
Abstract
Background:
The Trauma Expectation Factor Trauma Outcomes Measure (TEFTOM) questionnaire is a self-administered, patient-rated outcome measurement questionnaire designed to measure both ‘expectation’ and ‘outcome’ in orthopaedic trauma patients using two subsets of 10 items. We aimed to validate this instrument in a culturally diverse cohort of patients recruited from Asian and European regions.
Methods:
A total of 193 adult patients with surgically treated AO Foundation/Orthopaedic Trauma Association types 43 and 44 ankle malleolar and distal tibia fractures were recruited with 158 followed up till 1 year. Expectations were assessed prior to surgery, at 2 weeks and after 6 months using the trauma expectation factor (TEF) score. Outcomes were evaluated at 2 weeks, 6 and 12 months using the trauma outcome measure (TOM), American Academy of Orthopaedic Surgeons (AAOS), foot and ankle outcome score (FAOS) and short form-36 (SF-36) questionnaires. Psychometric properties of TEFTOM were assessed.
Results:
TEF and TOM demonstrated good internal consistency (Cronbach’s α > 0.87) and reliability at all time points (intra-class correlation coefficients > 0.90). TOM showed strong correlations (R 2 ≥ 0.60) with the AAOS foot and ankle score, all FAOS subscales, except ‘symptoms’ and SF-36 physical functioning, role physical, bodily pain, social functioning and the physical component summary at 6 and 12 months. Effect sizes for TOM were 2.30 and 0.74 from 2 weeks to 6 months and from 6 months to 12 months, respectively. The baseline patient TEF was predictive for the 1-year TOM score.
Conclusions:
TEFTOM demonstrated good psychometric properties in this cohort of patients with ankle fractures. The TEF ‘expectation’ score was predictive of the TOM ‘outcome’ score. We recommend researchers and clinicians to utilize TEFTOM when patient expectation measurement is concerned for orthopaedic trauma patients.
Introduction
In healthcare, the association between patient expectation, treatment outcome and overall satisfaction has been suggested for painful musculoskeletal conditions, including back pain, knee and hip arthritis, rotator cuff syndrome and finger joint arthritis. 1 –6 Some studies have demonstrated that patients with positive expectations are more likely to experience better outcomes. Moreover, fulfilment of expectations may constitute overall patient satisfaction. 6 –10 Understanding the nature, extent and implications of patient expectation and its relationship to outcomes and satisfaction are increasingly identified as important in treatment delivery. 4
In the context of modern patient-centred care, validated patient-reported outcome measures (PROMs) are widely implemented in research and quality assurance. 11 –15 Some examples of PROMs that measure ‘expectation’ in musculoskeletal conditions include the 13-item Expectations for Complementary and Alternative Medicine Treatments questionnaire, 16 the 20-item hospital for Special Surgery Hip Replacement Expectations Survey, the 17-item Knee Replacement Expectations Survey 17,18 and the 20-item Patient Reported Fulfilment of Expectation (PROFEX) questionnaire. 10
The TEFTOM questionnaire
The TEFTOM is designed as a self-administered expectation and outcome measurement tool, designated specifically for orthopaedic trauma, indexed as a single score describing expectation and outcomes. The questionnaire, which was developed by a team of surgeons with support of the AO Foundation, was the first tool developed specifically to assess ‘expectation’ in orthopaedic trauma. The English version was multi-institutionally validated in the American continent. 19
Unique to the TEFTOM, the questionnaire consists of 2 matched, 10-item subsets (total of 20 items). Separately, the trauma expectation factor (TEF) measures ‘expectation’ while the trauma outcome measure (TOM) assesses ‘outcome’. Five domains that are regarded most relevant to orthopaedic trauma—pain, physical function, disability, injury satisfaction and overall satisfaction, as defined by Deyo et al. 20 and Bombardier et al. 21 —are measured. Similar to the PROFEX tool which also measures ‘expectation’ and ‘outcome fulfilment’ using matched question items, 10 items within the TEF and TOM are matched to assess either expectation or outcome in a specific domain. As such, ‘fulfilment of expectation’ can be determined by comparing prior expectation and eventual outcome, which in turn can be useful in defining success or failure of a treatment.
