
Abstract
Introduction:
Surgical intervention through the ‘triangle of auscultation’ is less morbid to patients, as it is devoid of muscles and provides an easy access to tumours arising on the ventral aspect of scapula especially near inferior angle.
Method:
Three patients presented to us with pseudo-winging of scapula and an audible thud on abduction of the arm. A bony mass, painful in two and painless in one patient, was palpable along the anterior aspect of the inferior angle of scapula. A clinical diagnosis of osteochondroma was made which was corroborated by X-rays and computed tomography (CT) imaging. Ventral scapular osteochondroma excision is challenging due to multiple muscle attachments, requiring extensive soft tissue dissection and muscular release. Numerous blood vessels and nerves in the vicinity may also add to the degree of difficulty. This necessitates the need of a minimally invasive and muscle-sparing procedure. We hereby describe a novel surgical approach to the ventral aspect of scapula through the triangle of auscultation for excision of scapular osteochondroma.
Results:
Pseudo-winging disappeared following surgery. Snapping of the scapula resolved with early, full shoulder range of motion. Quick disabilities of arm, shoulder and hand (DASH) score improved from mean 20.2 preoperatively to 0 postoperatively at 3 months in all the patients.
Conclusion:
The approach is simple with minimal blood loss as it does not involve splitting or cutting of trapezius, rhomboid major or subscapularis muscles.
Keywords
Introduction
Osteochondromas are benign tumours, most commonly distributed along the metaphysis of long bones.
1
Their occurrence in the scapular region is rare but still they are the most common primary benign bone tumours of scapula,
2
predominantly located on the ventral aspect of scapula (63%).
3
The symptoms arising from scapular osteochondromas are because of direct pressure on the overlying anatomic structures or indirectly by reactive bursitis with the former causing snapping scapula syndrome leading to restriction in range of motion. Snapping scapula syndrome is painful grating, audible or snapping sensation of scapula due to the friction between back of ribs and ventral aspect of scapula, leading to the disruption of normal scapulothoracic mechanics, mainly during abduction and internal rotation of arm. However, mass effect may cause static pseudo-winging of scapula which may be cosmetically unacceptable to the patient. Dorsally located osteochondromas may cause discomfort in lying supine, whereas lateral location may cause subacromial impingement syndrome. Rarely rapid increase in the size of swelling associated with pain may be suggestive of malignant transformation. Postoperatively patients with ventral scapular osteochondroma presented with disruption of normal scapulothoracic mechanics.
4
Therefore, it may be wise to minimize tissue dissection and preserve muscle attachments in an attempt to preserve the normal scapulothoracic rhythm. We resected three ventral scapular osteochondromas through the triangle of auscultation without splitting and cutting any muscle, over the last 2 years, leading to rapid and natural healing.
Patient information: Written informed consent taken for the publication of images and patient information.
Three patients presented to us with a unilateral, bony hard swelling in the scapular region, gradually increasing in size (Figures 1(a), 2(a) and 3(a)). There was no history of trauma or constitutional symptoms in any of these cases with no significant family history. The salient features have been presented in Table 1.

Patient 1: (a) preoperative picture showing static pseudo-winging of left scapula. (b) CT scan showing bony pedunculated mass arising from the medial border of scapula on ventral aspect. (c) Intraoperative image showing osteochondroma and its stalk.

Patient 2: (a) preoperative picture showing static pseudo-winging of left scapula. (b) and (c) X-ray and CT scan showing bony pedunculated mass arising from the medial border on the ventral surface of the inferior angle of scapula with pressure deformation of ribs.
Salient features.

