
Abstract
Introduction:
The effect of leg dominance on anterior cruciate ligament (ACL) injuries has been studied with some studies noting a propensity for injuries in the non-dominant leg. Its effect on post-ACL reconstruction recovery, however, is not well known. The authors hypothesize that dominant limb injuries undergo rehabilitation faster and positively affect early functional outcome scores and return to sports and set about studying these effects.
Methods:
This is a retrospective study of 254 patients from a single institution who underwent ACL reconstruction for acute ACL ruptures and the results were compared between patients with dominant and non-dominant limb injuries. Objective measurements including the KT-1000, single-leg hop distance and Biodex knee extension peak torque were used to evaluate recovery. Pre- and post-operative functional outcome scores such as the International Knee Documentation Committee (IKDC), Tegner activity score and Lysholm knee scale were documented.
Results:
Early functional outcomes were similar. Minimal clinically important difference (MCID) improvement in IKDC scores was achieved in 69.7% of the dominant versus 66.0% of the non-dominant injury group (p = 0.99), 75.2% versus 79.6% (p = 0.45) for the Lysholm knee scale, and 81.6% versus 84.9% (p = 0.50) for the Tegner activity score. The majority of patients in both subgroups had a return of at least 80% of peak knee flexion and extension peak torque at 5.4 months post-operatively; 92.9% of subjects with a non-dominant leg injury and 87.2% with a dominant leg injury had returned to their pre-injury sports 1 year from surgery.
Conclusions:
Results from this study suggest that despite theoretical differences, leg dominance does not have a significant impact on short-term functional outcomes and return to sports. Objective measurements suggest that limb strength recovers at a comparable rate. Injuries to either leg demonstrate equally positive improvement post-ACL reconstruction given the same post-operative rehabilitation.
Level of Evidence:
III, retrospective comparative study.
Level of Evidence:
III, retrospective cohort study.
Background
Anterior cruciate ligament (ACL) injury is a common orthopaedic sports injury that occurs in the younger population who actively participate in sporting activities. Estimates put the frequency of tears at 1–10 in 1000 people every year. 1 A significant proportion of patients with such injuries experience loss of ability to participate in sporting activities and require ligament reconstruction for return to sports. Many factors have been purported to contribute to injuries and affect outcomes of surgical ACL reconstruction. Studies looking at the return to sports post-ACL reconstruction conclude that the time required to return to pre-injury sports may take more than a year. 2,3 The factors affecting return to sports have not been clearly identified, with psychosocial factors being postulated of importance. 4,5
Physical factors such as the effect of leg dominance on knee joint kinematics pre- and post-operatively for ACL have been studied for individual sports. 6 Studies have demonstrated higher resting electromyography (EMG) 7 as well as higher muscle output in the dominant legs of their subjects 8 – 10 with resultant kinematic differences. However, the effect of leg dominance on ACL injuries 11 –14 and biomechanics 15 is controversial. There is a debate on the impact of leg dominance on ACL injuries and limited literature on the effect of leg dominance on ACL reconstruction functional outcomes. In this study, we look at the effect of leg dominance on post-ACL reconstruction functional outcome scores and return to sports.
Questions/purposes
Time to return to sports varies greatly among patients’ post-ACL reconstruction and its factors are still poorly understood. The authors hypothesize that dominant limb injuries undergo post-operative physiotherapy and rehabilitation more effectively and lead to better functional outcomes and return to sports in the short term.
Patients and methods
This is a retrospective study involving patients who underwent primary ACL reconstruction for ACL ruptures between 2013 and 2014 in the Singapore General Hospital, Department of Orthopaedic Surgery. Institutional review board approval (ref. no. 2016/2544) was obtained for the completion of this retrospective cohort study. A total of 254 patients who had ACL rupture and failed conservative management underwent arthroscopic ACL reconstruction using ipsilateral hamstring autografts. Of the 254 patients, 78 patients had concomitant meniscal injuries who underwent partial meniscectomy, 31 underwent double-bundle ACL reconstruction, whereas 8 underwent bone–patella tendon–bone ACL reconstruction. Patients with revision ACL reconstruction, multi-ligamentous injuries or associated meniscal injuries requiring meniscal repair were excluded from the study as these factors would affect the immediate post-operative physiotherapy management due to prolonged weight-bearing and range of motion (ROM) restrictions, which may affect the short-term functional outcomes. Prior to surgery, patients were commenced on physiotherapy for at least 6-week duration, with therapy goals of maintaining quadriceps strength and improving knee ROM.
