
Abstract
Purpose:
This prospective multicenter study evaluated patient reported outcomes (PROs) in individuals undergoing medial open-wedge high-tibial osteotomy (OWHTO) with plate stabilization compared to conservative care or no treatment.
Methods:
One hundred eighteen of 148 patients older than 40 years were elected for OWHTO with plate treatment. Thirty patients declined surgery and were followed as a conservative group. The primary outcome measure was the Knee Injury and Osteoarthritis Outcome Score (KOOS) at 2 years. Secondary measures included Oxford knee score, Western Ontario and McMaster Universities osteoarthritis index, range of motion (ROM), joint space width (JSW), femorotibial angle (FTA), and weight-bearing line ratio (WBLR).
Results:
Patient enrollment and baseline characteristics were heterogeneously distributed and led to group characteristics that were not comparable. Therefore, the comparison of the KOOS between the groups showing no differences must be treated with caution. In the OWHTO plate group, all PROs and the ROM significantly improved between baseline and 2-year follow-up. JSW remained stable in the OWHTO group. The FTA and WBLR significantly changed from a mean of 179.3 (95% confidence interval (CI): 178.7, 179.9) to 169.8 (95% CI: 169.2, 170.5) and from 23.1 (95% CI: 20.7, 25.5) to 62.4 (95% CI 59.0, 65.8), respectively. Treatment failure with conversion to total knee arthroplasty occurred in 1% of the OWHTO group; and in the conservative group, 10% converted to HTO or knee arthroplasty.
Conclusions:
OWHTO with plate leads to significant improvement of PROs and function 2 years after intervention and demonstrates reliable mechanical axis correction with subsequent shift of weight-bearing.
Introduction
Due to genetic predisposition and traditional kneeling posture, 1,2 prevalence of knee osteoarthritis (OA) is high in Japan. Many patients stay active until old age which demand for treatments that allow them to return to near normal function. 3 In patients suffering from medial compartment knee OA, high-tibial osteotomy (HTO) can be used to shift weight-bearing axis to the lateral compartment and improve load distribution, 4,5 thus reducing pain and decelerating medial knee compartment OA progression. 4,6
Medial open-wedge HTO (OWHTO) with plate fixation has shown good outcomes and an adequate risk–benefit ratio. 6 –11 Since patients of East Asia have different tibial geometric dimensions, the TomoFix small plate (Synthes GmbH, Oberdorf, Switzerland) was developed. 12
The primary objective of this study was to evaluate patient reported outcomes (PROs) using the Knee Injury and Osteoarthritis Outcome Score (KOOS) considering functional outcome as the most important factor for patients to assess the success of an operation.
This study tested the null hypothesis that there is no difference in knee function at 2 years, as measured by KOOS, between patients with medial unicompartmental OA and osteonecrosis (ON) of the knee treated with OWHTO with plate versus nonsurgical care. The secondary objectives of this study were to assess additional functional outcomes and surgical and postoperative details, including adverse events and radiological parameters.
Methods
This prospective, multicenter cohort study (NCT01048710) was conducted in nine Japanese hospitals and approved by the local ethics committees. Patients were assessed preoperatively, and follow-up was performed at 1, 3, 6, 12, 24, 36, 48, and 60 months. The primary end point was at 2 years and is presented in this article.
Patients were eligible if they were older than 40 years, had OA grade 1 to 4 (Kellgren–Lawrence) or ON stage 2–4 (Koshino classification), were surgical candidates for OWHTO with TomoFix Small plating, were able to understand and read elementary-level Japanese, agreed to comply with the postoperative management program, and provided informed consent. Detailed exclusion criteria were applied as described by Goldhahn et al.. 14 For patients in the conservative group, HTO on the contralateral side or major surgery on both knees was additional exclusion criterion.
To quantify potential patient benefit, OWHTO was planned to be compared to ongoing conservative therapy as blinding of patients and surgeons was not feasible and random allocation was perceived unethical. The conservative group was composed of patients although indicated for OWHTO preferred to continue with nonsurgical or no treatment. The study protocol did not define the type of conservative therapy used, that is, patients were allowed to continue pain medication, heat therapy, exercise therapy, injections into the knee (hyaluronic acid, corticosteroid), bracing during the study, and in some cases, patients stopped it altogether.