Y: year; F: female; M: male.
Clinical findings: All the three patients had bony hard swelling on the ventral aspect of scapula, palpable under the medial border of scapula to which it was attached. The range of shoulder abduction was comparable with the normal side but was associated with grating sensation. Overlying skin did not have any venous engorgement, redness/erythema, scar or ulcer. The local temperature was normal. There was no distal neurovascular deficit.
Diagnosis
X-rays were done especially scapular Y view to look for the osteochondromas and contrast-enhanced CT scan was done to delineate their size, location and margins (Figures 1(b), 2(b) and 2(c)).
Surgical procedure
Excision of osteochondroma was performed using the triangle of auscultation approach in all cases. Under general anaesthesia, the patient was put in a prone position. A parascapular incision was made parallel to the medial border of the left scapula (Figure 3(b)). The fascia overlying the trapezius muscle was incised (Figure 4(a)) and the muscle was retracted supero-medially (Figure 4(b)). The latissimus dorsi muscle was retracted inferiorly to enlarge the triangle of auscultation. The rhomboid major muscle was identified forming the floor of the triangle of auscultation. The fibrous insertion along the medial border of the scapula was detached using blunt dissection, leaving the fleshy insertion at the inferior angle undisturbed. The muscle was retracted medially to expose the underlying osteochondroma (Figures 1(c) and 4(c)) on the ventral aspect of scapula. It was observed intraoperatively that in all the patients, the subscapularis muscle had been breached by the osteochondroma arising from the ventral aspect of scapula (Figure 5). The osteochondroma was excised along with its stalk extraperiosteally with the help of an osteotome (Figure 6). Haemostasis was achieved. The rhomboid major and trapezius were allowed to fall back in place without suturing. Skin incision was closed directly using staples. The resected specimen was sent for histopathological evaluation, which confirmed the diagnosis of osteochondroma.

Patient 3: (a) preoperative picture showing static pseudo-winging of right scapula. (b) Skin marking of medial parascapular incision.

(a) Fascia overlying the trapezius muscle being incised. (B) Trapezius muscle retracted supero-medially. (c) Rhomboid major muscle retracted medially.

Subscapularis muscle dissected due to the mass effect of osteochondroma.