Surgery was decided upon after discussion between the attending surgeon and patient, based on persistent patient-reported knee instability precluding attempts to return to previous sporting activities as well as clinical knee laxity with positive knee anterior drawer and Lachmann’s tests.
The patients were followed up for 1-year post-surgery. The patient group included patients who participated in both competitive and recreational sporting events, similar to the general population in our local clinic setting. The level of pre-operative sporting proficiency was assessed based on the patient’s pre-injury Tegner activity score.
Leg dominance was determined pre-operatively based on a questionnaire on the preferred limb to execute an action 6,16 –18 (e.g. leg used to kick a ball and front leg used in lunging for retrieval in racquet sports). Most patients were uncomfortable with further objective tests that were not perceived to directly impact their recovery. Pre-operative Tegner activity scores, International Knee Documentation Committee (IKDC) and Lysholm knee scales were obtained by the Orthopaedic Diagnostic Centre (ODC), Department of Orthopaedic Surgery in our institution.
All patients underwent arthroscopic ACL reconstruction in our institution between 2013 and 2014 by consultant orthopaedic surgeons in our institution. Patients were discharged on post-operative day 1 once pain control was adequate and were commenced on a standardized hospital physiotherapy rehabilitative protocol with restricted ROM in the first 2 weeks with the use of a hinged knee brace, followed by progressive ROM increase. Full ROM was allowed at 6 weeks post-operatively and patients were started on muscle conditioning via closed-chain exercises. Patients were allowed to resume recreational sporting activities from 6 months post-operatively 6,19 upon achieving comparable hop tests (85%) and Biodex scores (80%) as the uninjured limb. 20 The intensity of the sporting activities was to be increased progressively. Follow-up clinic reviews were scheduled at 2 weeks, 6 weeks, 3 months, 6 months and 1 year post-operatively. Patient functional outcomes scores were captured at specific time points on their follow-up visits, up to 1-year post-surgery. The Tegner activity scale and Lysholm knee scales as well as the IKDC knee 21 and KT-1000 22 values were obtained at the 1-year follow-up visit. These scores were compared to the scores obtained pre-operatively and interpreted in conjunction with the minimal clinically important difference (MCID) of Lysholm knee scale at 10.1 and Tegner activity scale at 1. 23,24 The 1993 IKDC knee form is utilized in our institution. Functional knee scores for the 1993 IKDC knee forms were scored and given an alphabetical grade. The worst grade achieved in any of the subjective, symptom, ROM, ligament or functional score segments was taken as the overall IKDC grading for the patient. These grades were converted to numerical values for ease of statistical analysis (A = 1, B = 2, C = 3 and D = 4). The average IKDC grading pre-operatively as well as the proportion of patients who had a minimum one-grade improvement in overall IKDC grading was compared between the patient groups.
Objective measurements of outcome improvement were captured via the Biodex isokinetic dynamometer knee extension peak torques as well as KT-1000 scores and single-leg hop distances. The single-leg hop distance was used in conjunction with knee extension peak torque as a marker of limb strength and was measured at 1 year post-operatively. The differences in hop distance were compared between the two subgroups.
The outcome scores were extracted from standardized medical records from the hospital and the ODC for the purposes of this study.
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS v.20). Categorical data were analysed using χ 2 or Fisher’s exact tests, whilst other data were analysed using paired t-tests. A p value of <0.05 was interpreted as significant.
Results
We looked at 254 patients consisting of recreational sportsmen who underwent arthroscopic ACL reconstruction between 2013 and 2014. Of the 254 patients, 141 (55.5%) had injuries on the dominant leg, whereas 113 (44.5%) had injuries on the non-dominant leg; 75.2% sustained the injury during a non-contact event, whereas 24.8% sustained the injury after a direct contact with another player during sports. Contact injuries made up 34.4% of dominant leg injuries and 24.8% of non-dominant leg injuries (p = 0.203).