OWHTO treatment
For all patients in the OWHTO plate group, a postoperative anatomical valgus angulation of 10° (femorotibial angle (FTA) of 170°) or restoration of the mechanical axis with a weight-bearing line ratio (WBLR) at 62.5% of the tibial plateau was anticipated. Prior to the operation or at the beginning of it, a knee arthroscopy was performed. In the case of ON, debridement of the detached cartilage at the femoral condyle and drilling were conducted. In OA knees, microfracture procedure or drilling was optionally applied. The OWHTO plate procedure was performed according to Staubli et al. 9 and Lobenhoffer and Agneskirchner. 13
The osteotomy gap was either left empty or optionally filled with β-tricalcium phosphate wedges—OSFERION 60®—(Olympus Biomaterial, Tokyo, Japan).
The postoperative regimen followed the details as previously reported. 14 The plate was removed as part of the standard of care after healing.
Functional outcomes
The primary outcome measure KOOS consisting of five subscales, validated in Japanese patients with knee OA, has demonstrated good psychometric properties. 14,15
Other PROs included the Japanese version of the 12-item Oxford knee score, return to previous sporting activities and the patient-reported ability to sit on the floor in the traditional Japanese sitting style. 14,16 Absolute range of motion (ROM) was assessed using the neutral-zero method and compared to the ROM of healthy, not-affected knee (relative ROM). Length of HTO surgery was measured from incision to closure. The Western Ontario and McMaster Universities OA index (WOMAC score) was calculated from the KOOS as described by Roos. 17
Radiological evaluation
All radiographs were assessed and measured by an independent specialist including the knee OA or ON degree assessed according to the Kellgren–Lawrence and Koshino classification systems, respectively. 18,19 FTA and WBLR 20 were measured. Joint space width (JSW) was measured in the Rosenberg position. 21 at the narrowest part of subchondral bone on both femur and tibia. Radiologically detectable lateral cortex fractures were classified as described by Takeuchi et al. 22
Complication assessment
Patients with OWHTO were screened for predefined anticipated events. Postoperative adverse events were classified into complications around the treated knee including implant/surgery complications, bone complications and soft tissue complications, and general complications in other areas of the body.
Documentation and analysis of the complications were performed according to the published guidelines. 23,24 A study complication review board (CRB) composed by the principal clinical investigator and two study independent experienced knee surgeons performed a final classification and assessment of all complications using case report forms, radiographs, and available clinical data. The complication category “fractures around the lateral cortical hinge (intra- and postoperative)” included events that were reported as “Iatrogenic fracture at implant insertion side,” “Tibial plateau fracture,” “Tibial tuberosity fracture,” “Lateral cortex fracture,” or “Displacement of distal tibial fragment medially because of lateral cortical fracture.” Takeuchi type 1 fractures were rated by the CRB as no complication since the fracture is located in or just proximal to the proximal tibiofibular joint which is strengthened by the capsular ligaments. Takeuchi type 1 fractures generally heal with slight delayed weight-bearing without causing further sequelae.
Sample size calculation and statistical analysis
Sample size calculation was based on a two-sample t-test for each KOOS subscale. Considering a correlation of 0.80 between KOOS subscales, the Dubey and Armitage-Parmar procedure was used to obtain an overall significance level α of 0.05, which would lower the α for each test to 0.0365. Based on an 80% power to detect a 0.67 effect size (i.e. assuming a difference of 20 points divided by a standard deviation of 30) and a 75/25 distribution of patients electing surgery (OWHTO plate group) versus those declining surgery (conservative group), it was estimated that we would need 103 patients (77 and 26, respectively) at the 2-year follow-up examination. To correct for possible attrition of up to 30%, target enrollment was 148 patients.
Analysis was based on intent-to-treat. Missing data were not imputed. To compare KOOS subscales between treatment groups, t-tests were initially used. To adjust for important baseline parameters, regression analyses using the Akaike’s information criterion were performed. P values for the tests for differences in the five KOOS subscales between the groups were adjusted for multiple testing with the Dubey and Armitage-Parmar procedure. Within group change from baseline was analyzed with mixed-effects model for repeated measures with an unstructured covariance or with paired t-test as appropriate. The number and percentage of patients treated with OWHTO who had a particular adverse event are presented and two-sided exact (Clopper–Pearson) 95% confidence intervals (CIs) were calculated for adverse event rates. All statistical analysis was performed with SAS version 9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Of a total of 151 consecutive patients recruited between August 2009 and June 2013, 118 were elected for OWHTO surgery with plate fixation, while 30 chose to join the conservative control group, and 3 patients were ineligible. Enrollment was heterogeneously distributed across the nine clinics.
The mean age was 63.6 years (range 42.0–79.0), and the majority were female (81.1%). The conservative group was significantly younger at baseline (mean 59.0 vs. 64.7 years, p = 0.001). Baseline parameters are shown in Table 1.
Patient demographic (enrolled patients).

