
Abstract
Purpose:
(1) To compare postoperative range of motion (ROM), stability, and clinical outcomes between fixed-bearing posterior-stabilized (PS) and ultracongruent (UC). (2) The effect of postoperative stability on ROM and clinical outcomes was also evaluated in both designs.
Materials and methods:
Propensity score matching was conducted for age, gender, body mass index, preoperative ROM, Western Ontario and McMaster Universities Osteoarthritis (WOMAC) index, Knee Society (KS) scores, hip–knee–ankle (HKA) alignment, and follow-up period. Two hundred patients (100 PS and 100 UC) were enrolled. Preoperative and final follow-up outcomes including postoperative ROM, anteroposterior (AP) stability (good, fair, and poor), WOMAC index, and KS scores were compared. Then, postoperative outcomes compared between the PS and UC. We also analyzed if AP stability was associated with the postoperative outcomes in both implant designs.
Results:
In both groups, ROM and clinical outcomes of final follow-up showed improvement than preoperation. Statistical significance was not determined between the PS and UC groups in terms of postoperative ROM (PS vs. UC, 134.6° vs. 133.4°, p = 0.13), stability (good/fair/poor, 91/9/0 vs. 84/14/0, p = 0.376), WOMAC index, KS scores, and outliers of HKA alignment (15% vs. 10%, p = 0.393). “Fair” stability showed inferior KS scores but greater ROM than “good” stability in both designs.
Conclusion:
TKA with UC insert provided similar ROM, AP stability, and clinical outcomes when compared to PS insert. In both designs, greater postoperative ROM was found but inferior clinical outcomes were found when TKA resulted in fair stability instead of good stability.
Level of evidence III:
Retrospective comparative study.
Introduction
Posterior-stabilized (PS) total knee arthroplasty (TKA) was introduced as a technique due to multiple usefulness, such as severe malalignment or posterior cruciate ligament (PCL) insufficiency. 1,2 The PS design implant maintains a constant posterior femoral rollback during flexion, similar to the movement of the native knee, and showed favorable long-term outcomes. 3 But it has some disadvantages and complications—additional bone resection, post-produce fracture, and patellar clunk syndrome. 1,4,5 A highly conforming ultracongruent (UC) insert was introduced to overcome these complications. UC design has an increased anterior buildup and a more conforming articular surface to prevent anterior displacement during knee flexion and provides an easy option to substitute the PCL without additional bone resection. 6 Many studies have compared the results between UC and the other implant types—some studies compared mobile-bearing UC and PS design, 7,8 some other studies compared fixed-bearing UC implant and cruciate-retaining design, 9,10 and other previous studies compared between fixed-bearing UC and PS design in respect of intraoperative condition 11 –13 —the results have been controversial. Few studies compared between fixed-bearing UC and PS design in terms of range of motion (ROM), stability, and clinical outcomes; moreover, these studies are too short-term follow-up study or small volume study. 1,14
Previous studies suggested that some degree of knee instability (5–10 mm) in the anteroposterior (AP) direction gives satisfactory results including ROM in mid-flexion or 90° flexion; however, recent studies suggested that mid-flexion AP instability was related to poor outcome after TKA. 15 –22 These studies have conducted investigations of a CR or PS design; however, no study evaluated correlation between mid-flexion instability and postoperative outcomes in the UC-type insert.
Therefore, the purpose of this study was to compare postoperative ROM, mid-flexion stability, and clinical outcomes between fixed-bearing TKA with PS and UC insert. Then, we evaluated the influence of postoperative mid-flexion AP stability on ROM and clinical outcomes in each implant and in total cases. It was hypothesized that TKA with PS insert and UC insert would show similar postoperative results, and postoperative mid-flexion AP instability would be related to poor clinical outcomes with use of UC- and PS-type inserts.