There were no reported ACL re-ruptures or infected ACL grafts requiring revision surgery in this group of patients at 1-year follow-up, and all patients had attempted to return to pre-injury sporting activities.
Patient demographics were similar between the two patient subgroups, with no significant difference in the age, sex ratio, BMI, ROM pre-operatively or time between injuries to date of operation between the two patient subgroups (Table 1). Patients were encouraged to participate in at least 6 weeks of standardized pre-operative knee rehabilitation protocol and surgery was only performed when acute swelling has subsided and ROM had been regained. The timing of surgery was decided after consult by both the patient and the surgeon.
Demographics.

ROM: range of motion; BMI: body mass index.
The mean pre-operative Tegner activity scale and Lysholm knee scale were 2.81 and 64.01, respectively, for the non-dominant leg injury subgroup, and 2.91 and 64.62, respectively, for the dominant leg injury subgroup. There were no significant differences in the pre-operative activity scores between the two subgroups (Table 2).
Pre- and post-operative subjective functional knee scores at 3 and 6 months and 1 year.

IKDC: International Knee Documentation Committee.
At 3 months post-operatively, Tegner and Lysholm scores were not significantly different between the two subgroups. At 3 months post-operatively, Tegner activity scale was at 2.87 for both subgroups, whereas the Lysholm knee scale was 76.9 and 78.2 (p = 0.57) for the non-dominant and dominant limb injury subgroup. At 6 months post-operatively, Tegner activity scale was 3.86 and 3.94 (p = 0.74) and Lysholm knee scale was 74.9 and 80.5 (p = 0.10) for the non-dominant and dominant injury subgroups respectively. At 1 year post-operatively, the post-operative Tegner activity scale was at 5.04 with a 2.21 improvement in the non-dominant leg injury subgroup and 5.30 (p = 0.24) with a 2.34 mean improvement (p = 0.85) in the dominant leg injury subgroup. The Lysholm knee scale in the non-dominant leg injury subgroup was 89.01 with a 24.62 mean improvement and 88.86 (p = 0.65) with a mean improvement of 24.53 (p = 0.97) in the dominant leg injury subgroup. There was no significant difference in the absolute scores as well as the mean improvement in scores between the two groups.
The proportion of patients in each subgroup who experienced clinically significant improvement (MCID) in the knee scales at 1-year time point was also similar. In patients with non-dominant leg injuries, 79.5% had clinically significant improvement in Lysholm knee scale and 84.6% had clinically significant improvement in Tegner activity scale. This was not statistically different from the subgroup of patients with dominant leg injuries, which saw clinically significant improvement in 75.2% (p = 0.46) in Lysholm knee scale and 81.6% (p = 0.62) improvement in Tegner activity scale.
There was no significant difference in the initial and 1-year IKDC overall grade between patients in the two subgroups. The initial IKDC overall grade was 3.90 for patients in the non-dominant leg injury subgroup and 3.85 (p = 0.40) for the dominant leg injury subgroup. One-year IDKC overall grade was 2.89 and 2.79 (p = 0.99) for the non-dominant and dominant subgroups, respectively. The proportion of patients who achieved at least one-grade improvement in the overall IKDC score was 69.7% and 66.0% (p = 0.95) for the dominant and non-dominant injury subgroups.
Pre-operative and 1-year post-operative KT-1000 scores were captured as objective measurements of outcome improvement (Table 4); 231 (90.9%) patients had consented to this measurement modality. Pre-operative KT-1000 scores were 4.10 for the non-dominant injury subgroup and 4.17 (p = 0.86) for the dominant injury subgroup and 2.00 and 2.17 (p = 0.65) 1 year post-operatively. The improvement in KT-1000 scores of 2.24 and 2.18 (p = 0.89) for the non-dominant and dominant injury subgroups were not statistically significant.
Proportion of injuries achieving significant clinical improvement of Tegner and Lysholm knee scales and proportion return to sports at 1 year.