OWHTO: open-wedge high-tibial osteotomy; SD: standard deviation.
a Calculated as (“number of cigarettes”/20) × “years of smoking” for both smokers and ex-smokers.
b t-Test.
c χ 2 test.
d Fisher’s exact test.
Twenty-six patients in the OWHTO plate group suffered from both OA and ON, whereas one patient had ON only (Table 2). More severe degrees of OA (Kellgren–Lawrence grade 2–4) were observed in 88 patients (74.5%) in the OWHTO group, compared to 16 (53.4%) in the conservative group, but this difference was not statistically significant.
Baseline distribution of OA degrees (Kellgren–Lawrence classification) and ON degrees (Koshino classification) per group.
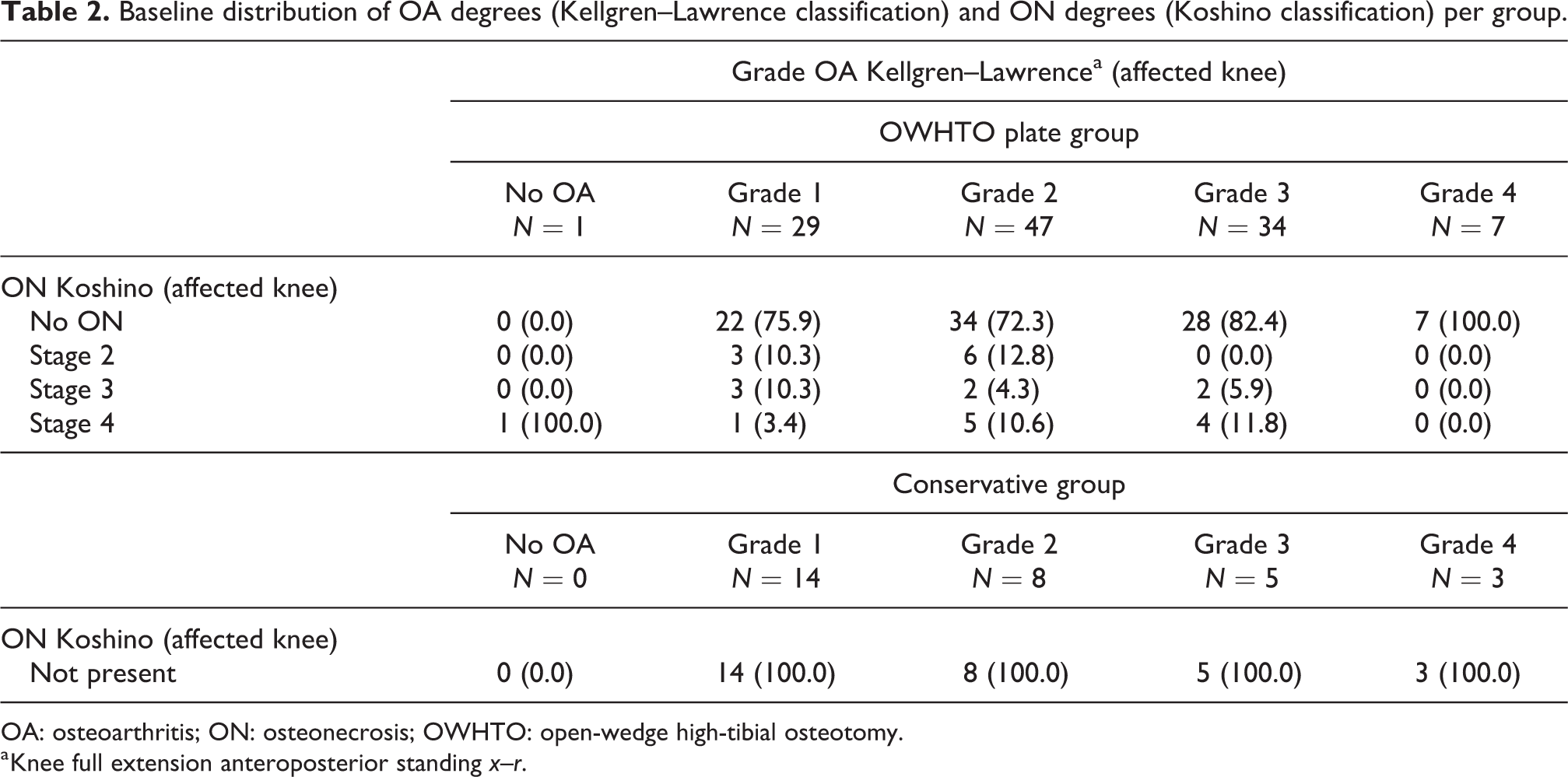
OA: osteoarthritis; ON: osteonecrosis; OWHTO: open-wedge high-tibial osteotomy.
a Knee full extension anteroposterior standing x–r.