Materials and methods
This was a retrospective comparative study with prospectively collected data and minimized the variability of the preoperative demographic, clinical scores, and preoperative hip–knee–ankle (HKA) alignment using propensity score matching. We reviewed the collected data of 1432 consecutive TKAs, conducted July 2010 to November 2014. Patients with a valgus deformity, history of revision surgery, a diagnosis other than osteoarthritis, a varus deformity of more than 20°, a body mass index (BMI) over 30 kg/m2, or a flexion contracture over 20° were excluded. In bilateral cases, 1 side (left or right) was selected by simple random sampling. We reviewed 331 patients—227 patients used the PS-type prosthesis (Scorpio NRG, Stryker, Allendale, New Jersay, USA; Figure 1(a)) and 104 patients used an UC-type prosthesis (Columbus, B. Braun, Aesculap, Tuttlingen, Germany; Figure 1(b)). In this study, propensity score matching was used for minimizing selection bias, and the matched variables were age at operation, gender, BMI, preoperative ROM, Western Ontario and McMaster Universities Osteoarthritis (WOMAC) index, Knee Society (KS) scores, HKA alignment, and follow-up period. 23,24 After matching, 100 patients used PS insert were matched with 100 patients used UC insert (Figure 2). All variables were successfully matched (Table 1). Mean follow-up period of PS group and UC group was 68.6 months and 68.5 months, respectively. This study was approved by our institution’s institutional review board (SMC 2015-05-060) and informed consent was obtained from all patients.
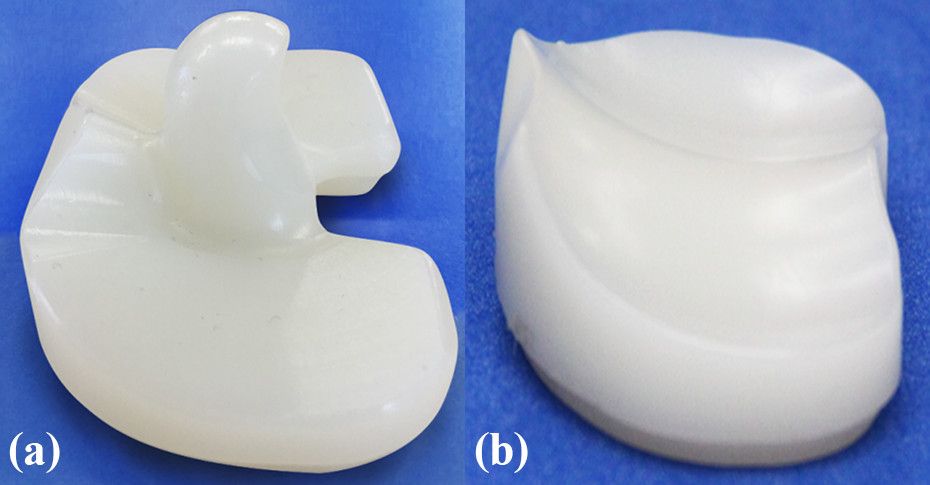
These photographs show two different fixed-bearing inserts. (a) NRG PS-bearing insert having a post and (b) Columbus UC prosthesis insert having an anterior buildup with a highly conforming deep dished geometry.

Flow chart describing the patients enrolled in this study.
Patient demographics after propensity score matching (mean ± standard deviation).

PS: posterior-stabilized; UC: ultracongruent; ROM: range of motion; WOMAC: Western Ontario and McMaster Universities Osteoarthritis; KS: Knee Society; HKA: hip–knee–ankle.
a Positive values indicate varus deformity.
All surgeries were conducted under pneumatic tourniquet inflation by the senior author. Both groups underwent TKAs with conducting a median skin incision, a standard medial parapatellar arthrotomy, and not doing patellar resurfacing. Surgery was conducted with gap-based femur cut technique—first, distal femur and proximal tibia cut were conducted perpendicular to the mechanical axis, then, femoral rotational alignment was determined by mediolateral flexion gap. A more detailed description of the surgical technique has been presented in our previous studies. 25,26 All patients started active and passive ROM exercises on the second postoperative day. Walking with a walker was also started on the second postoperative day.