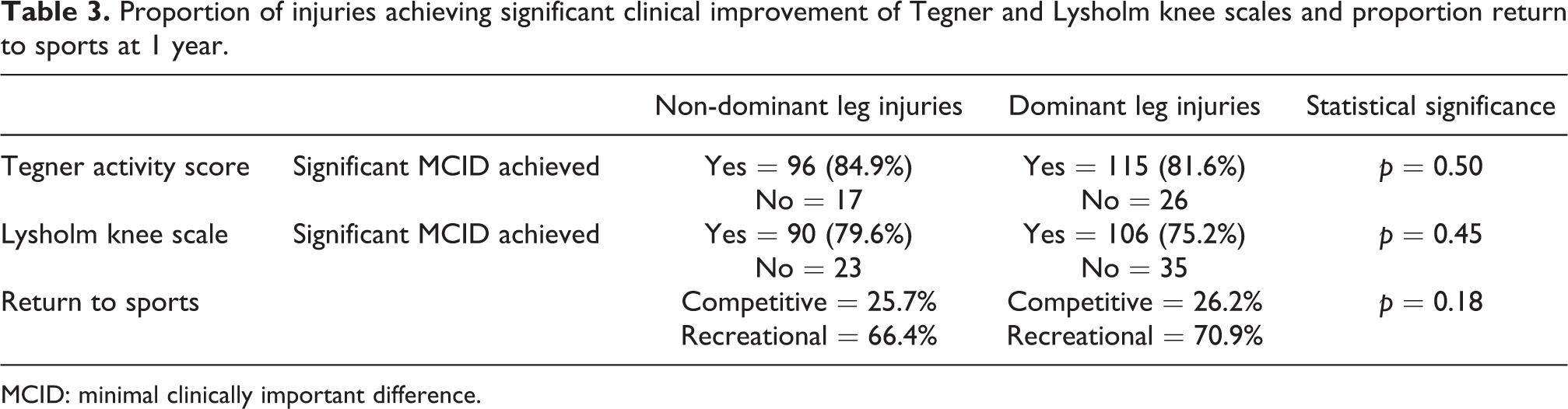
MCID: minimal clinically important difference.
Pre- and post-operative KT-1000 scores, post-operative hop distance at 1 year.
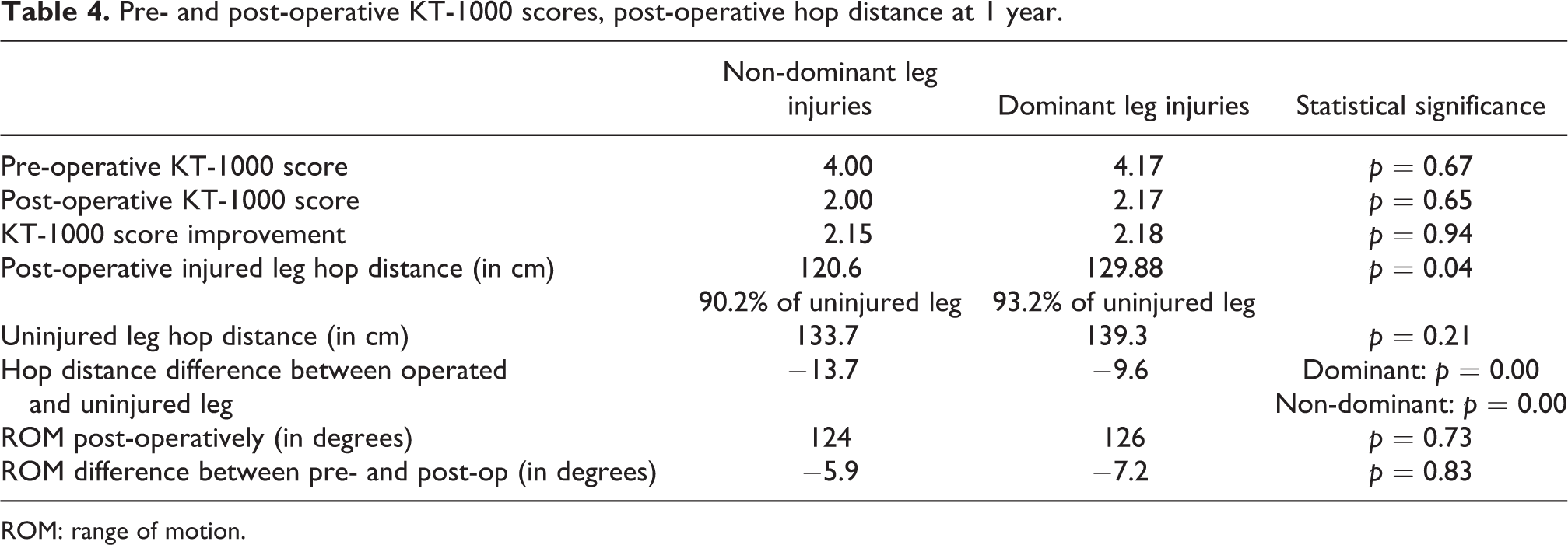
ROM: range of motion.