Pretreatment characteristics are shown in Table 3.
Pretreatment characteristics (enrolled patients).

OWHTO: open-wedge high-tibial osteotomy; SD: standard deviation; HA: hyaluronic acid; OA: osteoarthritis; ON: osteonecrosis.
a Multiple answers are possible.
b Wilcoxon rank sum test.
At 2 years, 112 patients (94.9%) in the OWHTO plate group and 24 patients (80%) in the conservative group completed follow-up. While all subscales of KOOS had significantly improved in both study arms (Figure 1), no significant difference in the KOOS at 2 years was found between the groups (Table 4), and KOOS profiles are shown in Figure 2.

Mean change in the KOOS between baseline and 2 years (enrolled patients). KOOS: KOOS containing the five subscales pain (Pain), symptoms (Symptoms), function in daily living (ADL), function in sport and recreation (Sport), and knee-related QOL (QOL). The whiskers show the 95% CI. KOOS: Knee Injury and Osteoarthritis Outcome Score; QOL: quality of life; OWHTO: open-wedge high-tibial osteotomy; CI: confidence interval.
Test for difference in KOOS at 2 years between treatment groups (enrolled patients).a

KOOS: Knee Injury and Osteoarthritis Outcome Score; OWHTO: open-wedge high-tibial osteotomy; CI: confidence interval; QOL: quality of life; OA: osteoarthritis.
a The total score of 100 points is the best score, 0 points show the worst score.
b Calculated from linear regression models adjusted for baseline confounders (KOOS pain: BL KOOS pain, age; KOOS symptoms: BL KOOS symptoms, age, VAS general, employment status; KOOS ADL: BL KOOS ADL, age, VAS general; KOOS sport: BL KOOS sport, age, gender, months of OA, chondropenia severity score; KOOS QOL: BL KOOS QOL, age, months of OA, chondropenia severity score). p Value was adjusted for multiple testing according to Dubey and Armitage-Parmar procedure.
c p Value for between-group difference at 2 years (t-test) with adjustment for multiple testing according to Dubey and Armitage-Parmar procedure.

KOOS profiles for the OWHTO and the conservative group at baseline and 2 years. KOOS: KOOS containing the five subscales pain (PAIN), symptoms (SYM), function in daily living (ADL), function in sport and recreation (SPORT), and knee-related QOL. OWHTO: open-wedge high-tibial osteotomy; QOL: quality of life; KOOS: Knee Injury and Osteoarthritis Outcome Score.
Due to the baseline differences between the groups and inhomogeneous distribution of enrollment, further results will be presented separately for each of the two groups.
OWHTO plate group
Mean length of OWHTO surgery time was 84.3 ± 33.5 min (range: 38.0–210.0 min), and the mean maximum width of the osteotomy gap at medial side was 11.2 ± 2.4 mm (range: 6.0–20.0). Bone substitute was used in 27.1% (n = 32) of the cases.
Treatment failure occurred in 1%: One patient with tricompartmental OA had to undergo treatment conversion to TKA because of loss of correction and breakage between the head and the shaft of the B-, C-, and D-screw after 3 months (Figure 3). The CRB identified the wrong position of the plate as its most likely cause. After a mean of 21 ± 4.7 months (range: 5.0–28.0), the plate was removed in all except three patients. The timing of plate removal before (47 patients) or after (62 patients) the 2-year follow-up did not appear to significantly affect the primary outcome.
