
Abstract
The association between carpal tunnel syndrome (CTS) and remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome, an elderly onset rheumatic disease, is not fully understood. Here, we describe a case of acute CTS caused by RS3PE syndrome. An 84-year-old man visited the hospital with sudden onset of severe neuralgia in the median nerve and pitting edema in both hands. Computed tomography showed low-density areas around the flexor tendons and median nerve compression in the carpal tunnel. Rapidly progressing intolerable neuralgia and paralysis required urgent carpal tunnel release in the left hand. After surgery, we considered the possibility of RS3PE syndrome and started the administration of prednisolone. The pitting edema and neuralgia improved. In this case, imaging and intraoperative findings suggest that the effusion generated from flexor tenosynovitis associated with RS3PE syndrome increased the internal pressure in the carpal tunnel rapidly, which led to acute CTS and urgent surgery.
Introduction
Carpal tunnel syndrome (CTS) is a chronic compressive neuropathy of the median nerve, 1 with most cases being idiopathic. 2 Acute CTS with the rapid onset of median neuropathy has many potential causes, usually related to hematomas due to trauma such as distal radius fractures or wrist injuries. 3 –6 However, in rare cases, the cause of acute CTS is atraumatic, rendering diagnosis and treatment difficult. 1,6,7
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome is an elderly onset rheumatic disease characterized by symmetrical synovitis of the hand and ankle with pitting edema, an acutely elevated inflammatory response, a negative test result for rheumatoid factor, and an excellent prognosis. 8,9 Although some case series studies on RS3PE syndrome have suggested an association between RS3PE syndrome and CTS, 10,11 no studies have described the pathological state and detailed treatment course.
Here, we report a case of acute bilateral progressive CTS caused by RS3PE syndrome. Although the patient’s response to treatment with prednisolone was favorable, urgent surgical carpal tunnel release was required due to progressive intolerable neuralgia and paralysis.
Case presentation
An 84-year-old man presented to our hospital with a chief complaint of sudden onset severe pain in the left hand, which began the previous night. The patient had a medical history of membranous nephropathy diagnosed 5 years prior, which was treated with prednisolone. This course of treatment was completed 2 months prior to his visit to our hospital. There was no history of trauma. With respect to physical findings, swelling of the entire left hand was observed (Figure 1), and Kanavel’s Four Signs 12 were all positive. Strong neuralgia and sensory loss were observed in the median nerve area of the left hand, and opposition of the thumb was difficult. In addition, slight swelling and numbness were also observed in the right hand. Blood tests revealed elevated inflammatory responses with 13,000 μL−1 white blood cell (WBC) and 12.3 mg/dL C-reactive protein (CRP). Computed tomography (CT) showed low-density areas around the flexor tendons, and the median nerve was compressed in the carpal tunnel (Figure 2). Based on these findings, we suspected left flexor tenosynovitis and associated acute CTS. Neuralgia and paralysis rapidly progressed in the patient’s left hand; therefore, emergency carpal tunnel release was performed on the same day. An axillary nerve block was performed, and a tourniquet was used. A skin incision was made along the thenar crease distally, and a zigzag skin incision was made proximally (Figure 3(a)). The palmar aponeurosis and flexor retinaculum were resected, and the carpal tunnel was released. A large amount of effusate was drained during the carpal tunnel release (Figure 3(b)). The median nerve was thin and flattened (Figure 3(c)), and the deep layer of the median nerve contained flexor tendons with synovial hyperplasia (Figure 3(d)). In particular, hyperplasia of the synovial membrane was notable in the middle finger and around the ring finger flexor digitorum profundus tendon (Figure 3(e)), which was excised as much as possible (Figure 3(f)). The carpal tunnel was washed with 1 L of physiological saline, a drain was indwelt, and the wound was closed. Bacteria were not detected in the culture of the effusate that was drained during the surgery.

Appearance of the left hand in this case. The entire left hand was swollen, and the fingers were held in slight flexion.

(a) At the level of the metacarpals, computed tomography images demonstrated low-density areas around the flexor tendons on both sides, predominantly on the left side. (b) At the level of the carpal bones, low-density areas were also observed around the flexor tendons on both sides, predominantly on the left side, suggesting the possibility of compression of the median nerve in the carpal tunnel. R: right; L: left; CT: computed tomography.