For example, question 1 in TEF ‘How painful do you expect your injury to be in 1 year?’ is correspondingly composed in TOM as ‘How painful is your injury today?’. For each question, a 5-point rating scale (from 0 to 4) is used. Finally, an overall sum from 0 (lowest expectation/outcome) to 40 (highest expectation/outcome) is calculated. The English version of the TEFTOM questionnaire is available at https://aotrauma.aofoundation.org/ (see also Online Supplementary Material).
The aim of this study was to test the psychometric properties of the German, Spanish and Chinese TEFTOM questionnaires. Criterion validity of TOM against foot and ankle region-specific and general quality of life PROMs, its repeatability (test–retest reliability), responsiveness and internal consistency were determined. We also evaluated whether TEF scores may have predicted eventual TOM scores and other PROM outcomes.
Patients and methods
Study design and patients
A prospective multicentre cohort study (clinicaltrials.gov registration number NCT01134354) was set-up in four clinics in Europe (one in Spain, one in Germany and two in Switzerland) and three clinics in Asia (two in China and one in India). Each centre obtained Institutional Review Board approval. Written informed consent was obtained from all participants. Patient recruitment started in April 2011 and ended in January 2013.
Inclusion criteria were the age of 18 or older, a distal tibia or a malleolar fracture classified as AO Foundation/Orthopaedic Trauma Association fracture classification type 43 (distal tibia fracture) or 44 (malleolar fracture), 22 and a schedule for either internal fixation, external fixation or both. Exclusion criteria were previous surgery of the same fracture, multiple fractures, surgery delayed by more than 28 days, any comorbidity that precluded likelihood of bone union, severe dementia or mental health problems hindering the completion of study questionnaires, and participation in any competing clinical research.
All centres followed a standardized recruitment, questionnaire filling and follow-up protocol. As this study mainly assessed the validity of questionnaires and not the treatment-related outcomes, each patient could receive investigations, surgery, post-operative care and rehabilitation protocols at discretion of the treating doctor conforming to the standard practice at each institution.
Questionnaire administration
The outcome questionnaire (TOM) was validated against two foot and ankle region-specific and one general quality of life PROM. These were, namely, the American Academy of Orthopaedic Surgeons foot and ankle outcomes questionnaire (AAOS-FAO), 23 the Foot and Ankle Outcome Score (FAOS) 24 adopted from the Knee Injury and Osteoarthritis Outcome Score 25 and the RAND Short Form-36 (SF-36) general quality-of-life survey. 26 Culturally and linguistically adapted versions of these questionnaires were administered as appropriate.
The expectation questionnaire (TEF) was administered prior to surgery at 2 weeks and 6 months after surgery. The outcome questionnaires (TOM, AAOS-FAO, FAOS and the SF-36) were assessed at 2 weeks, 6 months and 12 months after surgery. All instruments were filled by patients with research personnel facilitating the process. Previous scores were blinded to patients and surgeons and the theoretical relationship between TEF and TOM was not explicitly explained to patients.
Criterion validity
Criterion validity of the TOM questionnaire was assessed by non-parametric correlation (Spearman’s ρ (r s)) against the AAOS-FAO, FAOS subdomains and SF-36 subdomains at 6 and 12 months. Convergent validity (a coefficient above 0.6 indicating a strong correlation) between TOM and the AAOS-FAO, the FAOS pain and activities of daily living (ADL) subscales, the SF-36 physical function (PF) and role physical (RP) dimensions and physical component summary (PCS) was hypothesized.
Internal consistency
Internal consistency was assessed by means of Cronbach’s α 27 for each item within the TEFTOM questionnaire against the total score. Domains with high internal consistency should have a Cronbach’s α coefficient between 0.7 and 0.9, whereas values above 0.9 indicate redundancy. 28,29
Reliability
Patients were randomly invited to participate in the test–retest reliability part of the study at the discretion of recruiting centres but not following a strict randomization protocol and had to complete the TEF and TOM instruments again, 2 to 5 days after their regular visits. Test–retest reliability of TEF and TOM was assessed by intra-class correlation coefficient (ICC). A reliable score should have an ICC of 0.75 or more. 30
Minimum clinically important difference
The minimal clinically important difference (MCID) is used to determine whether a possible change is due to random effect or truly clinically important. Using the distribution-based approach, 31 the MCID was defined through the minimal detectable change (MDC) of TEF and TOM. The 90% and 95% confidence intervals (CIs) of the MDC were calculated by using the standard error of measurement (SEM).