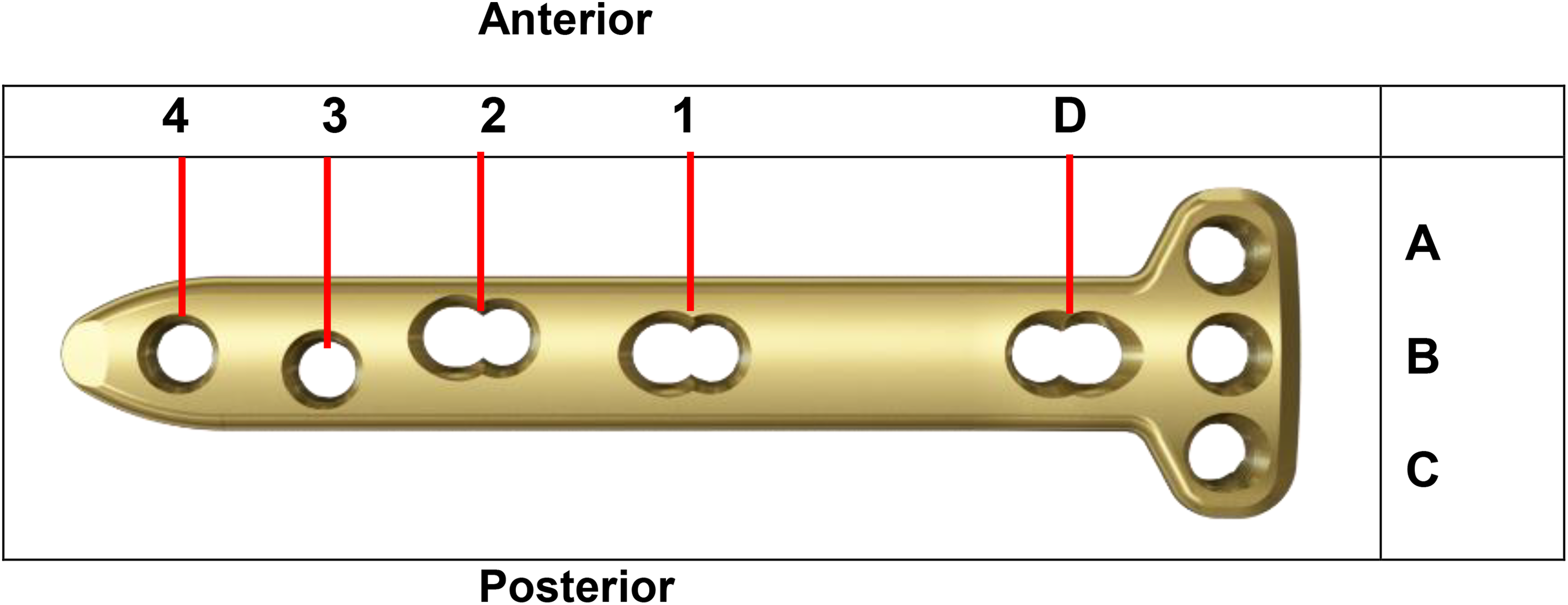
The holes of the TomoFix small plate. A-hole: proximal anterior head screw hole; B-hole: proximal middle head screw hole; C-hole: proximal posterior head screw hole; D-hole: combi-hole for oblique screw; hole 1: proximal combi-hole; hole 2: distal combi-hole; hole 3: proximal hole; hole 4: Distal hole.
As well as all subscales of the KOOS (Figure 1), other PROs and the absolute and relative ROM improved over time (Table 5), too. At 2 years, 90% (n = 27) of patients engaging in sports at baseline were at the same or higher level. The percentage of patients able to sit Japanese style with maximally flexed knees increased three fold from 11.9% to 34.8% (p < 0.001), and 30 patients (26.8%) who were not able to sit in Japanese style at baseline were able to do so 2 years after.
Within groups change from baseline to 2-year follow-up in functional scores and ROM (enrolled patients).a
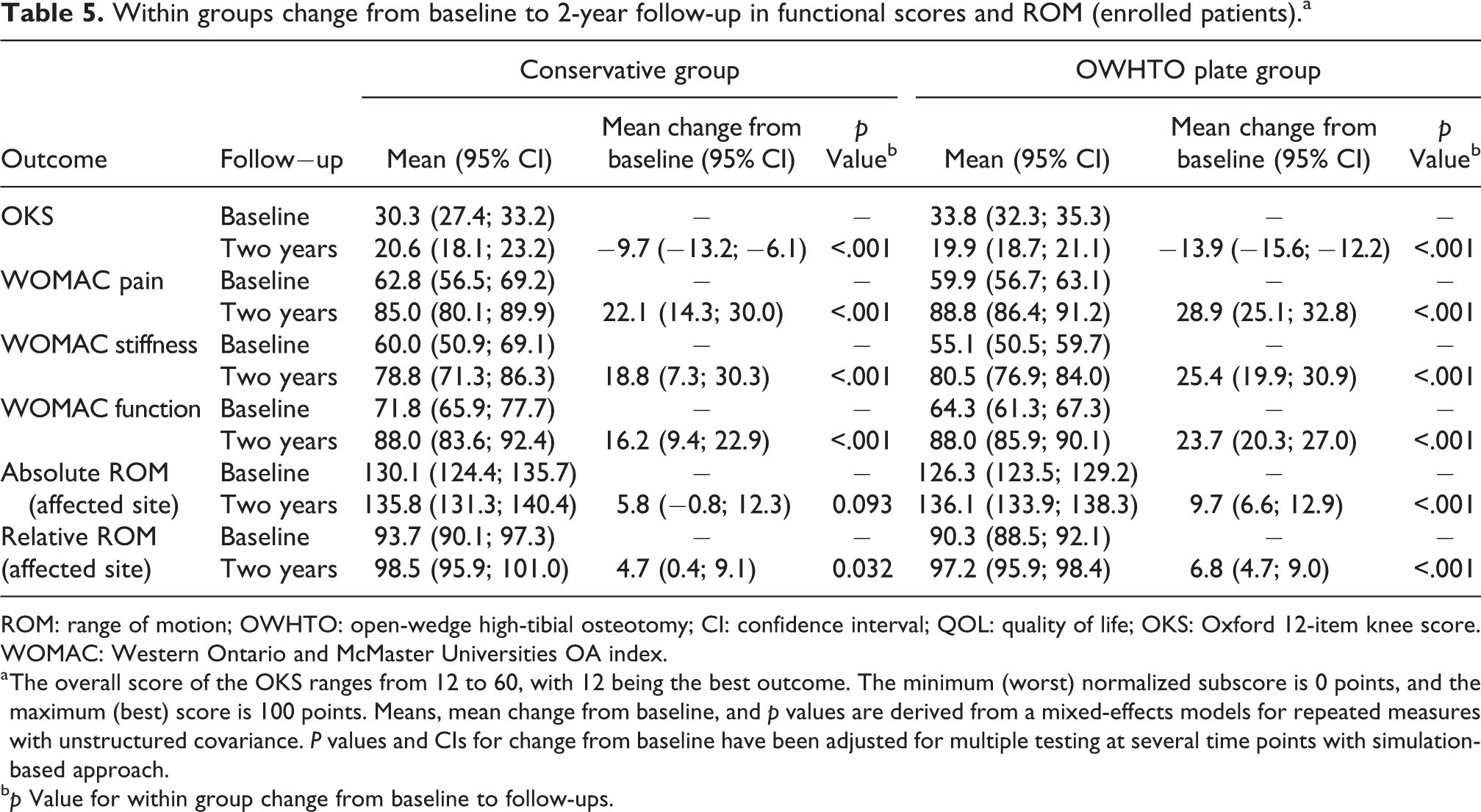
ROM: range of motion; OWHTO: open-wedge high-tibial osteotomy; CI: confidence interval; QOL: quality of life; OKS: Oxford 12-item knee score. WOMAC: Western Ontario and McMaster Universities OA index.
a The overall score of the OKS ranges from 12 to 60, with 12 being the best outcome. The minimum (worst) normalized subscore is 0 points, and the maximum (best) score is 100 points. Means, mean change from baseline, and p values are derived from a mixed-effects models for repeated measures with unstructured covariance. P values and CIs for change from baseline have been adjusted for multiple testing at several time points with simulation-based approach.