Intraoperative findings of surgical carpal tunnel release. (a) A skin incision was made along the thenar crease distally and a zigzag skin incision was made proximally. (b) A large amount of effusate was drained simultaneously during carpal tunnel release. (c) The median nerve was flattened, and (d) the deep layer of the median nerve contained flexor tendons with synovial hyperplasia. (e) Hyperplasia of the synovial membrane was notable in the middle finger and around the ring finger flexor digitorum profundus tendon, which was excised as much as possible (f).
After the surgery, the pain in the left hand was relieved, and the effusion around the flexor tendons decreased, as shown by postoperative magnetic resonance imaging (MRI) performed 2 days after the surgery (Figure 4), thereby confirming decompression of the median nerve. However, pitting edema of the dorsum of the right hand and ipsilateral neuralgia in the median nerve area began to worsen 1 day after the surgery. MRI revealed effusion around the flexor tendons, which were compressing the median nerve (Figure 5). Acute CTS associated with flexor tenosynovitis was also suspected in the right hand; however, since the symptoms were milder compared to the left hand, we ordered the patient to rest and elevate his hand.

MRI scans of the right hand. (a) The T2-weighted axial image revealed a high-intensity area around the flexor tendon, which suggested flexor tenosynovitis. (b) Flexor tenosynovitis created the exudative fluids within the carpal tunnel, which compressed the median nerve at the level of the hook of hamate. MRI: magnetic resonance imaging.
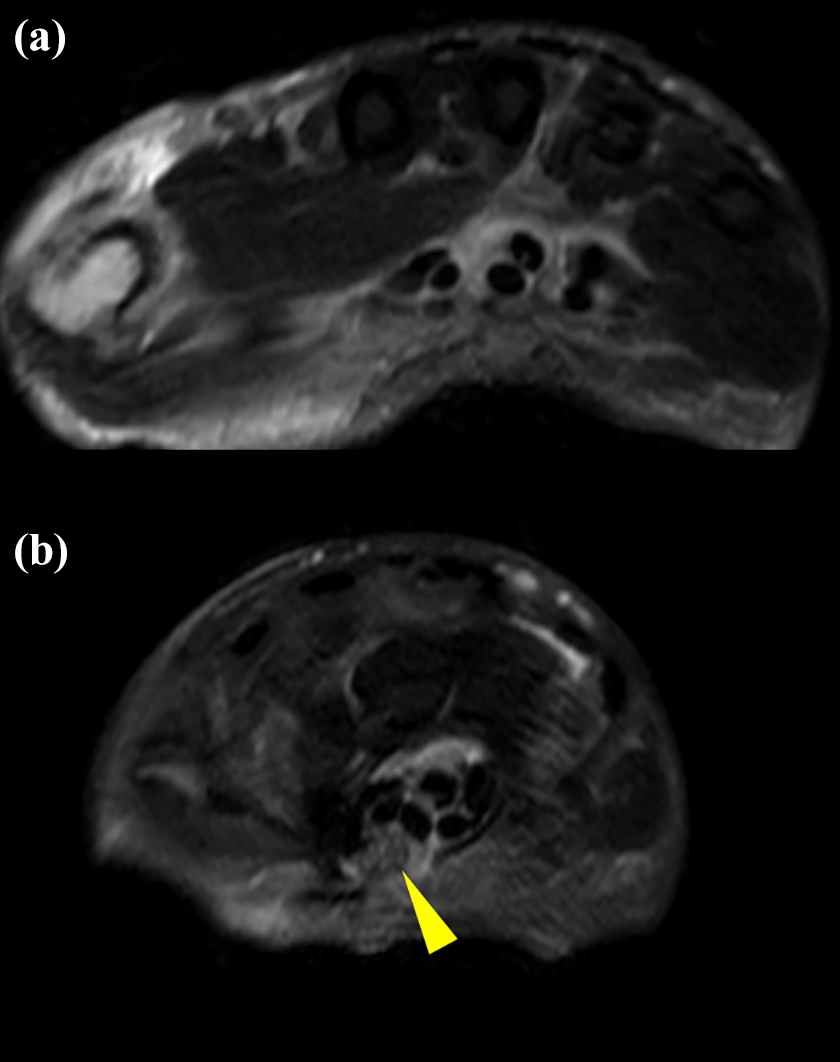
MRI scans of the left hand after the carpal tunnel release revealed decompression of median nerve (arrowhead) (a and b). MRI: magnetic resonance imaging.