Responsiveness
Responsiveness to change was assessed for TOM and compared to the AAOS-FAO, FAOS and SF-36 by using the effect sizes at 2 weeks, 6 months and 12 months. 32 A value of ≥0.8 was regarded as large effect, ≥0.5 as moderate and ≥0.2 as small. 33,34 The standardized response means (SRM) were used to detect any change as patients recovered from 2 weeks to 6 months, 6 months to 12 months and from 2 weeks to 12 months.
Predictive value of TEF
TEF scores before surgery and at 2 weeks after were correlated (Spearman’s ρ) against the final TOM, AAOS-FAO and FAOS at 1 year. Furthermore, stepwise multivariable regression was performed to determine whether other baseline variables such as age, gender, race or injury details were predictive of the 1-year outcomes. All variables were explored stepwise in univariable analysis and multivariable analyses to account for independent effects.
Sample size estimation
The sample size was estimated according to the objective for a stable regression equation to use TEF as a prediction factor for TOM and other outcomes. In this approach, we estimated that 40 subjects per predictor item were deemed necessary as recommended by Cohen. 35,36 For four predictors, we estimated that 160 subjects with complete follow-up were needed. This resulted in a subject to item ratio of 16 in each of our 10-item questionnaires, which conforms to the recommended practice. 37 Finally, adjusting for a 20% attrition to follow-up, 200 patients had to be enrolled.
Statistical analysis
Statistical analyses were performed using the software SAS version 9.2 (SAS Institute, Cary, North Carolina, USA). All missing items were reported and replaced by the mean of the patient’s responses to the available items. A type one error probability (p value) of <0.05 was considered statistically significant throughout.
Results
Patients and treatment
Of 193 patients recruited, recruitment was shared out relatively fairly by seven institutes, (Bangalore n = 32, Girona n = 16, Hong Kong n = 41, Cologne n = 20, Luzern n = 32, Shanghai n = 25 and Zurich n = 27) and no single cultural entity dominated the patient pool. Patients’ mean age was 44.0 (range 17−81); 53.3% were men. In all, 95 (49%) suffered falls, 35 (18%) were involved in traffic accidents, 33 (17%) were injured during sports and 30 (16%) had other injuries. There were 19 AO type 43, 31 type 44A, 119 type 44B and 24 type 44C fractures. There were six patients with Gustilo grade I and 2 with grade II open fractures. For patients with closed fractures, 52 (28%), 115 (62%), 16 (9%) and 2 (1%) patients had Tscherne grade 0, I, II and III soft tissue statuses, respectively. Thirty-one (16%) received temporary or definitive external fixation.
One hundred fifty-eight patients were seen at 1 year. The average scores and the number of patients who completed questionnaires at each time point are listed in Table 1. The number of adverse events and reoperations for various reasons is listed in Table 2.
Number of patients with questionnaire completion (no missing data) and respective mean TEF, TOM, AAOS-FAO, FAOS and SF-36 scores at respective time points.

TEF: trauma expectation factor; TOM: trauma outcome measure; AAOS: American Academy of Orthopaedic Surgeons; FAOS: Foot And Ankle Outcome Score; AAOS-FAO: American Academy of Orthopaedic Surgeons Foot And Ankle Outcomes questionnaire; ADL: activities of daily living; SF-36: short form-36; PCS: physical component summary; MCS: mental component summary; QOL: quality of life.
a MCS: Including vitality, social functioning, role emotional, mental health.
b PCS: Including physical functioning, role physical, bodily pain, general health.
Adverse events by action taken, and reoperations, patient level, n (%).

TOM criterion validity
Strong correlations (R 2 = 0.60–0.83) were found between TOM and the AAOS-FAO, all FAOS subscales except ‘symptoms’, and the SF-36 dimensions PF, RP, BP, SF and PCS at 6 and 12 months. Thus, the hypotheses of convergent validity were confirmed. Details are listed in Table 3.
TOM criterion validity: Spearman’s ρ correlation coefficient with the AAOS-FAO, FAOS, and SF-36.a,b

TOM: trauma outcome measure; FAOS: foot and ankle outcome score; AAOS-FAO: American Academy of Orthopaedic Surgeons foot and ankle outcomes questionnaire; SF-36: short form-36.
a p ≤0.001 for all values.
b R 2 value of larger than 0.6 is considered strong correlation confirming convergent validity.
c Items for convergent validity in the hypothesis.