Clinical assessments including ROM, WOMAC index, KS score, and AP stability were evaluated preoperatively and final follow-up. AP stability measurements were conducted via accurate physical examination and were checked by three different experienced orthopedic surgeons. The decision regarding the grade of stability was made by two or more surgeons in agreement. AP stability was measured in a 30° knee flexion state, and stability measurements were classified as good (0–5 mm), fair (5–10 mm), and poor (>10 mm) according to Lachman test grading system. 27 –29 All three times measurements were recorded in electronic medial recording system at every visit—87 patients of PS group and 91 patients of UC group showed unanimous agreement of stability. First, clinical assessments were compared between preoperation and final follow-up in each group. Then, clinical outcomes of final follow-up were compared between PS group and UC group. To analyze the influence of AP stability on postoperative results, ROM, WOMAC index, and KS scores were compared between good, fair, and poor stability in both implant groups, respectively.
HKA alignment was evaluated because poor postoperative coronal alignment is a potential bias of clinical outcomes. 30 Whole leg standing radiograph was evaluated before surgery and at final follow-up to measure HKA alignment. The HKA alignment was defined as the angle subtended by a line drawn from the center of the femoral head to the center of the knee and a line drawn from the center of the knee to the center of the talus. According to previous studies, outlier of postoperative HKA alignment was defined as over than varus 3° or valgus 3°. 30 Outlier number of postoperative HKA alignment was compared between PS group and UC group. Tourniquet time and amount of blood drainage were investigated and analyzed.
Statistical analysis
The Shapiro–Wilk test was used for checking the normality of distribution (Online Appendix 1). To compare variables between preoperation and final follow-up and between two different implant design groups, paired t-test, Student’s t-test, or Mann–Whitney test was used for continuous variables and a χ2 analysis was used for categorical variables. The influence of postoperative stability on postoperative ROM and clinical outcomes was evaluated using a Mann–Whitney test or a Student’s t-test. Analyzing the data and propensity score matching were conducted with Statistical Package for Social Science software version 21.0 (SPSS, Chicago, Illinois, USA) and SAS version 9.4 (SAS Institute, Cary, North Carolina, USA).
Results
In both groups, postoperation showed improvement when compared to the corresponding parameters preoperation in respect of ROM, WOMAC index, KS scores, and HKA alignment (Table 2). After TKA, statistical significance was not determined between the PS group and the UC group in terms of ROM, WOMAC index, KS knee score, KS functional score, tourniquet time, and amount blood drainage. There was no patient with poor stability. More AP instability was found in UC group but no statistical significance (good/fair/poor; PS—91/9/0, UC—86/14/0; p = 0.376). Outlier of HKA alignment also showed no statistical difference between two groups (PS vs. UC, 15% vs. 10%, p = 0.393; Table 3).
Clinical results of preoperation and final follow-up (mean ± standard deviation).

PS: posterior-stabilized; UC: ultracongruent; WOMAC: Western Ontario and McMaster Universities Osteoarthritis; KS: Knee Society; ROM: range of motion.
Postoperative results of PS and UC group (mean ± standard deviation).

PS: posterior-stabilized; UC: ultracongruent; ROM: range of motion; WOMAC: Western Ontario and McMaster Universities Osteoarthritis; KS: Knee Society; AP: anteroposterior; HKA: hip–knee–ankle.
In respect to the comparison between good and fair AP stability, patients with fair stability showed inferior KS score and functional score but better ROM than good stability in the PS and UC groups. WOMAC index was not shown significant difference (Table 4).
Influence of postoperative stability on postoperative results in both groups (mean ± standard deviation).

PS: posterior-stabilized; UC: ultracongruent; ROM: range of motion; WOMAC: Western Ontario and McMaster Universities Osteoarthritis; KS: Knee Society.