b p Value for within group change from baseline to follow-ups.
Radiograph evaluation revealed that JSW remained relatively stable with a mean decrease of 0.11 mm from baseline to 24 months (95% CI: −0.11, 0.34, p = 0.321; Figure 4). FTA and WBLR were improved over baseline and maintained at 2 years (Table 6).

Change in JSW for OWHTO and the conservative group from baseline to 2 years. JSW: joint space width; OWHTO: open-wedge high-tibial osteotomy.
Change of FTA and WBLR between baseline and 2 years.a

FTA: femorotibial angle; WBLR; weight-bearing line ratio; OWHTO: open-wedge high-tibial osteotomy; CI: confidence interval.
a Only patients with measurements at both time points included in table.
b Cases with flexion contracture of >10° at baseline are excluded, as value for FTA is not valid for these cases.
c Paired t-test.
In 53 patients (44.9%), a fracture around the lateral cortical hinge immediately postoperative or within the first postoperative month was radiographically detected: Takeuchi type 1 in 40 patients (33%), Takeuchi type 2 in 9 patients (7.6%), and type 3 in 4 patients (4.3%). There was no difference in the maximum width of osteotomy gap between patients with and without a lateral cortical hinge fracture (mean 11.0 and 11.3 mm, respectively).
During the 2-year follow-up, 44 patients had at least one complication (Tables 7 to 9). Sixteen patients had a fracture around the lateral cortical hinge Takeuchi type 2 or 3 (intraoperative or postoperative) corresponding to a risk of 13.6% (95% CI: 8.0, 21.1). Nonunion-insufficient signs of healing (>6 months) were observed in three patients (2.5%).