Internal consistency
All TEF and TOM items showed good internal consistency with Cronbach’s α values above 0.87. Items 1, 2, 4, 5, 8, 9, 10 of the TEF at 2 weeks and items 4, 7, 9 of TOM at 12 months had Cronbach’s α values 0.91–0.92 indicating borderline redundancy. However, such redundancy was not demonstrated at other timepoints. Details are presented in Table 4.
TEF and TOM internal consistency.

TEF: trauma expectation factor; TOM: trauma outcome measure.
a Number of patients with completed response for item.
b Cronbach’s α if item removed or for total row, the Cronbach’s α including all items.
Reliability
The ICC for TEF was 0.98 (n = 33) at 2 weeks and 0.90 (n = 27) at 6 months. The ICC for TOM was 0.94 (n = 27) at 6 months and 0.93 (n = 27) at 1 year. All values indicated a good reproducibility.
MCID
The 90% and 95% CIs MDC for TEF were 4.25 and 5.06, respectively (SEM = 1.83). The 90% and 95% CIs MDC for TOM were 3.15 and 3.75, respectively (SEM = 1.35).
Responsiveness
Changes for TOM between 2 weeks, 6 months and 12 months were significant (p < 0.001) and are listed in Table 5, together with all other instruments. The effect size of change of TOM was 2.30 (large) from 2 weeks to 6 months, 0.74 (moderate) from 6 months to 12 months, and 3.38 (large) from 2 weeks to 12 months. From 2 weeks to 6 months, only AAOS-FAO, FAOS ADL, and SF-36 PF had larger effect sizes compared to TOM. SRM values were generally comparable.
Responsiveness in TOM, AAOS foot and ankle outcomes instrument, FAOS, and SF-36 between 2 weeks, 6 months and 12 months.a
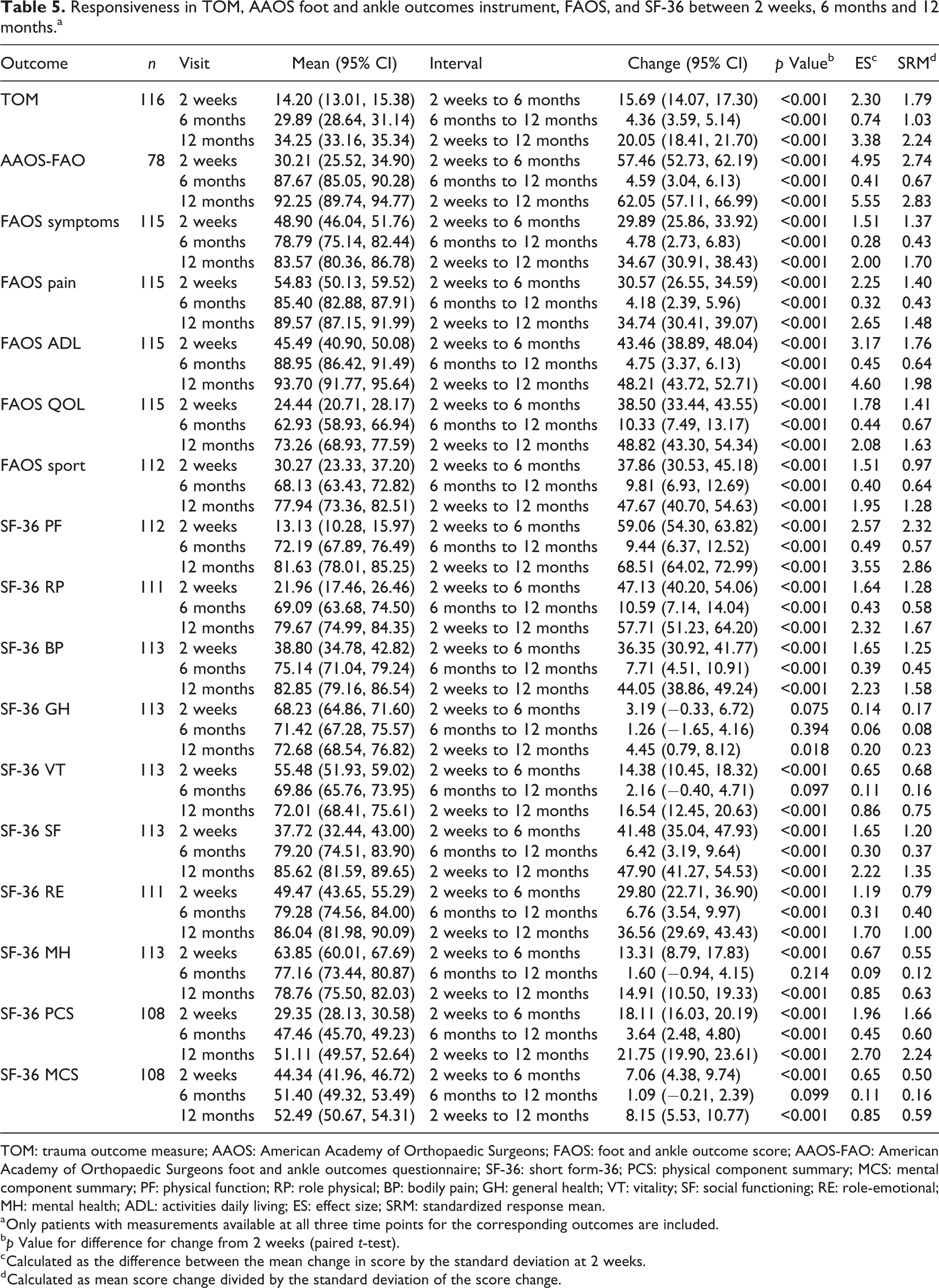
TOM: trauma outcome measure; AAOS: American Academy of Orthopaedic Surgeons; FAOS: foot and ankle outcome score; AAOS-FAO: American Academy of Orthopaedic Surgeons foot and ankle outcomes questionnaire; SF-36: short form-36; PCS: physical component summary; MCS: mental component summary; PF: physical function; RP: role physical; BP: bodily pain; GH: general health; VT: vitality; SF: social functioning; RE: role-emotional; MH: mental health; ADL: activities daily living; ES: effect size; SRM: standardized response mean.
a Only patients with measurements available at all three time points for the corresponding outcomes are included.
b p Value for difference for change from 2 weeks (paired t-test).