Post-operative hop distance in the operated knee was higher in the dominant leg injury subgroup. The hop distance between the injured and uninjured legs within each subject remained significantly different at 1 year post-operatively in both patient subgroups. Biodex knee flexion and extension peak torque scores were captured at an average of 5.4 months post-operatively, with no significant difference between the subgroups. Dominant limb injuries achieved 162 and 95.8 Nm knee extension and flexion peak torque, similar to that of 158 and 99.7 Nm in the non-dominant limb injury subgroup (Table 5).
Biodex knee extension peak torque scores.

At 1-year post-surgery, 25.7% and 26.5% of the patients in the two subgroups have returned to competitive sports, with 67.2% and 71.0% in the respective groups having returned to recreational sports (Table 3). This represents a return to sports in 92.9% of patients in the non-dominant subgroup and 97.2% in the dominant subgroup (p = 0.28).
Discussion
ACL injuries are common sports injuries. The risk factors for ACL injuries have been studied extensively, but there is limited literature on the effect of leg dominance on ACL injuries, 25,26 although its impact on ACL injuries in specific sports has been significant. 6,27 Chomiak et al. 28 reported no effect of limb dominance on severe ankle and non-contact knee injuries in male soccer players; however, the dominant leg incurred significantly more contact knee injuries. Orchard 29 reported that quadriceps strains were more commonly sustained by the dominant leg than the non-dominant side in female netball players.
There is, however, limited literature looking at the effect of leg dominance in post-operative ACL reconstruction recovery and functional outcome scores and return to sports. There have been studies demonstrating no difference in unilateral postural stability between dominant and non-dominant lower limbs in an uninjured study group, 30 but these studies had small sample sizes. Based on the available literature, the authors were interested in finding out the effect of leg dominance on short-term ACL recovery and functional outcomes, and if injuries in the non-dominant leg, translated to poorer recovery.
The patients were selected from our local institution. Cases with confounding factors such as associated meniscal injuries requiring repair or multi-ligamentous injuries requiring reconstruction and individualized rehabilitative protocols were excluded. The two patient subgroups had similar demographics (age and sex distribution) as well as pre-operative ROM and duration from injury to surgery. The proportion of patients who participated in competitive level sports was similar in both subgroups, while the Tegner and Lysholm knee scales pre-operatively were similar. The reported demographic factors and patient-reported activity levels do not seem to have a significant impact on the limb that the patient is likely to injure.
The patients were put through a similar physiotherapy programme by our physiotherapy department post-operatively. The mean Tegner and Lysholm knee scores were similar at 6 months post-operatively, and the absolute improvement in these scores was similar in both subgroups at both the 6 months and 1 year post-operatively time points. Patients continued to improve from 6 months to 12 months post-operatively. The proportion of patients who had improvement beyond the MCID 23,24 in each of the scales in both patient subgroups was also not significantly different. The results demonstrate that leg dominance does not significantly affect the improvement in knee objective and functional outcome scores post-operatively for ACL reconstruction in the short- to mid-term, with both groups doing equally well. Patients should be informed that they will continue to improve up to at least 1 year post-operatively, in line with expected ACL recovery timeframes.
The KT-1000 scores were derived by the subtraction of the anterior tibial motion relative to the femur of the injured knee as compared with the uninjured knee. Clinical trials have suggested that a score of >2 mm is highly suggestive of ACL injuries. 31 Pre-operatively, the scores of 4.10 and 4.17 in both patient subgroups are indicative of objective instability. These results were 2.00 and 2.17 in the non-dominant and dominant patient subgroups at the 1-year time point, evidence that objective stability has been improved. Although the post-operative KT-1000 results are not always below 2 mm for these patients, the ability for these patients to return to sports suggests that objective measurements should not be interpreted in isolation. The improvement of the KT-1000 scores at 1 year post-operatively was not significantly different between the two subgroups.