Risk of intraoperative complications.a

CI: confidence interval; OWHTO: open-wedge high-tibial osteotomy.
a All OWHTO plate group patients were prospectively screened for these events.
b Only adverse events starting up to <=776 days after surgery are included in the table.
c Number of patients with at least one complication. If a patient experienced multiple complications under any complication class, the patient was only counted once.
d Estimated risk of developing at least one complication (calculated by dividing the number of patients experiencing at least one complication by the total number of patients in the OWHTO plate group).
e CIs for percentages were calculated using the exact method.
Risk of postoperative complications.a

CI: confidence interval; OWHTO: open-wedge high-tibial osteotomy.
a All OWHTO plate group patients were prospectively screened for these events.
b Only adverse events starting up to <=776 days after surgery are included in the table.
c Number of patients with at least one complication. If a patient experienced multiple complications under any complication class, the patient was only counted once.
d Estimated risk of developing at least one complication (calculated by dividing the number of patients experiencing at least one complication by the total number of patients in the OWHTO plate group).
e CIs for percentages were calculated using the exact method.
Risk of general postoperative complications.a

CI: confidence interval; OWHTO: open-wedge high-tibial osteotomy.
a All OWHTO plate group patients were prospectively screened for these events.
b Only adverse events starting up to <=776 days after surgery are included in the table.
c Number of patients with at least one complication. If a patient experienced multiple complications under any complication class, the patient was only counted once.
d Estimated risk of developing at least one complication (calculated by dividing the number of patients experiencing at least one complication by the total number of patients in the OWHTO plate group).
e CIs for percentages were calculated using the exact method.
When most local adverse events were unlikely related to implant, only seven soft tissue events (pain around the plate) were likely related. For the other local events (e.g. fractures around the lateral cortical hinge, screw breakage, loss of correction, delayed healing, and nonunion), the most likely cause was a suboptimal surgical technique. Screw breakage occurred in six patients and was attributed to a wrong plate positioning (too anterior location). One of these cases was the patient described above who had to undergo TKA. All other cases of screw breakage were found at the planned implant removal: four of them occurred at the proximal posterior head screw (C-hole) and one was reported without specification.
All OWHTO plate patients with a local adverse event except two recovered without persistent damage. One patient with chronic regional pain syndrome did not recover from numbness and pain. Another patient with osteomyelitis/deep wound infection had an ongoing recovery; this patient had a history of osteomyelitis 20 years ago because of an open fracture at the lower leg that was osteotomized now.
Conservative group
The majority of the patients in the conservative group (26/30 patients) did not change their previous conservative treatment or received no knee-specific treatment. During the 2-year follow-up, treatment failures occurred in 10% of the patients. Due to continuing pain, two patients underwent OWHTO, and one patient underwent TKA. For data analysis, these patients were included in the 2-year outcome data based on their original group assignment.
All subscales of the KOOS improved significantly between baseline and 2-year follow-up (Figure 1). At 2 years, the other PROs, the relative ROM as well as the ability to sit in Japanese style showed significant improvement (Table 4); 84.6% of patients engaging in sports at baseline returned at 2 years to the same or higher level. The percentage of patients able to sit Japanese style with maximally flexed knees increased from 20% to 62.5% (p < 0.001); 10 patients (41.7%) who were unable to sit in Japanese style at baseline were able to do so 2 years later.
The evaluation of the radiographs revealed a decrease of JSW by an average 0.84 mm between baseline and 2-year follow-up (95% CI: 0.3, 1.38, p = 0.004; Figure 4).
Adverse event information was not collected for patients in the conservative group.
Discussion
In our study, improvements in all KOOS domains exceeded the thresholds for overall pooled smallest detectable change and are therefore not caused by a random error. 25 The KOOS data from the OWHTO versus conservative treatment groups were similar at 2 years and no differences were found. However, only the PRO improvement of the OWHTO group is supported by corresponding structural evidence: The JSW and the planned and corrected mechanical axis after OWHTO remained stable during the 2-year follow-up.
Large and significant changes in the KOOS throughout the 2-year follow-up are known from a study investigating function after osteotomy in patients with medial compartmental OA. 4 Compared to the mean changes reported there, patients in our study showed higher changes for all subscales. Cultural differences in our Japanese patient cohort, an older patient population with a lower body mass index, and a higher percentage of females in our study may explain this difference.