c Calculated as the difference between the mean change in score by the standard deviation at 2 weeks.
d Calculated as mean score change divided by the standard deviation of the score change.
Predictive value of the TEF
There was moderate correlation between baseline patient TEF and 1-year TOM scores (r s: 0.43; p < 0.001). The baseline patient TEF was predictive for the 1-year TOM, the 1-year AAOS foot and ankle and all 1-year FAOS sub-scores (p ≤ 0.001).
In a univariable logistic regression model, the baseline patient TEF was predictive for the 1-year TOM scores (CI: 33.6; 35.2, p ≤ 0.001), together with other factors like age, race, income and lawsuit filed. In a multivariable regression model, the factors age and race were confirmed to be predictive on the 1-year TOM scores. For each increase of the TEF score by one point, the 1-year TOM score would be expected to increase by 0.2 points (Table 6).
Association between TOM and potential determinants in univariable and multivariable analysis.

TOM: trauma outcome measure; CI: confidence interval; BMI: body mass index; ORIF: open reduction and internal fixation; EF: external fixation; TEF: trauma expectation factor.
a Interpretation: The multivariable model explains around 32% of the variation observed in the data (R 2).
b From the analysis of variance F-test.
c Results must be interpreted with caution as 45% of patients did not answer.
Discussion
The present study validated the German, Spanish and Chinese TEFTOM questionnaires in patients with ankle fractures. The TOM questionnaire demonstrated good criterion validity, internal consistency, reliability and responsiveness. The TEF demonstrated good internal consistency, reliability and predictive value of the 1-year TOM outcome. The MCID was determined for both TEF and TOM by the distribution-based approach.
The TOM demonstrated a large effect size in change after recovering from surgical treatment. However, higher effect sizes were shown for the AAOS-FAO and the FAOS ADL subscales, indicating a higher performance of these instruments compared to the TOM instrument. Since these instruments were specifically designed for foot and ankle problems, and the TOM is a general trauma outcomes measure, this is a reasonable finding.
