitted to our emergency department with hypotension (78/65) after a high-speed train crash in July 2011. The radiographs and full-body computed tomography (CT) scan showed hydropneumothorax, rib fracture, acetabular fracture, sacral fracture, femoral neck fractures, intertrochanteric fractures, and dislocation of the hip (Figure 1). Her broken leg was immediately placed in traction to prevent further displacement of the fracture and damage to the blood supply of the femoral head. Preoperative traction failed to restore dislocation and the position of femoral head remained unchanged. After 2 weeks, the general condition of the patient had become stable, and we decided to operate through a posterolateral approach in a lateral position. Since she was 38 years old, the femoral neck fractures and intertrochanteric fractures were fixed by PFLCP and multiple cancellous screws. The cerclage wire was used to reduce the femoral shaft. The type of acetabular fracture was avulsion fracture of posterior acetabular wall with nonoperative management.

(a) Plain preoperative radiograph and (b) three-dimensional reconstructed CT image. CT: computed tomography.
Our patient did not complain of pain in her leg and her hip joint function after surgery was satisfactory. However, 1 year later, the patient experienced slight hip pain, and the radiograph revealed osteonecrosis of the femoral head (ONFH) with a loosening of the Kirschner wire (Figure 2(c)). The loose Kirschner wire was immediately removed, after which our patient felt better. Three years after operation, radiographs showed that the ONFH was aggravated, and the femoral head had collapsed (Figure 2(d)). We advised the patient to remove the internal fixation to prevent further damage to the acetabulum; however, she refused citing good function and negligible pain. At a follow-up visit 7 years after the thigh problem, the patient complained of irregular dull hip pain with a Harris Hip Score of 92, but she refused to accept an X-ray examination.
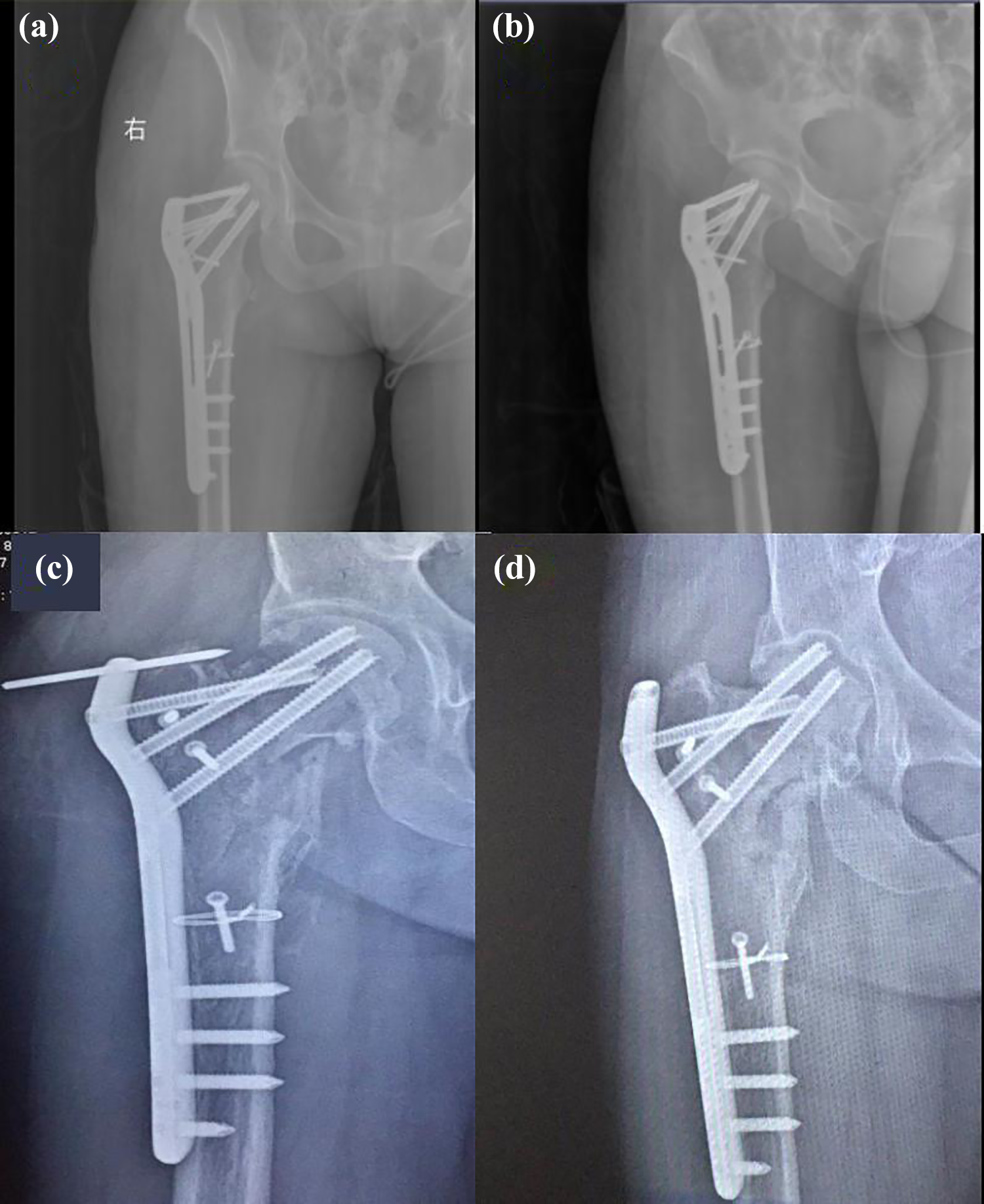
(a) Postoperative anteroposterior and (b) oblique radiographs. (c) One year postoperative radiograph showing ONFH with the loosening of the Kirschner wire. (d) The radiograph 3 years after the surgery showing that the osteonecrosis of femoral head was aggravated and that the femoral head appeared to have collapsed. ONFH: osteonecrosis of the femoral head.