Discussion
The most important finding of this study was that the TKA with fixed-bearing UC insert provided similar postoperative results when compared to the fixed-bearing PS insert. In addition, mild mid-flexion instability decreased patients’ satisfactory but increased postoperative ROM.
Many studies have compared between TKAs with an UC insert and other design inserts. 9,11 –14,31,32 In terms of clinical outcomes, most of studies demonstrated similar results of UC design TKA with PS or CR, it is consistent with our study results. Multiple factors include geometry, implant size, type of insert, PCL integrity, and gap balancing are associated with AP instability in TKAs. Interest in TKA with UC insert is increasing, some studies underwent biomechanical study about UC design, demonstrated as inferior AP stability in 90° knee flexion state than PS design due to lack of post-cam mechanism. 11,14 Otherwise, one intraoperative study that compared AP stability between UC and PS in respect of 0°, 30°, 60°, and 90° flexion state demonstrated that UC showed greater AP translation in 60° and 90° but similar in 0° and 30°; this study suggested that implant design if UC or PS had minimal effect on mid-flexion instability. 12 This finding supports our study results that postoperative mid-flexion stability was similar between TKA with UC and PS insert. In terms of postoperative ROM, it is not clear if TKAs with UC insert provide similar ROM compared to CR or PS design. However, to the best of our knowledge, including our results, a favorable result of fixed-bearing UC was demonstrated when comparing with fixed-bearing PS. 1,14
It is controversial if there is correlation between AP stability and ROM, some previous studies have demonstrated that greater AP translation is correlated with better postoperative ROM in PS- and CR-type TKA, these studies suggested that additional flexion gap than extension gap occurred better flexion range. 15 –21 We think these previous results supported our results that patients with “fair” stability showed greater ROM than “good” stability regardless of insert design. Some previous studies reported AP translation of 5–10 mm was related to similar or better patients’ clinical outcomes. 15,33 However, in an outpatient clinic, some patients with no excessive AP translation less than 10 mm complain about ascending or descending stairs and walking downhill. Mochizuki et al. 22 demonstrated that more than 7 mm of mid-flexion AP laxity can cause feeling of instability. In this study, patient with “fair” stability showed greater ROM but poor KS scores. This finding suggests that TKA with firm mid-flexion stability is more related to better patients’ satisfaction than greater ROM.
Our study has limitations. First, selection bias may have existed because implant selection was not performed randomly. Second, stability assessment was somewhat subjective. To overcome this limitation, we tried to collect data by using the same standard consistently. Three physical examinations were conducted by three different orthopedic surgeons in every patient. The final decision regarding stability was made based on consensus between the three orthopedic surgeons. Moreover, one previous study demonstrated that highly positive correlation was found between clinical AP grading by surgeon and quantification using navigation system. 27 Third, our study was a retrospective study, and therefore, a larger randomized controlled study is needed in the future. Third, this study evaluated the mid-term results; hence, the longevity of TKA could not be assessed. A long-term follow-up study is needed. Despite these limitations, to the best of our knowledge, this study included the largest number of cases to compare between the fixed-bearing PS TKA and the fixed-bearing UC TKA and is the first study that investigated correlation between AP stability and ROM in UC design TKA.
Conclusion
TKA with an UC insert provided similar postoperative outcomes when compared to TKA with a PS insert. In addition, mild mid-flexion instability induced greater ROM, but inferior KS score after PCL substitutes TKA regardless of implant design.
Supplemental material
Supplemental Material, Appendix_1_(2) - Similar outcomes between ultracongruent and posterior-stabilized insert in total knee arthroplasty: A propensity score-matched analysis
Supplemental Material, Appendix_1_(2) for Similar outcomes between ultracongruent and posterior-stabilized insert in total knee arthroplasty: A propensity score-matched analysis by Sung-Sahn Lee, Jaewoo Yeom, Dae-Hee Lee and Young-Wan Moon in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by B.Braun.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.