OWHTO group
The surgical goal of shifting weight-bearing from the medial to the lateral compartment was achieved as evidenced by the change in mean WBLR from 23.1% to 62.4%. It meets the definition of desired WBLR reconstruction of 48–70% in other studies and is as accurate as other HTO techniques, even when using navigation. 26,27 A secondary effect of surgical axis correction is that disease progression may be slowed. We observed this in our study as JSW remained relatively stable from prior to surgery through 2 years. The delay of OA progression following OWHTO with plating is also supported by the low rate of conversion to TKA, where the only patient receiving TKA had tricompartmental OA. As the study was designed to assess patients with medial unicompartmental OA and ON of the knee, having patients with a tricompartmental knee OA enrolled in the surgical treatment group should be considered a study limitation which might impact the final result.
While patients’ age in our study is comparable with another study in Japanese OWHTO patients, 28 our patients are more than 15 years older than in other European studies using the same implant in standard size. 6,11,29 Although this suggests a worse functional outcome, we observed a marked improvement in all PROs, ROM, ability to sit Japanese style, and return to sports. This may be attributed to possible cultural differences with high activity at higher age and lower BMI in Japanese patients and is also reported from another HTO study. 10 Our results confirm the short- and mid-term reports by other groups about the positive effect of OWHTO with plate fixation on functional parameters including an accurate and reliable reconstruction of the anatomical axis. 6,29,30 The achieved mean WBLR of 62.4% at 2 years corresponds to the anticipated study target of 62.5% of the tibial plateau and the clinical experiences of other groups. 26,27 This factor may have contributed to the subsequent improvement in PRO.
The adverse events and subsequent treatments observed during this study were overall expected for this patient population and can be compared to other studies using the same implant in standard size. 7,20 A direct comparison of complication types is not possible due to different complication definitions and lack of comparable classifications. 23,31 For example, in one study, 4/40 cases (10%) with superficial infection were reported compared to one case in our study. 7 In contrast, we observed one case with osteomyelitis. The authors consider the history of this patient with previous osteomyelitis as a potential risk factor of postoperative infection. From a retrospective study, Floerkemeier et al. report a risk of 1.5% for healing insufficiency (with a high risk of pseudarthrosis) diagnosed within the first 3 months after surgery, which led to a reoperation to circumvent pseudarthrosis at a later stage. 6 In our study, where we prospectively screened all patients for anticipated complications at all follow-up visits, the risk for delayed healing after 3 and 6 months is higher with 4.2% and 2.5%, respectively. The only implant-related complication in our study was pain around the plate observed in seven patients that was eliminated after implant removal. Although a direct comparison is not possible because of lacking comparable definitions, this is less than the 28 of 69 cases complaining about local irritation associated with a standard size plate reported by Niemeyer et al. 8 The low rate of local irritation in our group suggests that the adaptation of the plate size to the anatomical differences in the Asian population has a meaningful benefit.
Our rate of cortical hinge fractures type 2 to 3 (13.6%) is comparable with the rate from another group (10.8%) with a similar medial opening in all patients with cortical hinge fractures. 28 In contrast to their study, we found no association between fracture occurrence and open-wedge width. In our study, the most likely cause for cortical hinge fractures type 2 and 3 was a suboptimal surgical technique with the plate being placed too anteriorly and the screws directed too posteriorly. Further surgeon training might reduce this complication.
Conservative group
As patients in the conservative group declined OWHTO surgery at the beginning of the study, they may have a different perception of their disease and of surgical procedures in general. The improvement of the outcome scores of this group may attributed to coping strategies and a systematic response shift in PRO. The better functional status at baseline and the less severe disease with no patients suffering from both OA and ON might likewise have contributed to these unexpected results without morphological explanation. In addition, it is known from the literature that a simple arthroscopic lavage, a debridement, or even a sham operation can have an impact on functional outcome. 32
Limitations
The study was not randomized and treatment groups were determined based on patient decision for or against surgery based on ethical considerations. However, it has the potential for enrollment bias, which was confirmed by baseline differences between the groups and site differences in treatment selected. For instance, the majority of patients (76.6%) in the conservative group underwent arthroscopy at baseline, which may have led to a certain therapeutic or placebo effect. The calculated small group size for the conservative group and 20% dropout rate may have led to a lower precision of the results. Also, our intent to treat analysis plan may have led to some bias, especially in the conservative group where 10% underwent HTO or TKA. The authors believe that because of the aforementioned reasons, making direct comparisons between the groups is likely not appropriate. While the primary end point is presented for scientific integrity and transparency, emphasis lies on changes within each group.
Conclusions
OWHTO with plate leads to significant improvement of PRO and function 2 years after intervention and demonstrates reliable mechanical axis correction with subsequent shift of weight-bearing. Medial compartmental OA cases that were treated with OWHTO with plate did not have any conversion to TKA. The PROs of patients in the conservative group showed similar functional improvements without morphological correlate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.