Case 2
A 29-year-old man was admitted to our hospital with a deformity and swelling in the right hip after a traffic accident. On physical examination, the patient’s right leg was shorter than the left one. The X-ray and CT scan revealed ipsilateral femoral neck fractures and intertrochanteric fractures with posterior dislocation of the hip (Figure 3(a) and (b)). No other injuries were found.

(a) Plain preoperative radiograph, (b) axial image CT scan, (c) 1 year postoperative anteroposterior radiograph, and (d) 3 years postoperative anteroposterior radiograph. CT: computed tomography.
We failed to reset the dislocation of hip joint by closed reduction. Traction was not used before operation, and surgery was performed 3 days after the trauma (the patient was injured on weekend, but our hospital only allowed our treatment group to operate on Tuesday). The treatment included reduction of the dislocation of the hip and an open reduction and plate fixation of the femur neck and intertrochanteric fracture through a posterolateral approach in a lateral position. The intertrochanteric fracture was fixed with two smaller plates, and the femur neck was treated with PFLCP. During his 3-year follow-up period, the patient never had any complaints about joint pain and had a good function of hip joint with a Harris Hip Score of 96, and there was no evidence of femoral head necrosis (Figure 3(c) and (d)).
Discussion
Simultaneous ipsilateral femoral neck fractures and intertrochanteric fractures are uncommon injuries, while injuries with a concomitant dislocation of the hip are rarer. Here, we have shown the good clinical efficacy of PFLCP in this type of fracture and dislocation. Only two cases have been previously reported in the literature. Both cases were fixed with dynamic hip screws (DHS), 5,6 and they were young patients. We believe that after the hip has been dislocated, a violent rotation may lead to additional fractures in young patients.
It is difficult to diagnose this fracture with radiographs, but three-dimensional reconstructed CT scans can be used to obtain an accurate diagnosis in the emergency department. Both femoral neck fractures and dislocation of the hip may result in avascular necrosis of the femoral heads. 1,7 It is a well-known fact that the reduction of the dislocation should be performed as soon as possible to minimize the risk of osteonecrosis. 1 However, these fractures and dislocation are usually caused by high-energy injures, when patients’ health situations are too unstable to operate. The optimal timing and processing method for each operation must be planned in relation to the patient’s physiological status and other injuries.
Due to the high risk of nonunion (9.3%) and avascular necrosis (14.3%) for isolated femoral neck fractures, 7 aged patients should have a lower threshold for primary arthroplasty, while the younger patients need to be treated by open reduction and internal fixation to achieve anatomic reduction. We would expect our patients’ complex hip disolcations would have a greater risk of nonunion and avascular necrosis. Avascaular necrosis occurred in one of our two patients. Compared with case 2, case 1 had a longer dislocation time of the hip joint which may have impeded vascular flow to the femoral head. Furthermore, the fracture pattern was more comminuted and was fixed without using additional plates for the smaller fragments.
An open approach can promote the decompression of the intracapsular hematoma, which may prevent adequate blood flow to the femoral head and increase the risk for avascular necrosis. 8 Both patients were fixed through a posterolateral approach in a lateral position. Compared with anterior surgical approach, the posterolateral approach poses a relatively higher risk for ONFH due to disruption of the femoral heads blood supply. Knowledge of the vascular danger zones could help us to protect the remaining blood supply of femoral head during surgery.
DHS allows for the controlled dynamic sliding of the femoral head component along the construct. Since three part fractures are unstable, compression may facilitate the shortening of the ipsilateral femur neck or fracture displacement. The two cases using DHS used derotational screws to give necessary additional rotational control. 5,6 PFLCP is a stronger construct for stabilizing a vertical shear femoral neck fracture. 9 In addition, it is not necessary to keep it in close contact with the bone surface, and it can be bent to match the femoral shape, which can protect the blood supply of periosteum.
There are no classifications of such fractures and dislocation. With the increasing number of high-energy injuries, this injury should be included in the existing classification system for hip fractures and dislocations. We suggested to add this injury to the Thompson and Epstein type. The authors believe that each patient must be considered separately to determine the selection of the internal fixation.
Conclusion
Combined ipsilateral femoral neck and intertrochanteric fractures with hip dislocation are extremely rare hip injuries. In our experience, it is hard to reset the dislocation of hip joint by closed reduction. The authors believe that using smaller plates with the lateral PFLCP is an acceptable method for treating this injury in young patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
All information was obtained with the patient’s consent.