This patient presented with bilateral flexor tenosynovitis and pitting edema that progressed over several days. His blood tests were negative for rheumatoid factor, and he did not present with bone erosion on a CT scan, suggesting the possibility of RS3PE syndrome. Since RS3PE syndrome has been reported to be associated with malignancies, 10,13 –16 this patient was also probed for tumors; however, no findings suggestive of malignancy were found.
Administration of prednisolone at a dose of 15 mg/day was started 3 days after the surgery. Bilateral pitting edema and neuralgia improved, blood tests revealed 8500 μL−1 WBC and 2.18 mg/dL CRP, and the patient was discharged from the hospital 20 days after the surgery.
Five months after the surgery, the symptoms suggestive of flexor tenosynovitis and neuralgia in the median nerve area disappeared.
Discussion and conclusion
The present case indicated two clinical issues. First, this case demonstrated the importance of considering the possibility of RS3PE syndrome as one of the differential diagnoses associated with atraumatic acute CTS. Acute CTS is uncommon and may have various causes, such as trauma, infection, inflammatory response, coagulopathic factors, oncologic factors, iatrogenic factors, anatomic factors, or fluid shifts. 1,6,7 Acute CTS generally develops due to numerous fluid and space-occupying lesions, such as hemorrhages, edema, purulence, tumors, or inflammatory pathologies, which rapidly increase the pressure within the carpal tunnel and cause ischemia of the median nerve. 1,6,7 In cases of intracarpal canal sepsis and pyogenic tenosynovitis, expansive purulent fluid in the carpal tunnel compresses the median nerve directly. 17,18 Previous studies on RS3PE syndrome have reported that 22–38% of patients with RS3PE syndrome also had CTS, 10,19 suggesting an association between RS3PE syndrome and CTS; however, no studies have described the pathological state and detailed treatment course for such cases. In this study, imaging and intraoperative findings suggested that the effusate generated from flexor tenosynovitis associated with RS3PE syndrome increased the internal pressure in the carpal tunnel and compressed the median nerve, which led to acute CTS. RS3PE syndrome has also been associated with malignancies, 10,13 –16 and, therefore, screening for potential malignancies is required at the initial diagnosis. Since acute CTS can be the initial manifestation of RS3PE syndrome, as was the case in our patient, early detection and treatment are necessary.
Second, this case suggested that flexor tenosynovitis and CTS associated with RS3PE syndrome respond favorably to prednisolone; however, urgent surgical treatment is indicated when rapid progression of intolerable neuralgia and paralysis is observed. Previous reports of CTS associated with RS3PE syndrome reported good responses to glucocorticoid treatment. 19 However, in the present case, rapidly progressing unilateral paralysis and intolerable neuralgia required urgent carpal tunnel release; the patient maintained a favorable clinical outcome after surgery combined with postoperative prednisolone treatment. The timing of surgery for acute CTS may be crucial, as certain studies have reported that delayed intervention (36–96 h after onset) was associated with permanent consequences 4,20 ; other studies recommend immediate carpal tunnel release (within 8 h of onset) based on results in experimental models, 21,22 suggesting a consensus in favor of relatively early decompression. In the present case, carpal tunnel release was performed 12 h after the onset of symptoms and, fortunately, the patient’s neuralgia and paralysis improved. Because the onset of RS3PE syndrome is sudden and symptoms often mature within 1–2 days, pain and paralysis due to CTS may progress before the treatment initiation, as was the case in our patient. Therefore, it is important to consider the possibility of RS3PE syndrome as a differential diagnosis for acute CTS and perform carpal tunnel release as needed.
In summary, this case provides important information on the association between acute CTS and RS3PE syndrome. Given that acute CTS that is associated with RS3PE syndrome can require urgent surgical management due to the rapid progression of symptoms, it is essential to consider the possibility of RS3PE syndrome in the differential diagnosis for acute progressive CTS.
Footnotes
Consent for publication
Written informed consent for publication of this case report and any accompanying images was obtained from the patient. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.