The hop distances were significantly higher post-operatively in the dominant leg injury subgroup, as is expected of a dominant leg. However, although the difference between the injured and uninjured legs was not statistically different between the two subgroups, the post-operative injured limb was still significantly weaker than the uninjured limb in both subgroups. Interpretation of these results is difficult as there is no baseline of the injured leg for comparison, but the authors note that the majority of subjects in both patient subgroups have been able to return to recreational sports at 1 year with significant improvement in functional knee outcome scores. Biodex knee flexion and extension peak torque score recovery were comparable between the two subgroups, with both subgroups achieving at least 80% strength compared to the uninjured limb approximately 5.4 months post-operatively. The results suggest that the recovery time for knee peak torque is not significantly different regardless of the leg injured.
As the dominant limb is expected to be equivalent to or superior to the non-dominant limb in subjective measurements such as the hop distance or Biodex scores, the results suggest that patients may not need to achieve return to baseline strength to be able to participate meaningfully in recreational sporting activities. Future work to evaluate the relationship between the return of limb strength in the injured limb and how this improvement towards baseline translates to further functional improvement is required. The presence of psychosocial factors 4,32 has also been postulated to play a part in determining the return to competitive sports.
The proportion of patients who had returned to competitive sporting activities at 1 year is generally similar between the two patient subgroups, consistent to that in the literature. 2,3,33 The authors do expect a lower rate of return to competitive sporting activities in the short term, as most of the study population are non-professional athletes with less necessity for early return to competitive sporting activities. However, the authors note that a significant proportion of our subjects in either subgroup were able to return to recreational sports at 1 year post-operatively. The results suggest that the majority of patients are able to commence recreational sports at 1 year post-operatively, although the return to competitive sports is at a lower rate. Our results suggest that leg dominance, despite its purported advantage of higher muscle output and improved knee kinematics, did not translate to the enhanced return of knee extension peak torque or return to sports in the short term. The authors agree that longer term follow-up studies are necessary to further evaluate the rate of return to competitive sporting events, although the effects of physical differences are unlikely to play a significant contributory effect in the long run.
The authors acknowledge some limitations in our study: Leg dominance was determined using a questionnaire and no subjective EMG was done. This was largely limited to patient preference not for further non-essential procedures prior to ACL reconstruction. Pre-operative objective measurements were not captured for the injured leg for analysis and comparison with post-operative outcomes. The study was targeted at evaluating limb dominance and its effect on ACL reconstruction and thus no further subgroup analysis on the specific techniques used by different surgeons as well as the duration between injury and surgery. The outcomes scores were not captured beyond 1 year post-operatively, as most patients have returned to an acceptable degree of participation in recreational sporting activities and were no longer keen for follow-up.
Conclusion
ACL injuries are common sports injuries that demonstrate good recovery post-ACL reconstruction. ACL injury recovery and return to sports have been well-studied, although the factors determining early return to sports have not been well established. Many factors have been attributed as contributing factors to ACL injuries, with leg dominance being one of them. There is limited literature on its contribution to post-ACL reconstruction outcomes and return to sports.
The results from this study suggest that leg dominance does not have a significant impact on the short-term functional outcomes and return to sports. Post-ACL reconstruction rehabilitative regimes can be similar regardless of limb dominance, with similarly good short-term outcomes in the non-dominant limb. Objective measurements suggest that limb strength recovers at a comparable rate regardless of limb dominance. The objective strength measurements and functional outcome improvement post-ACL reconstruction surgery at 1 year post-operatively are comparable, despite literature that suggests dominant legs having better muscle tone and power. Injuries to either leg demonstrate equally positive improvement post-ACL reconstruction given the same post-operative rehabilitation regime and have a similar return to sports.
Footnotes
Authors’ note
Institutional review board approval (ref. no. 2016-2544) was obtained for completion of this retrospective cohort study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.