In our study, the TEFTOM questionnaire is used only after the patient is informed of his/her realistic condition, surgery and possible recovery. We have confirmed that the initial TEFs at 2 weeks were both predictive of the 1-year TOM, AAOS-FAO and the FAOS. In addition to TEF, age and race were independently predictive for the 1-year TOM scores in the multivariable analysis. An important potential implication in interventional research is that variations in baseline expectations can be taken as ‘background noise’ in interventional studies as they may not truly reflect differences imparted the treatment process. Additional research would be required to better understand these implications.
Suk 38 has demonstrated that less than half of patients with ankle fractures have their expectations fulfilled at 1-year, with ‘fulfilment’ or ‘exceeding’ expectation defined by comparing pretreatment TEF score and the outcome represented by the TOM score. It was noted that social, economic, education and cultural difference can affect patient expectation and the perception of outome. 38 This is consistent with the common understanding that spending time in explanation to reinforce realistic patient expectations and treatment goals may avoid dissatisfaction and litigations.
The application of TEFTOM is of importance in the acutely injured because ‘return to full function’ might be vague, patient-dependent, or overly ambitious. On the contrary, ‘fulfilment of expectations’ may be more realistic as many severe trauma patients never reach their full baseline status again. As seen from the results and in line with other studies in painful musculoskeletal conditions, 1,15 higher baseline expectation correlated with higher eventual outcome scores. However, this also indicates that those with ‘higher expectations’ maybe more difficult to sense ‘fulfilment’ and satisfaction. 2,7 The unique itemwise matching capability of the TEFTOM allows for quantification of ‘expectation fulfilment’ and whether this results in ‘satisfaction’ is an exciting topic for future study.
This study compliments the initial validation study by Suk 19 and has reconfirmed the validity of the TEFTOM tool in another diverse, multicultural and multiregional cohort. We were the first to determine the MCID and confirm the predictive value of the TEF score in the TEFTOM questionnaire. In this article, we reported our results per the study protocol. The complex interplay between baseline variables, such as age, gender, litigation status, cultural and regional background and ‘expectation’ shall be an interesting objective for a future study, perhaps utilizing current data.
Limitations
The limitations include the recruitment of 158 patients with complete data out of a targeted 160, which may minimally impact the statistical power. Test–retest reliability interval was rather short (2–5 days), and patients may have remembered their first answers. The distribution-based approach in determining the MCID is challenged to be simplistic compared to more sophisticated methods, such as the item-response theory method. We were unable to confirm the construct validity of TEF due to the lack of an existing validated questionnaire and confirm whether they indeed matched the same domains measured by the TOM score. The current cohort only validated ankle fracture patients treated by surgery and not by non-operative methods. Further studies will be needed to validate the TEFTOM questionnaire of specific languages and indications.
Conclusion
In conclusion, we have validated the German, Spanish and Chinese TEFTOM questionnaires in patients with ankle fractures. We recommend researchers and clinicians to utilize TEFTOM when patient expectation measurement is concerned for orthopaedic trauma patients.
Supplemental material
Supplemental Material, Appendix_TEF - Evaluation of an expectation and outcome measurement questionnaire in ankle fracture patients: The Trauma Expectation Factor Trauma Outcomes Measure (TEFTOM) Eurasia study
Supplemental Material, Appendix_TEF for Evaluation of an expectation and outcome measurement questionnaire in ankle fracture patients: The Trauma Expectation Factor Trauma Outcomes Measure (TEFTOM) Eurasia study by Christian Fang, Andreas Platz, Lars Müller, Thomas Chandy, Cong-Feng Luo, Josep María Muñoz Vives, Frankie Leung and Reto Babst in Journal of Orthopaedic Surgery
Supplemental material
Supplemental Material, Appendix_TOM - Evaluation of an expectation and outcome measurement questionnaire in ankle fracture patients: The Trauma Expectation Factor Trauma Outcomes Measure (TEFTOM) Eurasia study
Supplemental Material, Appendix_TOM for Evaluation of an expectation and outcome measurement questionnaire in ankle fracture patients: The Trauma Expectation Factor Trauma Outcomes Measure (TEFTOM) Eurasia study by Christian Fang, Andreas Platz, Lars Müller, Thomas Chandy, Cong-Feng Luo, Josep María Muñoz Vives, Frankie Leung and Reto Babst in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
The authors would like to thank Kathrin Espinoza for statistical analysis and Andrea Blumenthal for medical writing services (both employees of AO Clinical Investigation and Documentation).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the AO Trauma Network.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.