Excised osteochondroma with periosteum and cartilage cap.
Follow-up and outcomes
The approach was simple and quick. The patients were discharged the subsequent day after surgery.
Pseudo-winging disappeared following surgery. Snapping of the scapula resolved with early, full shoulder range of motion. Quick DASH score improved from a mean of 20.2 preoperatively to 0 postoperatively at 3 months in all the patients. The patients at 1-year follow-up showed no functional deterioration. Maximum follow-up is 2 years and minimum follow-up is 1 year.
Discussion
Tumours involving the ventral surface of the scapula are rare, commonly generating pseudo-winging, snapping and at times may be painful. Excision of osteochondromas that arise from the ventral aspect of scapula is challenging due to the numerous muscle origins and attachments, thereby causing extensive soft tissue dissection and multiple muscular detachments. This necessitates the need of a minimally invasive and muscle-sparing procedure. We hereby describe a novel surgical approach to the ventral aspect of the scapula through the triangle of auscultation for excision of scapular osteochondromas. The triangle of auscultation is so named because deep to it, on the left side is the cardiac orifice of the stomach, where the splash of swallowed liquid was timed in cases of oesophagal obstruction in pre-Roentgen days. It is bounded superiorly and medially by the lateral border of the inferior portion of the trapezius, inferiorly by the upper border of the latissimus dorsi and laterally by the medial border of the scapula. The rhomboid major muscle forms the floor of this triangle. 5
Morphologically osteochondromas vary in size between 1 cm and 20 cm and have a cartilage cap that is usually less than 2 cm in thickness. 6 A cartilage cap less than 1 cm in thickness indicates a benign condition, a cap between 1 and 2 cm is objectionable and a cartilage cap thicker than 2 cm mostly corresponds to malignant conversion. 7 The cartilage resembles a disorganized growth plate undergoing endochondral ossification. The inner portion of the head and stalk is made by newly formed bone. Cortex and central region of the stalk merge with the cortex and medullary cavity, respectively, of the host bone. 6
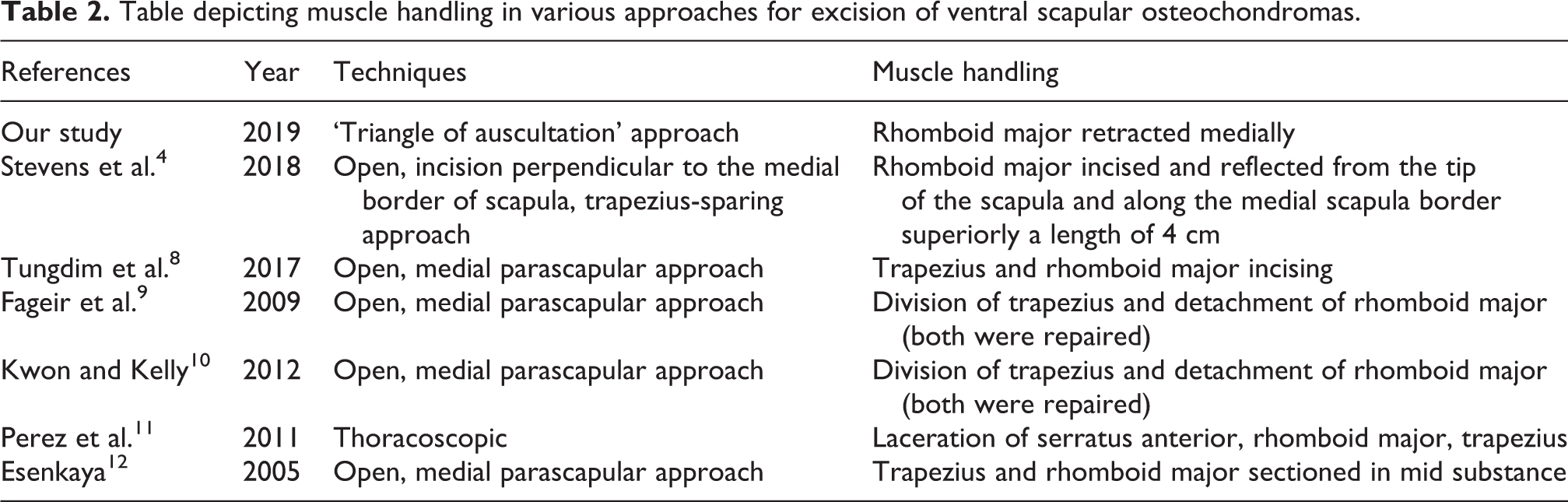
Various surgical approaches have been described to excise ventral scapular osteochondromas (Table 2).
Table depicting muscle handling in various approaches for excision of ventral scapular osteochondromas.
We excised ventral scapular osteochondromas through the ‘triangle of auscultation’. The triangle of auscultation approach has been used by cardiothoracic surgeons for thoracotomies because of its decreased morbidity in comparison to the conventional thoracotomy. This relatively avascular zone provides a safe, quick approach with satisfactory operative exposure, good functional and cosmetic results.
Since the location of the osteochondroma in our cases was on the ventral surface of the inferior angle of scapula, it presented an opportunity to adopt the triangle of auscultation approach for exposing the osteochondroma in these patients. The muscles encountered in the exposure were the trapezius, rhomboid major and subscapularis.
The trapezius was superficial and had no attachments in this triangular area and thus could be retracted medially. The trapezius is followed by the rhomboid major which arises from four thoracic spines (second to fifth) and the intervening supraspinous ligaments. It is inserted into the scapula, extending from the inferior angle to the upper part of the triangular area at the base of the scapular spine. A fibrous arch receives the fibres of the muscle between these two points. The fibrous arch is often only loosely attached to the vertebral border of the scapula except at its ends. Hence, it is easy to retract the rhomboid major muscle after mobilization by merely using blunt dissection. The fibrous arch is relatively less vascular so even if sharp dissection is required, the surgical muscle trauma and blood loss are likely to be minimal. The subscapularis muscle arises from the medial 3/5th of the ventral surface of the scapula. 4 An osteochondroma arising from the ventral aspect of scapula may breach the muscle gradually due to the dynamics of growth of the bone tumour or due to the muscle undergoing slow local attrition as it gets pinched between the osteochondroma and the rib cage. The latter possibility is supported by the deformity of the ribs due to the pressure effect exerted by the osteochondroma. This natural dissection of the subscapularis obviated the need for any further surgical division (Figure 5).
A similar approach has been described by Stevens et al. 4 However, the skin incision used was perpendicular to the medial border of the scapula, which may be a cosmetic concern for the patient. The fleshy insertion of the rhomboid major was incised and reflected from the tip of the scapula and along the medial scapula border superiorly for a length of 4 cm necessitating re-suturing. The longitudinal incision used in our approach made it extensile and cosmetically better. Moreover, the rhomboid major was not incised at its fleshy inferior insertion and merely retracted. Hence, the triangle of auscultation approach used by us involved lesser soft tissue trauma and concomitant blood loss. The quick and complete recovery of shoulder function supported its use.
Conclusion
Triangle of auscultation offers a quick, safe and minimally invasive anatomical corridor particularly suitable for osteochondromas arising from the ventral aspect of the scapula.
Footnotes
Authors’ note
Investigations were performed at the Department of Orthopaedics, Maulana Azad Medical College and Lok Nayak Hospital, New Delhi, India.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.